Depressed test nhs
SAMHSA’s National Helpline | SAMHSA
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Main page content
-
SAMHSA’s National Helpline is a free, confidential, 24/7, 365-day-a-year treatment referral and information service (in English and Spanish) for individuals and families facing mental and/or substance use disorders.
Also visit the online treatment locator.
SAMHSA’s National Helpline, 1-800-662-HELP (4357) (also known as the Treatment Referral Routing Service), or TTY: 1-800-487-4889 is a confidential, free, 24-hour-a-day, 365-day-a-year, information service, in English and Spanish, for individuals and family members facing mental and/or substance use disorders.
This service provides referrals to local treatment facilities, support groups, and community-based organizations.
Also visit the online treatment locator, or send your zip code via text message: 435748 (HELP4U) to find help near you. Read more about the HELP4U text messaging service.
The service is open 24/7, 365 days a year.
English and Spanish are available if you select the option to speak with a national representative. Currently, the 435748 (HELP4U) text messaging service is only available in English.
In 2020, the Helpline received 833,598 calls. This is a 27 percent increase from 2019, when the Helpline received a total of 656,953 calls for the year.
The referral service is free of charge. If you have no insurance or are underinsured, we will refer you to your state office, which is responsible for state-funded treatment programs. In addition, we can often refer you to facilities that charge on a sliding fee scale or accept Medicare or Medicaid. If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
The service is confidential. We will not ask you for any personal information. We may ask for your zip code or other pertinent geographic information in order to track calls being routed to other offices or to accurately identify the local resources appropriate to your needs.
No, we do not provide counseling. Trained information specialists answer calls, transfer callers to state services or other appropriate intake centers in their states, and connect them with local assistance and support.
-
Suggested Resources
What Is Substance Abuse Treatment? A Booklet for Families
Created for family members of people with alcohol abuse or drug abuse problems. Answers questions about substance abuse, its symptoms, different types of treatment, and recovery.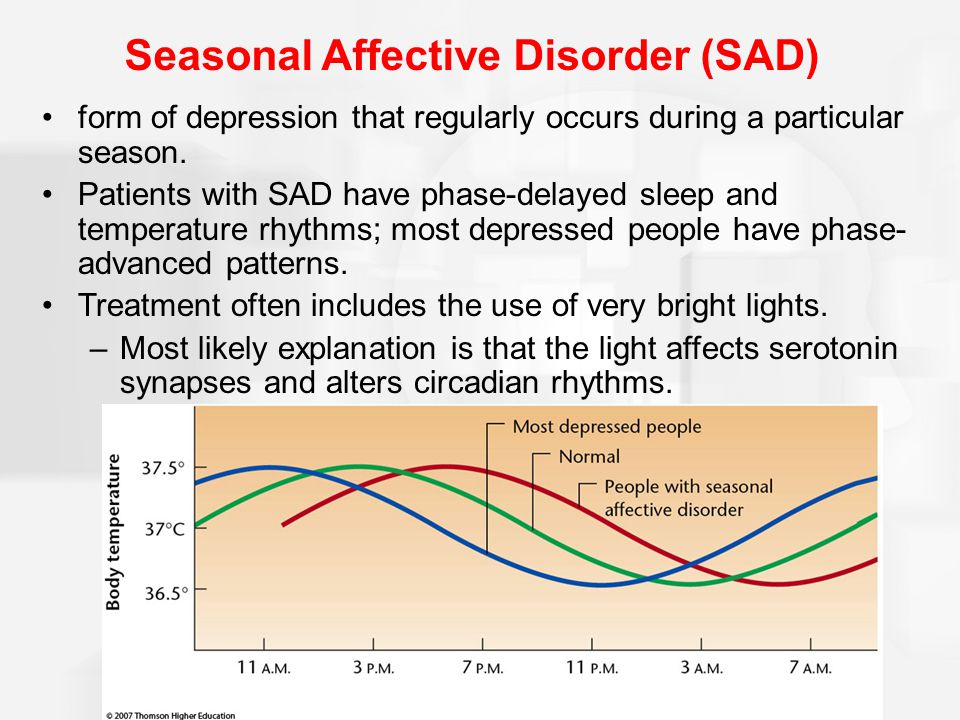 Addresses concerns of children of parents with substance use/abuse problems.
Addresses concerns of children of parents with substance use/abuse problems.It's Not Your Fault (NACoA) (PDF | 12 KB)
Assures teens with parents who abuse alcohol or drugs that, "It's not your fault!" and that they are not alone. Encourages teens to seek emotional support from other adults, school counselors, and youth support groups such as Alateen, and provides a resource list.After an Attempt: A Guide for Taking Care of Your Family Member After Treatment in the Emergency Department
Aids family members in coping with the aftermath of a relative's suicide attempt. Describes the emergency department treatment process, lists questions to ask about follow-up treatment, and describes how to reduce risk and ensure safety at home.Family Therapy Can Help: For People in Recovery From Mental Illness or Addiction
Explores the role of family therapy in recovery from mental illness or substance abuse. Explains how family therapy sessions are run and who conducts them, describes a typical session, and provides information on its effectiveness in recovery.
For additional resources, please visit the SAMHSA Store.
Last Updated: 08/30/2022
SAMHSA Behavioral Health Treatment Services Locator
HomeWelcome to the Behavioral Health Treatment Services Locator, a confidential and anonymous source of information for persons seeking treatment facilities in the United States or U.S. Territories for substance use/addiction and/or mental health problems.
PLEASE NOTE: Your personal information and the search criteria you enter into the Locator is secure and anonymous. SAMHSA does not collect or maintain any information you provide.
Please enter a valid location.
please type your address
-
FindTreatment.
 gov
gov Millions of Americans have a substance use disorder. Find a treatment facility near you.
-
988 Suicide & Crisis Lifeline
Call or text 988
Free and confidential support for people in distress, 24/7.
-
National Helpline
1-800-662-HELP (4357)
Treatment referral and information, 24/7.
-
Disaster Distress Helpline
1-800-985-5990
Immediate crisis counseling related to disasters, 24/7.
- Overview
- Locator OverviewLocator Overview
- Locator OverviewLocator Overview
- Finding Treatment
- Find Facilities for VeteransFind Facilities for Veterans
- Find Facilities for VeteransFind Facilities for Veterans
- Facility Directors
- Register a New FacilityRegister a New Facility
- Register a New FacilityRegister a New Facility
- Other Locator Functionalities
- Download Search ResultsDownload Search Results
- Use Google MapsUse Google Maps
- Print Search ResultsPrint Search Results
- Use Google MapsUse Google Maps
- Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
 Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). - Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). Find programs providing methadone for the treatment of opioid addiction (heroin or pain relievers).
The Locator is authorized by the 21st Century Cures Act (Public Law 114-255, Section 9006; 42 U.S.C. 290bb-36d). SAMHSA endeavors to keep the Locator current. All information in the Locator is updated annually from facility responses to SAMHSA’s National Substance Use and Mental Health Services Survey (N-SUMHSS). New facilities that have completed an abbreviated survey and met all the qualifications are added monthly.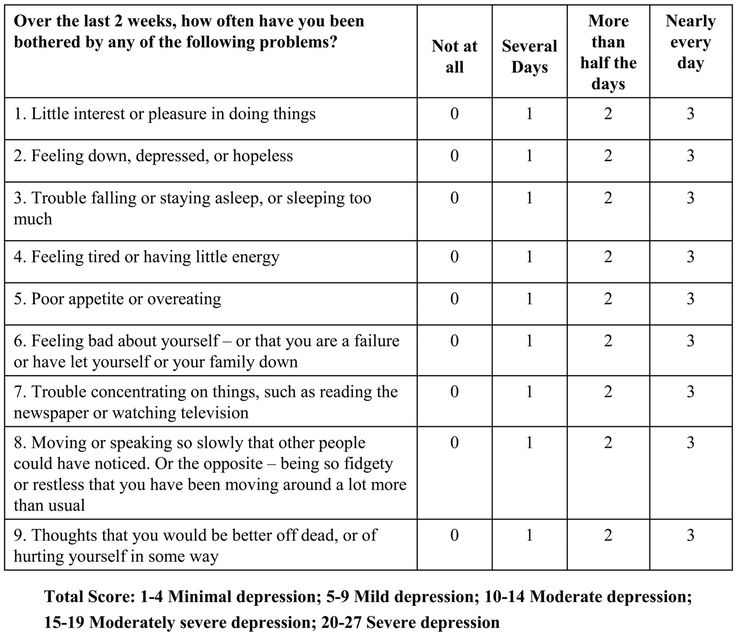 Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Why (and how) you should take a self-test for depression | mental health articles | Emotional & Mental Health center
Depression has always been common, but with the world in turmoil over COVID-19, there are now three times as many people. Could you be depressed without knowing it? Why should you take a self-examination test?
Depression was already one of the most common mental health disorders both in the United States and around the world even before the pandemic, but a new study published in JAMA Network Open finds that depression rates among US adults have tripled since COVID-19.
Now, frankly, it is estimated that despite the fact that we all know that the world is in turmoil, it is still shocking that 27.8% are depressed.
Not surprisingly, people who were more financially insecure and those who had lost loved ones to COVID-19 were more vulnerable to depression. These two risk factors apply to many people, while people with other risk factors or no obvious "reasons" for depression can also become desperate.
The question is, do depressed people know they are clinically depressed? Here's why (and how!) In honor of National Depression Screening Day, everyone should take the time to get self-exams for depression during these turbulent times. nine0003
Why you might be clinically depressed and not know it
Many people seem to view depression as a state of mind in which someone constantly feels sad, tearful, and hopeless almost all the time, although all of these symptoms are indeed present in the diagnostic criteria for major depressive disorder in the Diagnostic and Statistical Manual. mental disorders (DSM-5), that's not all.
mental disorders (DSM-5), that's not all.
Depression can also be manifested by various dominant symptoms. nine0003
You may feel chronically angry, irritable, and impatient, or you may feel bored, pointless, and unmotivated rather than sad. Some people - especially autistic people and people with post-traumatic stress disorder - also have to deal with alexithymia. Alexithymia is a condition in which people are unsure of how they feel or have difficulty labeling their emotions.
All of these factors can make it difficult to recognize your depression, but even if you know you are feeling depressed, you can easily dismiss it as a natural result of stress, not a treatable disease. You may be in denial about the possibility that you have major depressive disorder or one of the other diagnoses that fall under the depressive umbrella, or the idea that you might have clinical depression may simply never cross your mind. nine0003
Why screening tests are important and you should check yourself for depression from time to time
Think of screening as a pre-diagnostic tool that can help identify people at higher risk of the disease so they can move on to more thorough diagnostic testing. In other words, selection programs are like the first round of job interviews, in which employers narrow down the people they want to see again. nine0003
In other words, selection programs are like the first round of job interviews, in which employers narrow down the people they want to see again. nine0003
Screening matters because it allows disease to be detected earlier, even when patients are asymptomatic, or to be freed from them, allowing them sometimes access to life-saving treatment.
Without treatment, depression (obviously) leads to a significant reduction in quality of life. Depression is associated with loss of income, which is itself a risk factor for depression. It can also negatively affect your physical health, increasing your risk of heart disease, stroke, and suicide. nine0003
However, clinical depression is treatable with antidepressants and psychotherapy, often quite effectively. If you are depressed, you want to know about it so that you can get the help you need.
How to self-test for depression
To self-test for clinical depression, you can use the Patient Health Questionnaire (PHQ), a questionnaire to screen for some of the most common mental disorders that has been scientifically proven to give a fairly accurate indication of the likelihood that that the person has a disorder. disorders to which it is directed, as well as the severity of the disease. PHQ-9is the part of this questionnaire specifically for the treatment of major depressive disorder. It is intended for people aged 16 and over.
disorders to which it is directed, as well as the severity of the disease. PHQ-9is the part of this questionnaire specifically for the treatment of major depressive disorder. It is intended for people aged 16 and over.
In PHQ-9 you will think about how often and how severely you have experienced certain emotions and symptoms in the last two weeks. You answer questions on a scale from “not at all” to “almost every day,” and it targets all of the key symptoms of major depression.
How often do you ...
- Have you had no interest or pleasure in your activities in the last couple of weeks? nine0042
- Do you feel overwhelmed, downtrodden or hopeless?
- Did you have trouble falling or staying asleep, or did you oversleep or stay in bed?
- Are you feeling tired and exhausted?
- No appetite, poor appetite or desire to overeat or overeat?
- In the past two weeks, have you felt like you were a failure, let yourself or your family down, or something bad?
- Did you have problems with everyday, normal things? nine0042
- Was physically lethargic, did people notice that you were slower than usual, or vice versa, were you especially restless and restless?
- Were you thinking that you'd be better off dead?
Finally, to what extent have these symptoms and feelings affected your ability to perform your normal duties or interact with people in your life?
These questions are a little more specific and practical than the DSM-5 list for major depressive disorder, and the good news is that you don't even have to take the PHQ-9 screening test yourself. to depression. Online versions that rate this for you are all over the internet. Take this UK NHS version of PHQ-9 for example - and don't be fooled by the fact that it's labeled as a mood self-report.
to depression. Online versions that rate this for you are all over the internet. Take this UK NHS version of PHQ-9 for example - and don't be fooled by the fact that it's labeled as a mood self-report.
A score of 5, 10, 15, and 20, respectively, indicates that you may have mild, moderate, moderately severe, or severe depression, and anything above 5 is a good reason to make an appointment with your family doctor for further diagnosis. . If, like me, you're not a fan of numbers, simply recognizing that you experience a lot of depressive symptoms most of the time is reason enough to do the same. nine0003
Take the results seriously, especially if, after taking a good and honest look at your mood, you find that your depressive symptoms have been bothering you for much longer than two weeks. Although it is normal to feel temporarily depressed and hopeless in objectively stressful circumstances, clinical depression usually does not go away on its own. On the other hand, treatment can save your life in the most severe cases. Other times it will make your life worthwhile again.
Other times it will make your life worthwhile again.
Not English spleen and not Russian blues: how depression is treated in Britain
Loss sculpture by Jane Mortimer in Belfast, Northern Ireland. Photo: unsplash.comDepression is one of the most common mental illnesses worldwide, including the UK. According to statistics, about 17% of the inhabitants of the island (more than 7 million people) take antidepressants. The number of British adults being treated for depression has increased by half a million this year compared to last year, according to recent NHS data. Interestingly, the rates of psychological distress among native Britons are twice as high as those of first-generation immigrants. However, no one is immune from depression: Kommersant UK has prepared a detailed guide on how to recognize depression and where to turn when difficult emotions do not let go. nine0003
What is depression?
Depression, as defined in British textbooks of psychiatry, is a mental state that is long-term, physically and emotionally difficult, characterized by loss of interest in ordinary things, low mood and inability to carry out daily tasks.
The main difference between clinical depression and despondency or just a bad mood is that depression usually lasts for quite a long time and has a serious impact on a person's lifestyle. A depressed person may perceive the most ordinary events negatively, feel acute loneliness and hopelessness, indulge in despair and suicidal thoughts. nine0077 Some patients compare severe depression to a black hole in the soul that cannot be masked or filled with anything. In severe cases, depression can lead to self-harm and suicide.
Causes of depression
Nobody knows exactly what causes depression. One of the most popular theories is the chemical imbalance hypothesis. It is claimed that there are important chemicals in the human brain that regulate mood and state in general. When the balance of chemicals is disturbed, it can lead to depression - the same is observed with hormonal imbalances. nine0003
However, according to a recent study by British scientists from University College London, there is no scientific evidence that a biochemical imbalance in the human brain (low levels of serotonin or decreased activity) causes a depressive state, therefore, when determining the causes of the disease, it is recommended to consider other factors, such as psychological. However, other experts, including scientists from the Royal College of Psychiatrists, disagreed with these findings and urged patients not to stop taking antidepressants, most of which are known to correct abnormally low levels of serotonin. nine0003
However, other experts, including scientists from the Royal College of Psychiatrists, disagreed with these findings and urged patients not to stop taking antidepressants, most of which are known to correct abnormally low levels of serotonin. nine0003
In some cases, depression can be inherited. In addition, various negative life events (family or relationship problems, job loss, etc.) can increase the risk of depression. Lack of exercise and an unhealthy diet, as well as a lack of certain vitamins, plus drug and alcohol consumption, is a sure way to depression. In addition, a history of mild mental illness such as anxiety or phobias, as well as chronic pain from various physical health problems, increase the risk of developing depression. nine0003
Types of depression
Depression can occur in mild, moderate and severe forms (the latter can be a particularly serious condition - psychotic depression).
Psychotic depression (depressive psychosis) is a severe clinical condition in which a depressed person develops hallucinations and delusions, accompanied by depressed mood, as well as restlessness, anxiety, and self-flagellation. According to British scientific studies, about 10-15% of people with severe clinical depression are at risk of developing symptoms of psychosis. A person experiencing psychotic symptoms can be very anxious. It is difficult for him to fall asleep, relax, or just sit still; this condition is called "psychomotor agitation". Another sign of depressive psychosis is a complete detachment from reality: for example, a person with this diagnosis may show symptoms of paranoia and be afraid that others are watching him or reading his thoughts. nine0003
According to British scientific studies, about 10-15% of people with severe clinical depression are at risk of developing symptoms of psychosis. A person experiencing psychotic symptoms can be very anxious. It is difficult for him to fall asleep, relax, or just sit still; this condition is called "psychomotor agitation". Another sign of depressive psychosis is a complete detachment from reality: for example, a person with this diagnosis may show symptoms of paranoia and be afraid that others are watching him or reading his thoughts. nine0003
During pregnancy, so-called prenatal depression can occur in women, and after the birth of a child in the first year after birth, postpartum depression is common (in severe form, it flows into postpartum psychosis). Postpartum depression is a serious mental condition that can last for months (or even longer) and this is different from the so-called baby blues - a short-term (usually observed within two weeks in the mother almost immediately after childbirth) period, which is accompanied by a bad mood, tearfulness, insomnia and feelings of restlessness. The most dangerous form of postpartum depression is postpartum psychosis, a severe mental condition that can occur in a woman in the first weeks after giving birth. One of the features of this condition is deep depressive experiences that affect the life of a woman and her loved ones. nine0003
The most dangerous form of postpartum depression is postpartum psychosis, a severe mental condition that can occur in a woman in the first weeks after giving birth. One of the features of this condition is deep depressive experiences that affect the life of a woman and her loved ones. nine0003
There are also relatively mild types of depression: seasonal affective disorder (SAD; seasonal affective disorder), which appears in a person only at certain times of the year (for example, in winter or autumn), and dysthymia - chronic depression, or depressive neurosis, which can be observed in sluggish form for more than two years.
Where can I get help?
Depression can have a profound effect on life. Various worries and hardships of everyday life in themselves require high energy resources, but when a person is depressed, routine (even simple tasks!) Can become a really difficult test for him. A depressive state in which severely depressed mood and low energy develops can lead to an inability to perform simple tasks, go to work or study, or meet other people. A person suffering from depression may feel empty and guilty, completely losing interest both in things that he used to like and in life in general; his behavior can bring moral and physical suffering to himself and his loved ones. Therefore, timely diagnosis and subsequent treatment of a depressive state are so important. nine0003
A person suffering from depression may feel empty and guilty, completely losing interest both in things that he used to like and in life in general; his behavior can bring moral and physical suffering to himself and his loved ones. Therefore, timely diagnosis and subsequent treatment of a depressive state are so important. nine0003
Regular exercise is recommended for mild depression in the UK. As you know, sports contribute to the production of endorphins (hormones of happiness) and increase energy levels, which is vital for a person suffering from depression. In addition, physical activity helps stimulate appetite and promote healthy sleep. Any kind of physical activity (dancing, swimming or football) can help fight depression. And, surprisingly, simple gardening courses are effective: for example, in London, all people suffering from depression and increased anxiety are offered by the MindFood charity. Classes are held six days a week at two gardens in Ealing. nine0003
GP
If you suspect depression, you should first contact your GP, a general practitioner who can diagnose the disorder, prescribe treatment, recommend psychological therapy (counselling), and connect the patient to the CMHT (Community Mental Health Teams), which supports people with mental problems.
The GP usually prescribes antidepressants when primary treatments for depression (like the aforementioned regular exercise or psychological counseling) do not help. Side effects of some antidepressants include weight gain, anorgasmia, and decreased libido. In addition, in the first weeks, antidepressants can cause severe nausea and panic, so they are selected individually and in combination with other drugs. nine0003
Crisis Services and Charities
Crisis Resolution Services is staffed by doctors and nurses who provide all the support they need for people suffering from depression. They are especially useful in cases where a person prefers to be treated on an outpatient basis rather than in a hospital (for example, mothers of young children usually do not want to part with their babies when they are hospitalized in a psychiatric hospital, and this option may be optimal for them).
The Community Mental Health Team (CMHT) is not only for people with mental health problems, but also for their caregivers. A CMHT team typically includes a Community Psychiatric Nurse (CPN), a psychologist, an occupational therapist, a counselor and social support worker, and a social worker. The coordinator assigns a dedicated staff member who maintains regular contact with their patient and helps plan their treatment. nine0003
A CMHT team typically includes a Community Psychiatric Nurse (CPN), a psychologist, an occupational therapist, a counselor and social support worker, and a social worker. The coordinator assigns a dedicated staff member who maintains regular contact with their patient and helps plan their treatment. nine0003
The charities MIND, Rethink and The Depression Alliance provide helpful information and free counseling for people with any mental health condition (including depression) and their loved ones.
Psychological help / CBT
For mild to moderate depression, psychological help (eg talking therapies / counselling) is recommended.
CBT (Cognitive Behavioral Therapy) - cognitive behavioral therapy as one of the main forms of therapy - is performed for most mental illnesses, including anxiety, phobias and depression. The goal of CBT is to change the negative thoughts (patterns) in the patient's head, thereby directing his attitude towards himself and his perception of the world in a positive direction. nine0003
nine0003
A timely visit to a psychologist is an effective way to combat depression of any form, but with the condition that in moderate and especially severe conditions, psychological therapy alone will still not be enough, and, as a rule, doctors advise combining it with medications or hospitalization ( with depressive psychosis)
How is depressive psychosis treated?
In Britain, a combination of antidepressants and neuroleptics is used to treat psychotic depression: this combination is useful in relieving the symptoms of hallucinations and delusions. In addition to drugs, psychological therapy (Counselling, Talking Therapies) is prescribed. On average, it lasts about a year. nine0003
In some cases, people with psychotic depression may also be placed under the care of CMHT - Community Mental Health Teams. Treatment takes place in the presence of a psychiatrist, social workers and psychiatric nurses at the patient's place of residence.
A separate form of treatment for psychotic depression is electroconvulsive therapy (ECT; Electroconvulsive Therapy), in which an electrical current is passed through the patient's brain. It is effective in treating severe forms of depression, but this type of treatment should only be used when other methods have failed or when the patient's life is at risk (for example, he won't drink or eat). ECT is usually performed in hospitals under general anesthesia. nine0003
It is effective in treating severe forms of depression, but this type of treatment should only be used when other methods have failed or when the patient's life is at risk (for example, he won't drink or eat). ECT is usually performed in hospitals under general anesthesia. nine0003
When is a depressed patient hospitalized?
In Britain, patients with depression are admitted to hospital only in the most serious cases: for example, when a person is diagnosed with psychotic depression or the depression is further exacerbated by the presence of schizophrenia.
However, hospitalization is mostly voluntary. According to the Mental Health Act 1983, involuntary hospitalization can occur when a patient is suffering from a mental disorder and external supervision is necessary for their own interests (to ensure safety) or for the protection of others. nine0003
When a person is at risk of committing suicide or harming others, immediate family members can seek support and request a mental health assessment. A psychiatrist regularly monitors the state of health of the hospitalized in the future.
A psychiatrist regularly monitors the state of health of the hospitalized in the future.
The same applies to postpartum psychosis: if the situation has become too dangerous for the mother or child, she is admitted to a hospital where she can stay with the child, or the mother is referred for outpatient treatment in a clinic where she will be offered medical and psychiatric care. Doctors may recommend that a woman's loved ones take care of her child while she receives the necessary treatment. If she does not have a family or relatives do not provide any support (or are too far away), you can contact the specialized Mother and Baby clinic, whose staff will provide care for both mother and baby. nine0003
Treating depression in the UK and Russia: personal experience
“If in Russia antidepressants are prescribed by psychiatrists, in Britain they can be easily obtained from GPs” : the story of Albina
(names changed. - Note ed.) — About nine years ago, after the death of a close relative, I developed depression, and I turned to psychiatrists for help. Then I lived in Moscow. The doctors prescribed me antidepressants, but, as I now understand, it was a prophylactic dose, so the pills did not help much. nine0003
Then I lived in Moscow. The doctors prescribed me antidepressants, but, as I now understand, it was a prophylactic dose, so the pills did not help much. nine0003
Later, by some miracle, I managed to enroll in a master's program at a British university. Before the move, I started having problems with my appetite: I actually stopped eating, only sometimes I literally stuffed a little food into myself. In this difficult morale, in 2015 I left for the British province and there I went to the GP with complaints of lack of appetite and suspected gastritis. To which the therapist immediately told me: “No, it’s psychological for you, here are pills for depression.” Later, I moved to London, where I was also prescribed antidepressants and did not consider the lack of appetite to be some kind of serious disorder. A couple of months after I complained to the doctors about my suicidal thoughts, I was prescribed eight sessions of talking therapy (talking therapies), but I would not say that this helped, because this time is only enough to establish trust between the psychologist and the patient. nine0003
nine0003
During the coronavirus pandemic, I got even worse: I weighed 45 kg, I was 170 cm tall, and I was still taking antidepressants prescribed by local doctors at a small preventive dose. After two months of taking the pills, I changed them to others, equally ineffective. And by April of this year, I came up in a terrible state: in addition to lack of appetite, I had insomnia. I remembered that certain pills put me into a long and deep sleep, and went to my new GP after moving to Edinburgh to ask for them. I was prescribed them (it was mirtazapine), I took them for two weeks, but again there was no positive effect. Then the doctor decided not to change the pills anymore, but to try to increase the dose three times - and it turned out to be the right decision: I finally started to sleep normally. But during the day, my health remained unimportant, so I was prescribed a second antidepressant, fluoxetine. Moreover, my therapist consulted with a psychiatrist whether it is possible to combine these two types of antidepressants. After that, I began to feel much better: insomnia disappeared, appetite returned. I was surprised by the fact that the lack of appetite was not an indication for serious medical intervention: only insomnia became an important argument for me to be treated. nine0003
After that, I began to feel much better: insomnia disappeared, appetite returned. I was surprised by the fact that the lack of appetite was not an indication for serious medical intervention: only insomnia became an important argument for me to be treated. nine0003
In general, I assess the experience of treating depression equally not very positively, both in the Russian Federation and in the UK. Perhaps in Russia it would be better if I talked with the same doctor for a longer time (in Moscow I changed three specialists), since psychiatrists prescribe antidepressants there - unlike Britain, where the pills are prescribed by GP, then there are general practitioners, and I am skeptical about this, because not all of them consider it necessary to consult with specialized specialists beforehand (as my doctor, with whom I was so lucky in Edinburgh, did). In my opinion, it would be better to prescribe talking therapy before antidepressants come into play, but there are long queues for these sessions (at least several months), and here patients with serious problems are a priority - with drug or alcohol addiction, with severe mental disorders . nine0003
nine0003
There is another important nuance: we, as foreigners, do not have the usual conversational pattern of dialogue with local doctors (it's not even about knowing the language), so the level of trust is not quite the same as at home. Accordingly, it may be difficult for them to understand what treatment immigrants really need.
“Doctors in Russia mistook my depression for VVD”: Victoria's story
— I live between Moscow and London: I have a husband in Britain, close relatives in Moscow. A few years ago, I began to feel psychologically and physically ill, I had insomnia, chronic pain, and a depressed mood. Doctors in Russia only shrugged. They mistook my incipient depression for chronic fatigue and made “favorite” Russian diagnoses: CFS (chronic fatigue syndrome) and VVD (vegetovascular dystonia), advised me to rest more and prescribed only herbs like ginseng and eleutherococcus to increase efficiency. But my working capacity did not increase, rather the opposite. Later in London, I went to the GP and said I suspected depression. I was asked about my symptoms and was prescribed a light dose of antidepressants, which helped me to some extent to work and function normally. nine0003
Later in London, I went to the GP and said I suspected depression. I was asked about my symptoms and was prescribed a light dose of antidepressants, which helped me to some extent to work and function normally. nine0003
After giving birth last year, I developed signs of moderate postpartum depression, and the dose of antidepressants was increased. Now I take these pills constantly, but gradually reduce their dose again, as my health is more or less returning to normal, I began to sleep better and can enjoy simple things more often than before.
Doctors in Britain really take depression seriously, considering it not as something like the blues, but as a disease requiring treatment, and this, in my opinion, is the main difference from Russia (although I may not have been very lucky there with doctors). The British GP also recommended avoiding additional stress and resting more, but his advice did not cancel the use of antidepressants ...
Useful phone numbers and websites for urgent psychological help in the UK:
SOS Silence of Suicide - for everyone.