Domestic violence patterns and indicators
Domestic Violence: Patterns and Indicators
Monash University Accident Research Centre - Report #63 - 1994
Authors: J. Sherrard, J. Ozanne-Smith, I. Brumen, V. Routley & F. Williams
Full report in .pdf format [7.6MB]
Abstract:
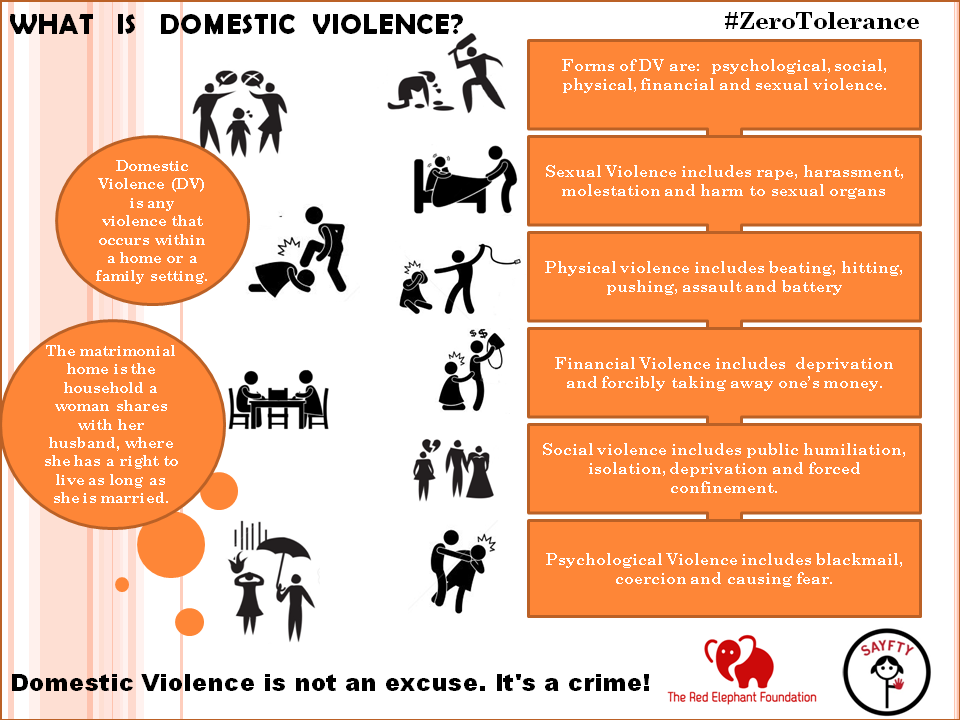
Domestic violence is a substantial intersectoral public health issue, which impacts on the economy, health services, and policing, court and welfare systems. This study aimed to determine the occurrence, patterns and indicators of domestic violence in Victoria using current injury data collection systems, and to explore the barriers to detection of domestic violence victims in hospital emergency departments. The definition of domestic violence used for this study is "partner inflicted injury".
Coroner's data showed that deaths in women due to assault were
more likely to be the result of domestic violence compared with
men, and that 90% of all domestic violence deaths occur in women.
Although a potentially useful source of data, the hospital
admissions injury data set does not allow discrimination between
different categories of assault, with respect to perpetrator, and
therefore cannot be used in its current form to identify domestic
violence victims. Emergency department presentation data showed,
as for deaths, a disproportionate representation of women as
positive victims of domestic violence injury, although, as a
proportion of all injury presentations for women, domestic
violence injury is low (1.3%).
Medical records analysis revealed differences between domestic
violence injury cases and controls including a higher rate of
repeated presentations and admissions to hospital, alcohol abuse,
injuries to the head and trunk, and referral and utilisation of
services by domestic violence victims. Interviews with clinical
staff showed a lack of protocols and training for detecting and
managing domestic violence victims.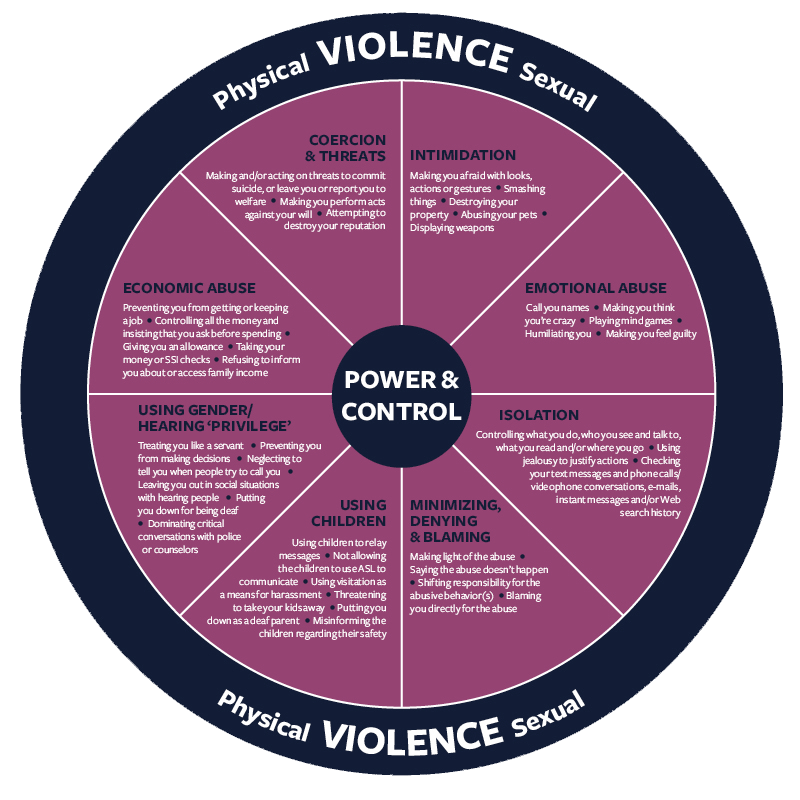
Based on descriptive categories of probable and suggestive cases of domestic violence in emergency department presentation data, a crude estimate of under detection of domestic violence indicated that up to 70% of female domestic violence victims may be missed by hospitals. Our findings also revealed that the proportion of female hospital admissions for self harm or suicide attempt was three times greater than for men, and in some cases was associated with a suggestion of domestic conflict.
Recommendations include improvement in data collection systems, education and training, information and services for domestic violence victims, and future research.
Executive Summary
Domestic violence is a substantial intersectoral public health
problem which impacts on the economy, health services and
policing, court and welfare systems, as well as on the victims
and perpetrators of domestic violence. The recent, strong and
continuing media focus on domestic violence, child abuse, assault
and the issue of gun legislation has increased public attention,
concern and support for action.
Domestic violence appears to be relatively widespread and is reported in the U.S. to be considerably unrecognised by the medical profession. Current research suggests that the Australian experience may reflect that of the United States of America. Domestic violence is specifically identified as a public health issue in 'Goals and Targets for Australia's Health in the Year 2000 and Beyond' (Nutbeam et al., 1993) and a target has been set to reduce morbidity resulting from domestic violence, with women as the priority population.
Although there have been attempts to measure the extent of
domestic violence by the judicial system, the police, the
hospital admissions system and women's refuges, no method is
available to systematically measure the incidence and prevalence
of domestic violence in the wider community. The development of
protocols for improving the identification, treatment and
referral of domestic violence in the hospital setting, and the
establishment of increased services, including those after-hours,
are seen as priorities for reducing the incidence and prevalence
of domestic violence in the community. This report documents a
study of the patterns and indicators of domestic violence, with a
particular focus on injuries.
This report documents a
study of the patterns and indicators of domestic violence, with a
particular focus on injuries.
Literature Review
The major findings of the literature review include;
over-representation of women as victims of domestic violence,
under detection of domestic violence, overuse of medical, health,
psychiatric and social services by victims of domestic violence,
repeated presentations, various barriers to the identification,
management and recording of domestic violence, high rates of
suicide by victims of domestic violence, the cyclical nature of
abuse, the relationship between child and adult victimisation,
history of family violence, and the high incidence of domestic
violence injury during pregnancy. The lack of protocols and
training concerning the identification, management and recording
of domestic violence by professional personnel is also
highlighted. Finally, clarification of definitions, improvements
in baseline data, and identification of risk factors are required
to adequately describe the problem, to identify appropriate
points for intervention, and to evaluate the effectiveness of
preventive measures.
Aims and Objectives
- To determine the occurrence and patterns and indicators of domestic violence in Victoria using current data collection systems.
- To explore the barriers to detection of domestic violence victims in emergency departments with a view to making recommendations for improvements to data collection and management systems and for improving detection levels and services.
- To determine additional alerting characteristics to domestic violence injury, and develop recommendations for their validation.
- To recommend improvements to data collection methodologies to more precisely define and monitor the prevalence of domestic violence
- To develop recommendations for data collection and
systems which Will identify language spoken at home,
aboriginality, country of birth, and any other
demographic risk factors identified by the study.
Methodology
Three approaches to determining the patterns and indicators, and to estimating the frequency of domestic violence (partner inflicted) have been employed for this study. The first is the extraction and analysis of domestic violence injury data from routine injury data currently contained in three data bases. The second is the detailed extraction and analysis of previous histories from medical records of cases identified as domestic violence injury, and from a comparison group, to determine additional patterns and indicators of domestic violence presentation from this source. The third is a survey of clinical staff in hospital emergency departments to determine their level of training in relation to domestic violence issues, and the barriers they perceive to the detection and management of domestic violence victims.
Results
Deaths - Coroner's Facilitation System
Domestic violence injury deaths as a proportion of all injury
death is low (0. 7% in 1991). However, the proportions of
assaultive deaths in women due to domestic violence for the
financial years 1990 and 1991 were 71% and 42% respectively,
whereas the proportions for men were only 3% and 2.4%. Not only
are deaths due to assault in women more likely to be as a result
of domestic violence compared with men, but of all domestic
violence deaths, women are highly over represented (90% of all
domestic violence victims). The use of guns and knives as weapons
of death in domestic violence, in a high proportion of cases,
provides some support for countermeasures aimed at gun and knife
control.
7% in 1991). However, the proportions of
assaultive deaths in women due to domestic violence for the
financial years 1990 and 1991 were 71% and 42% respectively,
whereas the proportions for men were only 3% and 2.4%. Not only
are deaths due to assault in women more likely to be as a result
of domestic violence compared with men, but of all domestic
violence deaths, women are highly over represented (90% of all
domestic violence victims). The use of guns and knives as weapons
of death in domestic violence, in a high proportion of cases,
provides some support for countermeasures aimed at gun and knife
control.
Admissions data - Victorian Inpatient Minimum Database (VIMD)
Males are disproportionably represented in admissions to
hospital for assault, with an overall male to female ratio of
5:1. However, because of the coding system, the proportion of
cases resulting from partner inflicted injury cannot be
discriminated from the database.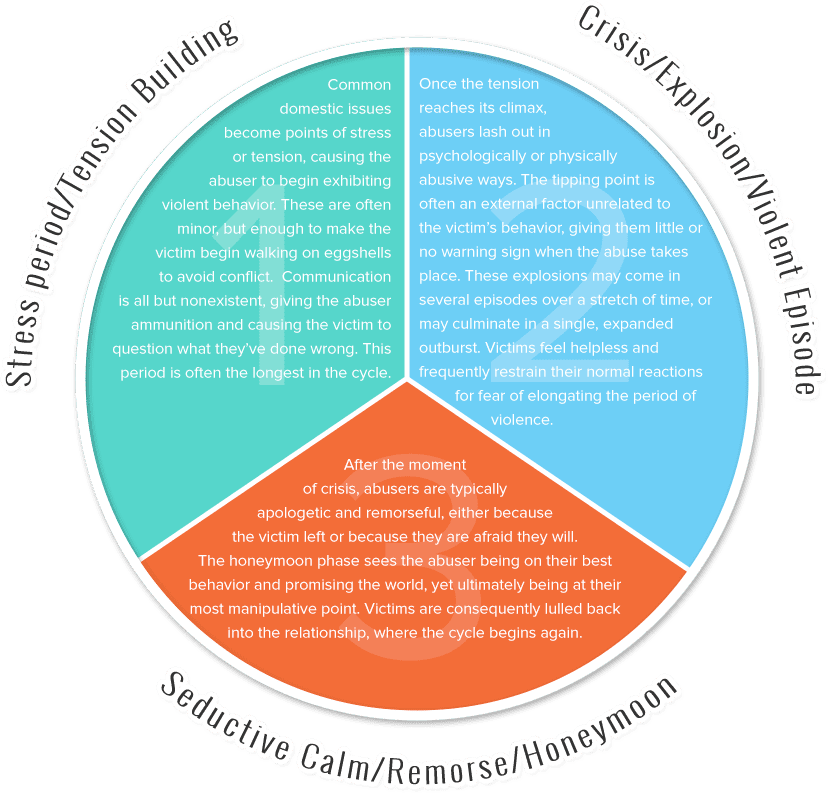 It is clear that VAM in its
current form can offer little useful information on hospital
admissions due to domestic violence. Additional codes in the ICD
database for type of perpetrator in assault cases would clarify
and contribute to information on the nature and extent of
domestic violence cases admitted to hospital.
It is clear that VAM in its
current form can offer little useful information on hospital
admissions due to domestic violence. Additional codes in the ICD
database for type of perpetrator in assault cases would clarify
and contribute to information on the nature and extent of
domestic violence cases admitted to hospital.
Presentation data - Victorian Injury Surveillance System (USS)
The analysis was based on 53,320 cases of adult injury presenting to the emergency departments of five VISS participating hospitals. Following careful screening of the data for cases of domestic violence injury (using the categories of domestic violence injury of Stark and Flitcraft 1981), the final subset consisted of 288 positive cases of partner inflicted domestic violence (83% female), 402 probable cases, 313 suggestive cases, and 52,320 negative cases of domestic violence.
The above findings represent a very small proportion of all
injury presenting to the emergency departments of VISS hospitals,
even combining positives, probables and suggestive, and account
for only 2. 0% of all emergency department presentations. These
results also indicate that of all injury presentations in women,
up to 4.4% may be due to domestic violence.
0% of all emergency department presentations. These
results also indicate that of all injury presentations in women,
up to 4.4% may be due to domestic violence.
Extrapolation, using VISS and VIMD data, gives a very crude estimate that approximately 1 in 200 injury admissions for women are the result of partner inflicted violence. The proportion of female hospital admissions for self harm or suicide attempt was three times greater than for men, and in some cases was associated with a suggestion of domestic violence. Further exploration of this association is warranted.
Analysis of medical records
Data was extracted from the Medical Records of 44 definite
cases of domestic violence and 44 controls (initially selected
from all VISS cases admitted to hospital). Data which could have
provided considerable insight into the circumstances surrounding
some cases of domestic violence were missing from medical
histories.
Females comprised 75% of the victims of domestic violence requiring hospital admission. An overview of the total number of hospital presentations/admissions to the index hospital highlights the repeated use of services by the domestic violence cases. A larger number of domestic violence victims (57%) were recorded as having more than one prior admissions to the index hospital than the controls (36%). Similarly, more victims of domestic violence (57%) were noted as having previous presentations to the index hospital than were the control group (9%).
A number of differences were found between the two groups.
Significant differences were found for involvement of police and
ambulance services, a history of alcohol abuse and current
alcohol abuse, injuries to the head and trunk, referral to a
social worker, and previous non-domestic violence related
presentations or admissions to hospital. This supports the view
that the utilisation of medical services by victims of domestic
violence is generally high.
Interestingly, 20% of the controls (women under 40 years selected from VISS presentations as negative cases of domestic violence) were subsequently found to have a history of suspected abuse when their medical records were examined in detail. The similarity with other studies merits further research using a larger sample of medical records to determine the significance of this result.
Clinical staff interviews
A total of 21 senior doctors and nurses from hospital
Emergency Departments (E.D.) and senior hospital social workers
were interviewed regarding their formal training, both basic and
post-graduate, and attendance at in-service training sessions.
Staff were also asked how many hours overall have been allocated
specifically to domestic violence training, whether they
considered more training necessary and whether they were aware of
their hospital having a policy or protocol for the identification
and management of domestic violence. In sum, the results show a
lack of protocols and education for detecting and managing
victims of domestic violence.
In sum, the results show a
lack of protocols and education for detecting and managing
victims of domestic violence.
Under detection
According to VISS data, the ratio of positive male to female
cases of domestic violence is 1:5. This suggests that 1.3% of
female and 0.14% of male presentations to emergency departments
(0.54 % of all adult presentations) are clearly the result of
partner inflicted injury (positive cases). Thus, injuries in
females presenting to Emergency Departments are 10 times more
likely than those in males to be due to domestic violence. If the
estimate (4%) of new cases from the study by Stark and Flitcraft
(1991) were correct, this result could suggest an under detection
of more than 60% for domestic violence in females. An estimate of
under detection of domestic violence using VISS data on probable
and suggestive cases for females was 70%, although this figure is
likely to be an over estimate due to difficulties in interpreting
case narratives.
Similarly, a crude estimate of under detection can be extrapolated from the analysis of medical records cases. In all, a total of 55 potential controls were selected and 11 (20%) rejected after examination. Although the numbers are very small these figures give a very crude estimate of the potential level of under detection of domestic violence defined in the broader sense (beyond partner inflicted injury). It suggests that up to 1 in 5 admissions for injury in women under 40 years, (after presentation at emergency departments), may be associated with a history of domestic violence, or be self-inflicted injury following a domestic dispute. However this crude estimate should be interpreted with caution.
Recommendations
A number of recommendations are made in relation to data collection systems, education, information and services for domestic violence victims and future research.
(a) Data
1. Standardisation of definitions and terminology of domestic
violence.
Standardisation of definitions and terminology of domestic
violence.
2. Introduction of a locally expanded ICD-9 E-code classification to identify partner inflicted violence.
3. Utilisation of the narrative in the National Minimum Dataset (Injury Surveillance) to identify partner inflicted violence.
4. Investigation of the feasibility of linkage of justice and police databases to give expanded measures of the prevalence of domestic violence
5. Collection of information to identify language spoken at home, aboriginality, country of birth and other demographic variables identified by the study as potential risk factors.
6. Data collection from general practice to determine the prevalence and characteristics of domestic violence presentation to this sector.
(b) Education and Training
7. Development and implementation of policy and strategies for
education and training of health sector personnel for effective
detection and response to domestic violence.
8. Collaboration between Medical, Nursing and other relevant professional bodies to develop hospital protocols for the detection, management and prevention of domestic violence.
9. Evaluation of the effects of training together with protocols in the Emergency Department on detection and recording of domestic violence cases.
(c) Information and Services
10. Establishment of access to domestic violence information for domestic violence victims and perpetrators.
11. Provision of information for hospital staff regarding outside services for domestic violence victims and perpetrators.
12. Determination of the need for increased provision and hours of services in hospitals and increased resources to manage psychosocial and other issues of domestic violence as a result of the increasing detection of victims and their children.
13. Investigation of improved service linkages between
hospital emergency departments, general practice, community based
domestic violence and sexual assault support services.
14. Evaluation of the effectiveness of early intervention services on domestic violence.
(d) Research
15. Estimation of the level of under reporting of domestic violence injuries to the health care system by means of community surveys.
16. Ongoing reviews of successful countermeasures and implementation strategies.
17. Exploration of the role of domestic violence in suicide and attempted suicide and self-harm.
18. Determination of the most effective service provision model for domestic violence victims in crisis.
(e) General
19. Adoption and implementation of the recently developed National and State Strategies for the Prevention and Control of Interpersonal Injury and Suicide.
Sponsor: Department of Health and Community Services, Victoria
Module 2: Indicators of domestic violence
Identification of violence
Indicators
Domestic violence: Frequent radiological findings
Witnesses of domestic violence
Introduction to the topic
Victims who are exposed to domestic violence often originally seek medical attention because of the psychological or physical injuries they suffer. However, they do not often talk about the violence out of shame, fear of being judged or fear of their partner. In order to support the patient, it is important that victims are identified at an early stage and that the violence is disclosed as early as possible.
However, they do not often talk about the violence out of shame, fear of being judged or fear of their partner. In order to support the patient, it is important that victims are identified at an early stage and that the violence is disclosed as early as possible.
Learning objectives
The learning objectives of this module are to become familiar with the various indicators of domestic violence as well as their related risks and to be sensitised to them.
Case study: Disclosure of domestic violence in medical practice
We are in a family practice and a 25-year-old patient comes to a consultation.
Physician: “Good morning Mrs. Schmidt, what can I do for you today?”
Patient: “I feel totally overworked at the moment and wanted to ask if you could put me on sick leave for two weeks?”
Physician: “Is there any particular reason why you feel that way and has this happened before?”
Patient: “I have never been on sick leave because of overload before. But I have just recently separated, and everything just gets too much for me at the moment.”
Physician: “Of course, I can put you on sick leave, but if you feel so overwhelmed by your situation, I would be happy to offer you further support. Perhaps you would like to talk to me about it?”
Patient: “Mmm, I actually feel very uncomfortable to talk about it. There were some problems in my previous relationship. My boyfriend was a control freak and constantly checked my cell phone. We were fighting whenever I wanted to meet with my friends or family. As a result, I became more and more isolated and the only company when leaving the house was my boyfriend. He read messages from my friends before I had a chance to read them. I finally broke up, but I don’t know if that was the right decision.”
Physician: “If your boyfriend controlled and bullied you so much, why do you think the breakup was a mistake?”
Patient: “He keeps calling me and sending me messages. He puts me under pressure by saying that he cannot live without me and will hurt himself if I don’t come back. I see his car in the parking lot all the time: while shopping, being at work or meeting my friends. I always have the feeling that he is around. Can that even be a coincidence? I have already met him twice because I felt so sorry for him, and I was afraid that he would really hurt himself.”
Icon made by Payungkead from www.flaticon.com
Identification of violence
It is important for health service providers to be aware that a victim’s health problems may be caused or made worse by violence. Victims subjected to domestic violence in relationships seek health services for related emotional or physical conditions, including injuries. However, they often do not tell the provider about the violence due to shame or fear of being judged or fear of their partner. To tackle domestic abuse, it is essential that victims are identified and disclose their abuse as early as possible. People experiencing domestic abuse are more likely to come into contact with health services than other public services. As a health professional, you will be a first point of contact for many.
As a health professional, you will be a first point of contact for many.
There is a whole range of indicators to warn health professionals that a patient may be experiencing domestic abuse. Some of these are quite subtle and it is important that professionals remain alert to the potential signs and respond appropriately. Some victims also drop hints in their interactions with health and care staff and their behaviour may also be telling. They rely on staff to listen, persist, and enquire about signs and cues. They need staff to follow up on conversations in private, record details of behaviours, feelings and injuries seen and reported, and support them to take action suitable for their organisation’s systems and local pathways.
Indicators
To improve diagnosis and the subsequent care of patients, health care professionals should always ask about domestic violence when taken the medical history.
Many health settings are busy places, with people passing in and out of cubicles and offices. This is not an appropriate environment to be asking about domestic violence or talking about feelings.
This is not an appropriate environment to be asking about domestic violence or talking about feelings.
Indicators of domestic violence in adults
The following are indicators associated with victims of domestic violence. Please note that none or all of these might be present and be indicators of other issues. Some victims also give hints in conversations, and their behaviour can also be revealing. Victims are therefore dependent on being listened to, on someone being persistent and asking for signs and clues. Using these indicators as a guide can complement the practice of asking directly.
Physical indicators- Unexplained bruising and other injuries
- Especially head, neck, and facial injuries
- Bruises of various ages
- Injuries sustained do not fit the history given
- Bite marks, unusual burns
- Injuries on parts of the body hidden from view (including breasts, abdomen and/or genitals), especially if pregnant
- Chapped lips
- Teeth knocked out
- Miscarriages and other pregnancy complications
- Chronic conditions including headaches, pain and aches in muscles, joints and back
- Sexually transmitted infection and other gynaecological problems
- Emotional distress, e.
 g., anxiety, indecisiveness, confusion, and hostility
g., anxiety, indecisiveness, confusion, and hostility - Sleeping and eating disorders
- Anxiety/depression/pre-natal depression
- Psychosomatic complaints
- Self-harm or suicide attempts
- Evasive or ashamed about injuries
- Seeming anxious in the presence of their partner
- Social isolation/no access to transport
- Frequent absence from work or studies
- Submissive behaviour/low self-esteem
- Alcohol or drug abuse
- Fear of physical contact
- Nervous reactions to physical contact/quick and unexpected movements
- Injuries to the genitals, the inside of the thighs, the breasts, the anus
- Irritations and redness in the genital area
- Common infections in the genital area
- Pain in the lower abdomen and/or pelvic area
- Sexually transmitted diseases
- Bleeding in the vaginal or rectal area
- Pain when urinating or defecating
- Pain when sitting or walking
- Strong fears of examinations in the genital area; avoidance of examinations
- Severe cramps in the vaginal area during gynaecological examinations
- Sexual problems
- Self-harming behaviour
- Unwanted pregnancies/abortions
- Complications during pregnancy
- Miscarriages
Indicators of domestic violence in children
Physical indicators- Difficulty eating/sleeping
- Slow weight gain (in infants)
- Physical complaints
- Eating disorders (including problems of breast feeding)
- Fingertip injuries
- Aggressive behaviour and language
- Depression, anxiety, and/or suicide attempts
- Appearing nervous and withdrawn
- Difficulty adjusting to change
- Regressive behaviour in toddlers
- Delays or problems with language development
- Psychosomatic illness
- Restlessness and problems with concentration
- Dependent, sad, or secretive behaviour
- Bedwetting
- ‘Acting out’, for example cruelty to animals
- Noticeable decline in school performance
- Fighting with peers
- Overprotective or afraid to leave mother or father
- Stealing and social isolation
- Exhibiting sexually abusive behaviour
- Feelings of worthlessness
- Transience
Source: Hegarty (2011): Intimate partner violence – Identification and response in general practice
Factsheet: Indicators of domestic violenceDownload
Domestic violence: Frequent radiological findings
The following description refers to domestic violence against adults in particular (e.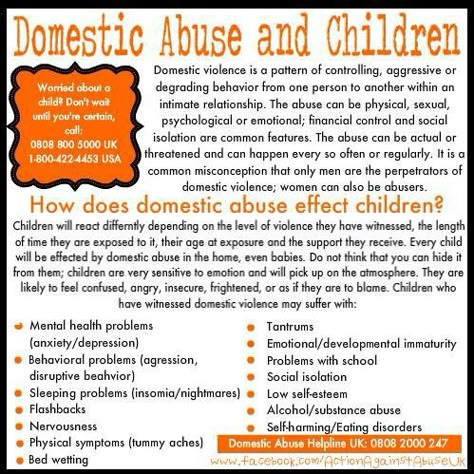 g., partners). A special aspect in the broader context is child abuse – radiological findings may be decisive for its detection.
g., partners). A special aspect in the broader context is child abuse – radiological findings may be decisive for its detection.
- In many cases, victims do not report domestic violence as the cause of an injury or for hospitalisation.
- Medical presentations that do not directly involve an injury can also provide indications of domestic violence.
- Victims of domestic violence receive radiological examinations more often, especially for physical trauma.
- Injuries to the reproductive organs (also during pregnancy, e.g., chorionic hematoma)
- Acute fractures (especially in the facial region, e.g., nasal bone fracture, orbital floor fracture; but also fractures of the extremities)
- Subacute and temporally indeterminate fractures (especially face, extremities, and spine)
- Soft tissue injuries (e.
 g., hematoma and laceration)
g., hematoma and laceration)
- Radiological findings and imaging data contribute to the documentation of the extent of physical injuries.
- However, the injury patterns of adult victims of domestic violence are similar to those of other causes of injury.
- The positive predictive value of a radiological examination alone for the possible presence of domestic violence is limited but can be better assessed and thus increased by considering the overall clinical context.
- This can include injury patterns that do not match the medical history, the presentation of multiple injuries of different ages and frequent radiological examinations in the past.
- The radiologist’s complementary view of the case and the often somewhat calmer situation when preparing and reporting the findings of the examinations (compared to the emergency room) can thus facilitate the detection of domestic violence.

Reference: E. George et al., Radiologic Findings in Intimate Partner Violence. Radiology 2019, 291:62-69
Further Reading: S. Matoori et al. (2020), Intimate partner violence crisis in the COVID-19 pandemic: how can radiologists make a difference? European Radiology
Factsheet: Radiological findingsDownload
Witnesses of domestic violence
Caregivers and family members, but also neighbours or work colleagues can become potential witnesses of domestic violence. The victim’s cooperation and consent are the most important prerequisites for intervening as a witness. An intervention by a witness can include talking to the victim, helping to access help services, or supporting the reporting of domestic violence to the authorities.
Factors that may inhibit or encourage intervention by witnesses
- Witnesses often have a strong desire to intervene, but not necessarily to report domestic violence to the police.
 The possibility to remain anonymous can encourage them to report domestic violence to the authorities.
The possibility to remain anonymous can encourage them to report domestic violence to the authorities. - Understanding domestic violence and knowing how to support victims can motivate witnesses to intervene. This underlines the importance of awareness-raising campaigns that promote understanding and help to identify the signals of domestic violence (especially non-physical violence). They should also provide guidance on how to support victims.
- In the health and social sector, the obligation to report domestic violence is a crucial factor, as witnesses must report domestic violence to the authorities. However, these obligations vary from country to country and the existing conflict between reporting and confidentiality may prevent them from reporting.
- As a rule, witnesses are more inclined to report domestic violence to the authorities if children are involved. If they do not report domestic violence in those cases, it may be because they are worried that the children will be separated from their parents or experience trauma as a result of a police investigation.
- Other factors that may prevent witnesses from intervening are a negative picture of the police and justice system, fear for their own safety and the misunderstanding that domestic violence is a private matter.
Recommendations
- There is a great need for measures that sensitise witnesses and encourage them to act. Further information is needed for professionals who are obliged to report domestic violence.
- It is crucial that police and judicial authorities increase their efforts to deal with reports of domestic violence in a way that protects both, victims and witnesses.
- Further research is needed to ensure that relevant measures to promote and facilitate witness intervention, such as awareness campaigns and helplines/hotlines, are monitored and evaluated to maximise their effectiveness.
More information on the decisive factors for witness intervention in domestic violence can be found here: https://eige.europa.eu/gender-based-violence/eiges-work-gender-based-violence/intimate-partner-violence-and-witness-intervention?lang=sl
Scientific research of the Faculty of Economics.
 Electronic journal. Volume 1. Issue 1.
Electronic journal. Volume 1. Issue 1. Dear reader!
Your attention is invited to a new electronic journal “Scientific research of the Faculty of Economics. Electronic Journal" . It publishes research papers carried out by scientists of Moscow State University and other research institutions and higher educational institutions. The electronic journal contains publications in the form of articles, short messages, reviews on various areas of the economic sphere of society. An important place is given to the materials of discussions and round tables.
The need for such a publication is long overdue and due to the intensity of the scientific life carried out at the Faculty of Economics. Thus, in 2008, researchers and lecturers of the Faculty of Economics of Moscow State University published 737 different papers. At the same time, the total volume of publications increased from 2114 p.p. in 2007 to 2574, 1 p.l. in 2008, i.e. by 22%. 559 articles were published (485 in 2007), with a total volume of 512 pp. (354 pp in 2007). This is almost 45% more than in 2007. The publications published by the Faculty (Bulletin of Moscow State University, the Economics series, Economic Almanac, Philosophy of Economics, etc.) cannot cope with the increased flow of finished manuscripts. But we are talking not only about expanding the possibilities for publishing in a quantitative aspect, but also about creating a qualitatively new multimedia electronic product. This approach is primarily reflected in the content of the journal and its structure. Along with general theoretical sections devoted to the methodological aspects of economic science, mathematical and statistical tools, a significant place is given to specific areas of economics, economic policy issues and economic education. The editorial policy of the journal is focused on the reflection in the articles of the main directions and topics of scientific research conducted at the Faculty of Economics in the context of the problems of world economic science.
(354 pp in 2007). This is almost 45% more than in 2007. The publications published by the Faculty (Bulletin of Moscow State University, the Economics series, Economic Almanac, Philosophy of Economics, etc.) cannot cope with the increased flow of finished manuscripts. But we are talking not only about expanding the possibilities for publishing in a quantitative aspect, but also about creating a qualitatively new multimedia electronic product. This approach is primarily reflected in the content of the journal and its structure. Along with general theoretical sections devoted to the methodological aspects of economic science, mathematical and statistical tools, a significant place is given to specific areas of economics, economic policy issues and economic education. The editorial policy of the journal is focused on the reflection in the articles of the main directions and topics of scientific research conducted at the Faculty of Economics in the context of the problems of world economic science. It is no coincidence that the headings of the journal take into account the names of the modern alphanumeric classification system in economic theory (Journal of Economic Literature). The editorial board of the journal sets itself an ambitious task - to make the journal recognizable among reputable economic publications and known to the world economic community, reflecting the latest achievements of economic science. Therefore, if at the first stage the Russian-language version of the journal is published, accompanied by the translation into English of the titles of articles with a brief annotation and the names of the authors, then at the second stage of the development of the journal, it will become bilingual. The scientific fame of the journal will be facilitated by openness and wide accessibility to the materials published in the journal around the clock. The magazine will be published at least twice a year. To maintain high quality, an examination of all materials will be carried out.
It is no coincidence that the headings of the journal take into account the names of the modern alphanumeric classification system in economic theory (Journal of Economic Literature). The editorial board of the journal sets itself an ambitious task - to make the journal recognizable among reputable economic publications and known to the world economic community, reflecting the latest achievements of economic science. Therefore, if at the first stage the Russian-language version of the journal is published, accompanied by the translation into English of the titles of articles with a brief annotation and the names of the authors, then at the second stage of the development of the journal, it will become bilingual. The scientific fame of the journal will be facilitated by openness and wide accessibility to the materials published in the journal around the clock. The magazine will be published at least twice a year. To maintain high quality, an examination of all materials will be carried out. At least one specialist with a doctorate degree in the specialty of this work can act as a reviewer. World-renowned scientists will be involved in cooperation within the framework of journals in various roles (author, reviewer, member of the editorial board and editorial board), which will also ensure the high quality of published materials.
At least one specialist with a doctorate degree in the specialty of this work can act as a reviewer. World-renowned scientists will be involved in cooperation within the framework of journals in various roles (author, reviewer, member of the editorial board and editorial board), which will also ensure the high quality of published materials.
A distinctive feature of this electronic journal is the efficiency of publishing materials received by the editorial office, since the publishing cycle will consist only of editing, proofreading and electronic preparation of materials. The reader will be able to get acquainted with the latest ideas of modern economic science and thus touch the cutting edge of science.
The activities of the journal are regulated by the Regulations on the scientific electronic journal of the Faculty of Economics of Moscow State University, as well as by regulatory documents and the current legislation of the Russian Federation.
All materials contained in the electronic resources (local and remote access) of the electronic journal are considered published and are subject to copyright.
We invite all interested parties to cooperate.
Dean of the Faculty of Economics, Moscow State University
Kolesov
Contents
Kolesov V.P. Opening speech of the editor-in-chief // Scientific research of the Faculty of Economics. Electronic journal. 2009. No. 1, p. 1-2.
Porohovsky A.A. Market development and political economy // Scientific research of the Faculty of Economics. Electronic journal. 2009. No. 1, p. 3-25.
Shastitko A.E. Clusters as a Discrete Institutional Alternative to Transaction Management // Scientific Research of the Faculty of Economics. Electronic journal. 2009. No. 1, p. 26-43.
Semenov A.L. Specificity of mergers and acquisitions in the Russian Federation. Management approach // Scientific research of the Faculty of Economics. Electronic journal. 2009. No. 1, p. 44-61.
2009. No. 1, p. 44-61.
Kalabikhina I.E., Kozlov V.A. Domestic violence against women in modern Russia: the impact of socio-demographic characteristics of spouses on the prevalence of violence // Scientific research of the Faculty of Economics. Electronic journal. 2009. No. 1, p. 62-84.
Petrin E.V. Actual aspects of determining the effectiveness and efficiency of the marketing department // Scientific research of the Faculty of Economics. Electronic journal. 2009. No. 1, p. 85-94.
Sidorenko V.N. Modeling indicators of development of the Russian energy market // Scientific research of the Faculty of Economics. Electronic journal. 2009. No. 1, p. 95-104.
Kuznetsov B.V., Aleksashenko S.V. Long-term consequences of anti-crisis policy. Dispute club "Knots of economic policy" ANCEA // Scientific research of the Faculty of Economics. Electronic journal. 2009. No. 1, p. 105-126.
What is domestic violence? - Stop Violence
" Violence in the family - intentional actions of the physical, psychological, sexual orientation of one family member in relation to another family member, violating his rights, freedoms, legitimate interests and causing him physical and (or) mental suffering. "
"
" Family members - close relatives, other relatives, disabled dependents and other citizens living together with a citizen and maintaining a common household with him."
Law of the Republic of Belarus "On the basics of crime prevention activities"
When analyzing the phenomenon of domestic violence, it is important to avoid judgments according to which it is appropriate to equate the concepts " conflict " and " situation of violence ". Domestic violence is a recurring pattern of incidents (pattern) of multiple types of violence . The presence of a pattern is an important indicator of the difference between domestic violence and just a conflict situation in the family (Braytseva, E.A. Female Spousal Violence - Nizhny Novgorod, 2008)
Family violence cycle
- Increasing family tension Dissatisfaction in relationships increases and communication between family members is disrupted.
- Violent incident . There is an outburst of verbal, emotional, or physical abuse. Accompanied by rage, arguments, accusations, threats, intimidation.
- Reconciliation . The offender apologizes, explains the reason for the cruelty, shifts the blame to the victim (s), sometimes denies what happened or convinces the victim (s) of exaggerating events.
- Quiet period in relationships ("honeymoon") . The violent incident is forgotten, the offender is forgiven. The phase is called "honeymoon" because the quality of the relationship between partners at this stage returns to the original.
After the "honeymoon" relationship returns to the first stage, and the cycle repeats. As time progresses, each phase becomes shorter, violent outbursts become more frequent and cause more damage. The victim (s) is not able to resolve the situation on her own ( Domestic violence as a problem of modern society. Pazukhina S.V., Fokin I.V., Furtaeva E.I., Tula Institute of Management and Business, Tula ).
Pazukhina S.V., Fokin I.V., Furtaeva E.I., Tula Institute of Management and Business, Tula ).
Domestic violence between partners - any act of violence by an intimate partner, usually on the basis of gender, and causing physical, psychological harm or suffering, as well as threats of such acts, coercion or arbitrary deprivation of liberty, whether in public or private life.
National model of integrated work
with male aggressors in the Republic of Belarus
Partners can be men and women who are both in a registered marriage and in unregistered relationships (cohabitants, young couples, etc.).
Violence between partners can be manifested by both men and women, the only thing that distinguishes them is the type of violence used. However, as practice shows, most often violence is committed by a stronger family member in relation to a weaker one - by a MAN against a WOMAN.
Violence against women - physical, sexual and psychological violence that occurs in the family, including battery, sexual coercion against girls in the family, dowry-related violence, rape of the wife by the husband, mutilation of the female genital organs and others traditional practices that harm women, extramarital violence and exploitative violence.
Declaration on the Elimination of Violence
Against Women (Article 2)
Violence against children dignity of the child, carried out by a person who is with the child in a relationship of responsibility, trust or authority.
World Health Organization
Of course, if we are talking about a family, such authority for a child is its adult members, parents.
Violence against the elderly is any act or omission that harms an older person or puts their health or well-being at risk. The World Health Organization defines elder maltreatment as “the commission of any single or repeated act or failure to act in any trusting relationship that harms or causes distress to the elderly.
Violence against the elderly includes:
- Physical and psychological punishment, treatment as small children, beatings, denial of food or drink, forced feeding, over-medicalization with tranquilizers, failure to comply with adequate doses of medication, bondage, confinement, isolation .
 Denial of hygiene, clothing, decent housing, comfort.
Denial of hygiene, clothing, decent housing, comfort. - Economic exploitation: illegal use of their money or property. Illegal use of unauthorized money checks, signature falsification, theft, etc. Others may suspect something is wrong if the elderly person suddenly changes the balance in the current account, unexpectedly changes his will, transfers large sums to the person who cares for the elderly, or includes him in a bank account as a beneficiary, the disappearance of money or property, the provision of unnecessary services to the elderly and with his explicit complaints of economic violence.
- Also possible is sexual abuse of the elderly, which may become visible to others through bruising or wounds on the chest and genitals; unexplained sexually transmitted diseases; blood stains on underwear; with explicit complaints of an elderly person about sexual abuse.
The appearance of an abused older person may show symptoms of dehydration, malnutrition, neglected bedsores, lack of hygiene, neglected illnesses; an older person may be excitable, frustrated, depressed, aggressive, or directly testify to abuse.