Bipolar disorder one
Bipolar I Disorder Symptoms, Treatments, Causes, and More
Written by Matthew Hoffman, MD
In this Article
- What Is Bipolar I Disorder?
- Who Is at Risk for Bipolar I Disorder?
- What Are the Symptoms of Bipolar I Disorder?
- What Are the Treatments for Bipolar I Disorder?
- Can Bipolar I Disorder Be Prevented?
- How Is Bipolar I Different From Other Types of Bipolar Disorder?
What Is Bipolar I Disorder?
Bipolar I disorder (pronounced "bipolar one" and also known as manic-depressive disorder or manic depression) is a form of mental illness. A person affected by bipolar I disorder has had at least one manic episode in their life. A manic episode is a period of abnormally elevated or irritable mood and high energy, accompanied by abnormal behavior that disrupts life.
Most people with bipolar I disorder also suffer from episodes of depression. Often, there is a pattern of cycling between mania and depression. This is where the term "manic depression" comes from. In between episodes of mania and depression, many people with bipolar I disorder can live normal lives.
Who Is at Risk for Bipolar I Disorder?
Virtually anyone can develop bipolar I disorder. About 2.5% of the U.S. population suffers from bipolar disorder -- almost 6 million people.
Most people are in their teens or early 20s when symptoms of bipolar disorder first appear. Nearly everyone with bipolar I disorder develops it before age 50. People with an immediate family member who has bipolar are at higher risk.
What Are the Symptoms of Bipolar I Disorder?
During a manic episode in someone with bipolar disorder, elevated mood can manifest itself as either euphoria (feeling "high") or as irritability.
Abnormal behavior during manic episodes includes:
- Flying suddenly from one idea to the next
- Rapid, "pressured" (uninterruptible), and loud speech
- Increased energy, with hyperactivity and a decreased need for sleep
- Inflated self-image
- Excessive spending
- Hypersexuality
- Substance abuse
People in manic episodes may spend money far beyond their means, have sex with people they wouldn't otherwise, or pursue grandiose, unrealistic plans. In severe manic episodes, a person loses touch with reality. They may become delusional and behave bizarrely.
In severe manic episodes, a person loses touch with reality. They may become delusional and behave bizarrely.
Untreated, an episode of mania can last anywhere from a few days to several months. Most commonly, symptoms continue for a few weeks to a few months. Depression may follow shortly after, or not appear for weeks or months.
Many people with bipolar I disorder experience long periods without symptoms in between episodes. A minority has rapid-cycling symptoms of mania and depression, in which they may have distinct periods of mania or depression four or more times within a year. People can also have mood episodes with "mixed features," in which manic and depressive symptoms occur simultaneously, or may alternate from one pole to the other within the same day.
Depressive episodes in bipolar disorder are similar to "regular" clinical depression, with depressed mood, loss of pleasure, low energy and activity, feelings of guilt or worthlessness, and thoughts of suicide. Depressive symptoms of bipolar disorder can last weeks or months, but rarely longer than one year.
Depressive symptoms of bipolar disorder can last weeks or months, but rarely longer than one year.
What Are the Treatments for Bipolar I Disorder?
Manic episodes in bipolar I disorder require treatment with drugs, such as mood stabilizers and antipsychotics, and sometimes sedative-hypnotics which include benzodiazepines such as clonazepam (Klonopin) or lorazepam (Ativan).
Mood Stabilizers
Lithium (Eskalith, Lithobid): This simple metal in pill form is especially effective at controlling mania that involves classical euphoria rather than mixtures of mania and depression simultaneously. Lithium has been used for more than 60 years to treat bipolar disorder. Lithium can take weeks to work fully, making it better for maintenance treatment than for sudden manic episodes. Blood levels of lithium as well as tests to measure kidney and thyroid functioning must be monitored to avoid side effects.
Valproate (Depakote): This antiseizure medication also works to level out moods. It is faster acting than lithium for an acute episode of mania. It is also often used "off label" for prevention of new episodes. As a mood stabilizer that can be used by a "loading dose" method -- beginning at a very high dose -- valproate allows the possibility of significant improvement in mood as early as four to five days.
It is faster acting than lithium for an acute episode of mania. It is also often used "off label" for prevention of new episodes. As a mood stabilizer that can be used by a "loading dose" method -- beginning at a very high dose -- valproate allows the possibility of significant improvement in mood as early as four to five days.
Some other anti-seizure drugs, notably carbamazepine (Tegretol) and lamotrigine (Lamictal), can have value in treating or preventing manias or depressions. Other antiseizure medicines that are less well-established but still sometimes used experimentally for the treatment of bipolar disorder, such as oxcarbazepine (Trileptal).
Antipsychotics
For severe manic episodes, traditional antipsychotics (such as Haldol, Loxapine, or Thorazine) as well as newer antipsychotic drugs -- also called atypical antipsychotics -- may be necessary. Cariprazine (Vraylar) is a newly approved antipsychotic to treat manic or mixed episodes. Aripiprazole (Abilify), asenapine (Saphris), clozapine (Clozaril), lumateperone (Caplyta), olanzapine (Zyprexa), quetiapine (Seroquel), risperidone (Risperdal), and ziprasidone (Geodon) are often used, and many other drugs are available. The antipsychotic lurasidone (Latuda) is approved for use -- either alone or with lithium or valproate (Depakote) -- in cases of bipolar I depression. Antipsychotic medicines are also sometimes used for preventive treatment.
The antipsychotic lurasidone (Latuda) is approved for use -- either alone or with lithium or valproate (Depakote) -- in cases of bipolar I depression. Antipsychotic medicines are also sometimes used for preventive treatment.
Benzodiazepines
This class of drugs, referred to as minor tranquilizers, includes alprazolam (Xanax), diazepam (Valium), and lorazepam (Ativan). They are sometimes used for short-term control of acute symptoms associated with mania such as agitation or insomnia, but they do not treat core mood symptoms such as euphoria or depression. They can also become habit-forming so need to be closely monitored.
Antidepressants
Common antidepressants such as fluoxetine (Prozac), paroxetine (Paxil), and sertraline (Zoloft) have not been shown to be as effective for treating depression in bipolar I disorder as in unipolar depression. In a small percentage of people, they can also set off or worsen a manic episode in a person with bipolar disorder. However, studies have shown that for bipolar II depression, some antidepressants (such as Prozac and Zoloft) may be safe and more helpful than in bipolar I depression. For these reasons, the first-line treatments for depression in bipolar disorder involve medicines that have been shown to have antidepressant properties but also no known risk for causing or worsening mania. The five FDA-approved treatments for bipolar depression are lumateperone (Caplyta), lurasidone (Latuda), olanzapine-fluoxetine (Symbyax) combination, quetiapine (Seroquel) or quetiapine fumarate (Seroquel XR), and cariprazine (Vraylar). Other mood-stabilizing treatments that are sometimes recommended for treating acute bipolar depression include lithium, Depakote, and lamotrigine (Lamictal) (although none of these latter three medicines is FDA-approved specifically for bipolar depression). If these fail, after a few weeks a traditional antidepressant or other medicine may sometimes be added. Psychotherapy, such as cognitive-behavioral therapy, may also help.
However, studies have shown that for bipolar II depression, some antidepressants (such as Prozac and Zoloft) may be safe and more helpful than in bipolar I depression. For these reasons, the first-line treatments for depression in bipolar disorder involve medicines that have been shown to have antidepressant properties but also no known risk for causing or worsening mania. The five FDA-approved treatments for bipolar depression are lumateperone (Caplyta), lurasidone (Latuda), olanzapine-fluoxetine (Symbyax) combination, quetiapine (Seroquel) or quetiapine fumarate (Seroquel XR), and cariprazine (Vraylar). Other mood-stabilizing treatments that are sometimes recommended for treating acute bipolar depression include lithium, Depakote, and lamotrigine (Lamictal) (although none of these latter three medicines is FDA-approved specifically for bipolar depression). If these fail, after a few weeks a traditional antidepressant or other medicine may sometimes be added. Psychotherapy, such as cognitive-behavioral therapy, may also help.
People with bipolar I disorder (mania or depression) have a high risk for recurrences and usually are advised to take medicines on a continuous basis for prevention.
Electroconvulsive Therapy (ECT)
Despite its scary reputation, electroconvulsive therapy (ECT) is a safe and effective treatment for both manic and depressive symptoms. ECT is often used to treat severe forms of depression or mania in bipolar I disorder when medicines may not be effective or likely to work fast enough to bring symptom relief.
Can Bipolar I Disorder Be Prevented?
The causes of bipolar disorder are not well understood. It's not known if bipolar I disorder can be prevented entirely.
It is possible to lower the risk of episodes of mania or depression once bipolar disorder has developed. Regular therapy sessions with a psychologist or social worker can help people to identify factors that can destabilize mood (such as poor medication adherence, sleep deprivation, drug or alcohol abuse, and poor stress management), leading to fewer hospitalizations and feeling better overall. Taking medicine on a regular basis can help to prevent future manic or depressive episodes.
Taking medicine on a regular basis can help to prevent future manic or depressive episodes.
How Is Bipolar I Different From Other Types of Bipolar Disorder?
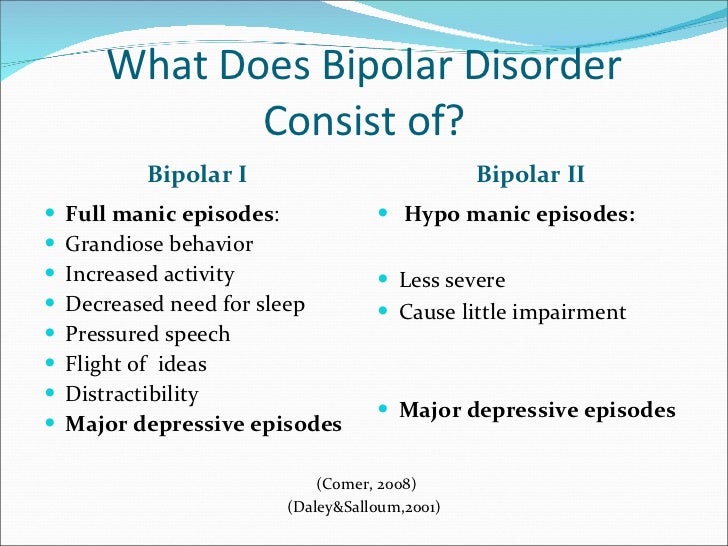
People with bipolar I disorder experience full episodes of mania -- the often severe abnormally elevated mood and behavior described above. These manic symptoms can lead to serious disruptions in life (for example, spending the family fortune, or having an unintended pregnancy).
In bipolar II disorder, the symptoms of elevated mood never reach full-blown mania. They often pass for extreme cheerfulness, even making someone a lot of fun to be around -- the "life of the party." Not so bad, you might think -- except bipolar II disorder usually involves extensive and disabling periods of significant depression, which can often be harder to treat than if episodes of hypomania had never occurred.
Bipolar Disorder Guide
- Overview
- Symptoms & Types
- Treatment & Prevention
- Living & Support
NIMH » Bipolar Disorder
Overview
Bipolar disorder (formerly called manic-depressive illness or manic depression) is a mental illness that causes unusual shifts in mood, energy, activity levels, concentration, and the ability to carry out day-to-day tasks.
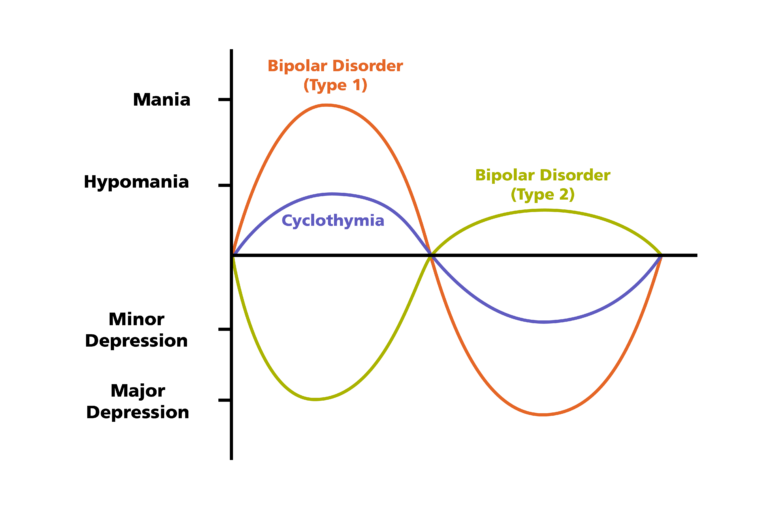
There are three types of bipolar disorder. All three types involve clear changes in mood, energy, and activity levels. These moods range from periods of extremely “up,” elated, irritable, or energized behavior (known as manic episodes) to very “down,” sad, indifferent, or hopeless periods (known as depressive episodes). Less severe manic periods are known as hypomanic episodes.
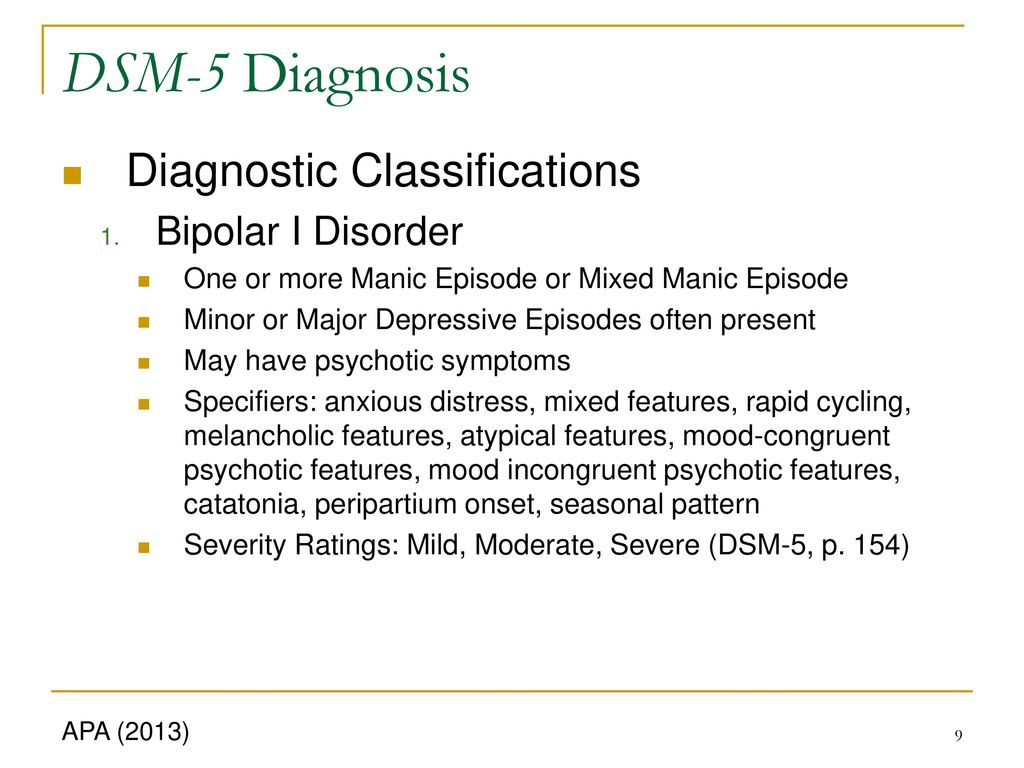
- Bipolar I disorder is defined by manic episodes that last at least 7 days (most of the day, nearly every day) or by manic symptoms that are so severe that the person needs immediate hospital care. Usually, depressive episodes occur as well, typically lasting at least 2 weeks. Episodes of depression with mixed features (having depressive symptoms and manic symptoms at the same time) are also possible. The experience of four or more episodes of mania or depression within a year is termed “rapid cycling.”
- Bipolar II disorder is defined by a pattern of depressive episodes and hypomanic episodes, but the episodes are less severe than the manic episodes in bipolar I disorder.
- Cyclothymic disorder (also called cyclothymia) is defined by recurrent hypomanic and depressive symptoms that are not intense enough or do not last long enough to qualify as hypomanic or depressive episodes.
Sometimes a person might experience symptoms of bipolar disorder that do not match the three categories listed above, and this is referred to as “other specified and unspecified bipolar and related disorders.”
Bipolar disorder is typically diagnosed during late adolescence (teen years) or early adulthood. Occasionally, bipolar symptoms can appear in children. Although the symptoms may vary over time, bipolar disorder usually requires lifelong treatment. Following a prescribed treatment plan can help people manage their symptoms and improve their quality of life.
Signs and Symptoms
People with bipolar disorder experience periods of unusually intense emotion, changes in sleep patterns and activity levels, and uncharacteristic behaviors—often without recognizing their likely harmful or undesirable effects. These distinct periods are called “mood episodes.” Mood episodes are very different from the moods and behaviors that are typical for the person. During an episode, the symptoms last every day for most of the day. Episodes may also last for longer periods, such as several days or weeks.
These distinct periods are called “mood episodes.” Mood episodes are very different from the moods and behaviors that are typical for the person. During an episode, the symptoms last every day for most of the day. Episodes may also last for longer periods, such as several days or weeks.
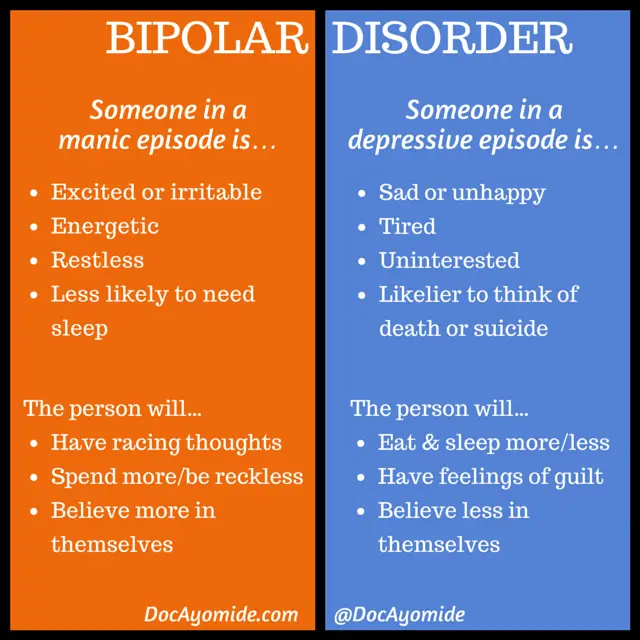
| Symptoms of a Manic Episode | Symptoms of a Depressive Episode |
|---|---|
| Feeling very up, high, elated, or extremely irritable or touchy | Feeling very down or sad, or anxious |
| Feeling jumpy or wired, more active than usual | Feeling slowed down or restless |
| Decreased need for sleep | Trouble falling asleep, waking up too early, or sleeping too much |
| Talking fast about a lot of different things (“flight of ideas”) | Talking very slowly, feeling unable to find anything to say, or forgetting a lot |
| Racing thoughts | Trouble concentrating or making decisions |
| Feeling able to do many things at once without getting tired | Feeling unable to do even simple things |
| Excessive appetite for food, drinking, sex, or other pleasurable activities | Lack of interest in almost all activities |
| Feeling unusually important, talented, or powerful | Feeling hopeless or worthless, or thinking about death or suicide |
Sometimes people experience both manic and depressive symptoms in the same episode, and this is called an episode with mixed features. People experiencing an episode with mixed features may feel very sad, empty, or hopeless while at the same time feeling extremely energized.
People experiencing an episode with mixed features may feel very sad, empty, or hopeless while at the same time feeling extremely energized.
A person may have bipolar disorder even if their symptoms are less extreme. For example, some people with bipolar II disorder experience hypomania, a less severe form of mania. During a hypomanic episode, a person may feel very good, be able to get things done, and keep up with day-to-day life. The person may not feel that anything is wrong, but family and friends may recognize the changes in mood or activity levels as possible bipolar disorder. Without proper treatment, people with hypomania can develop severe mania or depression.
Diagnosis
Proper diagnosis and treatment can help people with bipolar disorder lead healthy and active lives. Talking with a doctor or other licensed health care provider is the first step. The health care provider can complete a physical exam and order necessary medical tests to rule out other conditions. The health care provider may then conduct a mental health evaluation or provide a referral to a trained mental health care provider, such as a psychiatrist, psychologist, or clinical social worker who has experience in diagnosing and treating bipolar disorder.
The health care provider may then conduct a mental health evaluation or provide a referral to a trained mental health care provider, such as a psychiatrist, psychologist, or clinical social worker who has experience in diagnosing and treating bipolar disorder.
Mental health care providers usually diagnose bipolar disorder based on a person’s symptoms, lifetime history, experiences, and, in some cases, family history. Accurate diagnosis in youth is particularly important. You can find tips for talking with your health care provider in NIMH's Tips for Talking With a Health Care Provider About Your Mental Health fact sheet.
Bipolar Disorder and Other Conditions
Many people with bipolar disorder also have other mental disorders or conditions such as anxiety disorders, attention-deficit/hyperactivity disorder (ADHD), misuse of drugs or alcohol, or eating disorders. Sometimes people who have severe manic or depressive episodes also have symptoms of psychosis, such as hallucinations or delusions.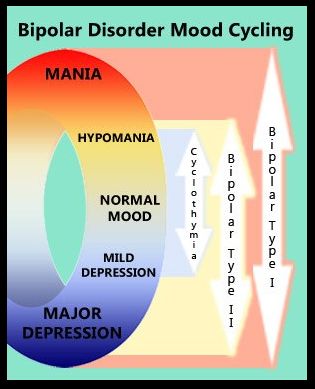 The psychotic symptoms tend to match the person’s extreme mood. For example, someone having psychotic symptoms during a depressive episode may falsely believe they are financially ruined, while someone having psychotic symptoms during a manic episode may falsely believe they are famous or have special powers.
The psychotic symptoms tend to match the person’s extreme mood. For example, someone having psychotic symptoms during a depressive episode may falsely believe they are financially ruined, while someone having psychotic symptoms during a manic episode may falsely believe they are famous or have special powers.
Looking at symptoms over the course of the illness and the person’s family history can help determine whether a person has bipolar disorder along with another disorder.
Risk Factors
Researchers are studying the possible causes of bipolar disorder. Most agree that there is no single cause and it is likely that many factors contribute to a person’s chance of having the illness.
Brain Structure and Functioning: Some studies indicate that the brains of people with bipolar disorder may differ from the brains of people who do not have bipolar disorder or any other mental disorder. Learning more about these differences may help scientists understand bipolar disorder and determine which treatments will work best.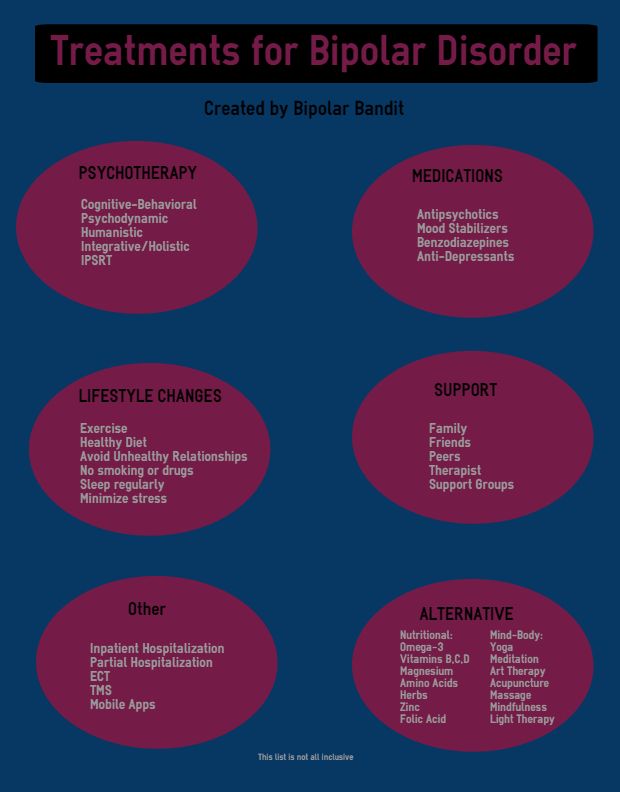 At this time, health care providers base the diagnosis and treatment plan on a person’s symptoms and history, rather than brain imaging or other diagnostic tests.
At this time, health care providers base the diagnosis and treatment plan on a person’s symptoms and history, rather than brain imaging or other diagnostic tests.
Genetics: Some research suggests that people with certain genes are more likely to develop bipolar disorder. Research also shows that people who have a parent or sibling with bipolar disorder have an increased chance of having the disorder themselves. Many genes are involved, and no one gene can cause the disorder. Learning more about how genes play a role in bipolar disorder may help researchers develop new treatments.
Treatments and Therapies
Treatment can help many people, including those with the most severe forms of bipolar disorder. An effective treatment plan usually includes a combination of medication and psychotherapy, also called talk therapy.
Bipolar disorder is a lifelong illness. Episodes of mania and depression typically come back over time. Between episodes, many people with bipolar disorder are free of mood changes, but some people may have lingering symptoms. Long-term, continuous treatment can help people manage these symptoms.
Long-term, continuous treatment can help people manage these symptoms.
Medications
Certain medications can help manage symptoms of bipolar disorder. Some people may need to try several different medications and work with their health care provider before finding medications that work best.
The most common types of medications that doctors prescribe include mood stabilizers and atypical antipsychotics. Mood stabilizers such as lithium or valproate can help prevent mood episodes or reduce their severity. Lithium also can decrease the risk of suicide. Medications that target sleep or anxiety are sometimes added to mood stabilizers as part of a treatment plan.
While bipolar depression is often treated with antidepressant medication, a mood stabilizer must be taken as well, as an antidepressant alone can trigger a manic episode or rapid cycling in a person with bipolar disorder. Because people with bipolar disorder are more likely to seek help when they are depressed than when they are experiencing mania or hypomania, taking a careful medical history is essential to ensure that bipolar disorder is not mistaken for depression.
People taking medication should:
- Talk with their health care provider to understand the risks and benefits of the medication.
- Tell their health care provider about any prescription drugs, over-the-counter medications, or supplements they are already taking.
- Report any concerns about side effects to a health care provider right away. The health care provider may need to change the dose or try a different medication.
- Remember that medication for bipolar disorder must be taken consistently, as prescribed, even when one is feeling well.
Avoid stopping a medication without talking to a health care provider first. Suddenly stopping a medication may lead to a “rebound” or worsening of bipolar disorder symptoms. For basic information about medications, visit NIMH's Mental Health Medications webpage. Read the latest medication warnings, patient medication guides, and information on newly approved medications on the Food and Drug Administration (FDA) website.![]()
Psychotherapy
Psychotherapy, also called talk therapy, can be an effective part of the treatment plan for people with bipolar disorder. Psychotherapy is a term for a variety of treatment techniques that aim to help a person identify and change troubling emotions, thoughts, and behaviors. It can provide support, education, and guidance to people with bipolar disorder and their families.
Cognitive behavioral therapy (CBT) is an important treatment for depression, and CBT adapted for the treatment of insomnia can be especially helpful as a component of the treatment of bipolar depression.
Treatment may also include newer therapies designed specifically for the treatment of bipolar disorder, including interpersonal and social rhythm therapy (IPSRT) and family-focused therapy. Determining whether intensive psychotherapeutic intervention at the earliest stages of bipolar disorder can prevent or limit its full-blown onset is an important area of ongoing research.
Visit NIMH's Psychotherapies webpage to learn about the various types of psychotherapies.
Other Treatment Options
Some people may find other treatments helpful in managing their bipolar symptoms, including:
- Electroconvulsive therapy (ECT) is a brain stimulation procedure that can help relieve severe symptoms of bipolar disorder. ECT is usually only considered if an individual’s illness has not improved after other treatments such as medication or psychotherapy, or in cases that require rapid response, such as with suicide risk or catatonia (a state of unresponsiveness).
- Transcranial magnetic stimulation (TMS) is a type of brain stimulation that uses magnetic waves, rather than the electrical stimulus of ECT, to relieve depression over a series of treatment sessions. Although not as powerful as ECT, TMS does not require general anesthesia and presents little risk of memory or adverse cognitive effects.
- Light therapy is the best evidence-based treatment for seasonal affective disorder (SAD), and many people with bipolar disorder experience seasonal worsening of depression in the winter, in some cases to the point of SAD.
 Light therapy could also be considered for lesser forms of seasonal worsening of bipolar depression.
Light therapy could also be considered for lesser forms of seasonal worsening of bipolar depression.
Unlike specific psychotherapy and medication treatments that are scientifically proven to improve bipolar disorder symptoms, complementary health approaches for bipolar disorder, such as natural products, are not based on current knowledge or evidence. For more information, visit the National Center for Complementary and Integrative Health website.
Finding Treatment
- A family health care provider or doctor is a good resource and can be the first stop in searching for help. For tips for talking with your health care provider, see NIMH’s Tips for Talking With a Health Care Provider About Your Mental Health fact sheet.
- For general information on mental health and to find local treatment services, call the Substance Abuse and Mental Health Services Administration (SAMHSA) Treatment Referral Helpline at 1-800-662-HELP (4357).
- The SAMHSA website has a Behavioral Health Treatment Services Locator that can search for treatment information by address, city, or ZIP code.
- Visit NIMH’s Help for Mental Illnesses webpage for more information and resources.
If you or someone you know is in immediate distress or is thinking about hurting themselves, call or text the 988 Suicide & Crisis Lifeline at 988 or chat at 988lifeline.org. You can also contact the Crisis Text Line (text HELLO to 741741). For medical emergencies, call 911.
Coping with Bipolar Disorder
Living with bipolar disorder can be challenging, but there are ways to help make it easier for yourself, a friend, or a loved one.
- Get treatment and stick with it. Treatment is the best way to start feeling better.
- Keep medical and therapy appointments and talk with your health care provider about treatment options.
- Take medication as directed.
- Structure activities. Keep a routine for eating, sleeping, and exercising.
- Try regular, vigorous exercise like jogging, swimming, or bicycling, which can help with depression and anxiety, promote better sleep, and is healthy for your heart and brain.
- Keep a life chart to help recognize your mood swings.
- Ask for help when trying to stick with your treatment.
- Be patient. Improvement takes time. Social support helps.
Remember, bipolar disorder is a lifelong illness, but long-term, ongoing treatment can help control symptoms and enable you to live a healthy life.
Join a Study
Clinical trials are research studies that look at new ways to prevent, detect, or treat diseases and conditions. The goal of clinical trials is to determine if a new test or treatment works and is safe. Although individuals may benefit from being part of a clinical trial, participants should be aware that the primary purpose of a clinical trial is to gain new scientific knowledge so that others may be better helped in the future.
Researchers at NIMH and around the country conduct many studies with patients and healthy volunteers. We have new and better treatment options today because of what clinical trials uncovered years ago. Be part of tomorrow’s medical breakthroughs. Talk to your health care provider about clinical trials, their benefits and risks, and whether one is right for you.
Be part of tomorrow’s medical breakthroughs. Talk to your health care provider about clinical trials, their benefits and risks, and whether one is right for you.
To learn more or find a study, visit:
- NIMH’s Clinical Trials webpage: Information about participating in clinical trials
- Clinicaltrials.gov: Current Studies on Bipolar Disorder: List of clinical trials funded by the National Institutes of Health (NIH) being conducted across the country
- Join a Study: Bipolar Disorder – Adults: List of studies being conducted on the NIH Campus in Bethesda, MD
Learn More
Free Brochures and Shareable Resources
- Bipolar Disorder: A brochure on bipolar disorder that offers basic information on signs and symptoms, treatment, and finding help. Also available en español.
- Bipolar Disorder in Children and Teens: A brochure on bipolar disorder in children and teens that offers basic information on signs and symptoms, treatment, and finding help.
 Also available en español.
Also available en español. - Bipolar Disorder in Teens and Young Adults: Know the Signs: An infographic presenting common signs and symptoms of bipolar disorder in teens and young adults. Also available en español.
- Shareable Resources on Bipolar Disorder: Help support bipolar disorder awareness and education in your community. Use these digital resources, including graphics and messages, to spread the word about bipolar disorder.
Multimedia
- Mental Health Minute: Bipolar Disorder in Adults: Take a mental health minute to learn about bipolar disorder in adults.
- NIMH Expert Discusses Bipolar Disorder in Adolescents and Young Adults: Learn the signs, symptoms, and treatments of bipolar disorder.
Research and Statistics
- Journal Articles: This webpage provides information on references and abstracts from MEDLINE/PubMed (National Library of Medicine).
- Treatment for Bipolar Disorder in Adults: A Systematic Review: A review from the Agency for Healthcare Research and Quality that assesses the effectiveness of medications and other therapies for treating mania or depression symptoms and preventing relapse in adults with bipolar disorder diagnoses.
- Bipolar Disorder Statistics: An NIMH webpage that provides information on the prevalence of bipolar disorder among adults and adolescents.
Last Reviewed: September 2022
Unless otherwise specified, NIMH information and publications are in the public domain and available for use free of charge. Citation of NIMH is appreciated. Please see our Citing NIMH Information and Publications page for more information.
Bipolar affective disorder (BAD), its signs, types and methods of treatment
Manifestations of various emotions, a change in a person's mood, manifestations of both sadness and joy are normal and depend on many factors - from temperament and character to ongoing events that influence from the outside. However, when these changes are excessive, often unexpected and for no apparent reason, emotions get out of control, or a person remains in a radically positive or negative mood for a long time, it is very likely that bipolar disorder can be diagnosed. This disease was first described at the end of 19century, the famous German psychiatrist Emil Kripelin, calling it manic-depressive psychosis. Many world famous personalities such as Vincent van Gogh, Isaac Newton, Ludwig van Beethoven, Abraham Lincoln suffered from this disease. The pronounced form of this disease, which in the international classification of diseases is called bipolar affective disorder (BAD), is detected in 3% of the world's population.
However, when these changes are excessive, often unexpected and for no apparent reason, emotions get out of control, or a person remains in a radically positive or negative mood for a long time, it is very likely that bipolar disorder can be diagnosed. This disease was first described at the end of 19century, the famous German psychiatrist Emil Kripelin, calling it manic-depressive psychosis. Many world famous personalities such as Vincent van Gogh, Isaac Newton, Ludwig van Beethoven, Abraham Lincoln suffered from this disease. The pronounced form of this disease, which in the international classification of diseases is called bipolar affective disorder (BAD), is detected in 3% of the world's population.
TABLE OF CONTENTS
- 1. Bipolar Personality Disorder - Overview
- 2. Symptoms and signs
- 3. Types of bipolar disorder
- 4. Phases of Bipolar Disorder
- 5. Bipolar disorder in women
- 6. Treatment of Bipolar Personality Disorder
It is not uncommon for women to be treated with a combination of drug therapy and cognitive behavioral or interpersonal therapy with a psychotherapist.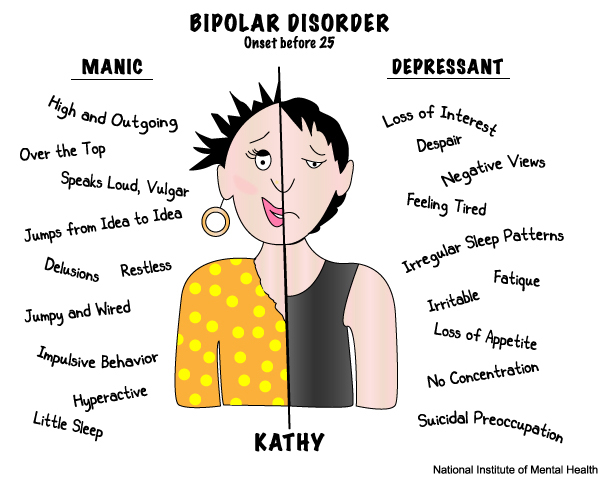
Bipolar personality disorder - general information
According to statistics, bipolar disorder affects people between 14 and 44 years of age. Unlike adults, children and adolescents experience more frequent mood swings from mania to depression, sometimes several times a day. 90% of young people make their debut precisely from the phase of depression or melancholy. Another feature of bipolar disorder is that, due to the low level of diagnosis, the patient can live with this disease for 5-10 years without knowing the cause of the painful symptoms.
Most often, bipolar disorder is diagnosed in people whose immediate family members have had a similar problem. The causes of this disease are unknown, but stress, overstrain, and various diseases can provoke the manifestation of its symptoms. However, having fenced off a person from the influence of these factors, it is impossible to get rid of the problem, you need to seek help from a psychotherapist.
Bipolar disorder is a disease that cannot be completely cured.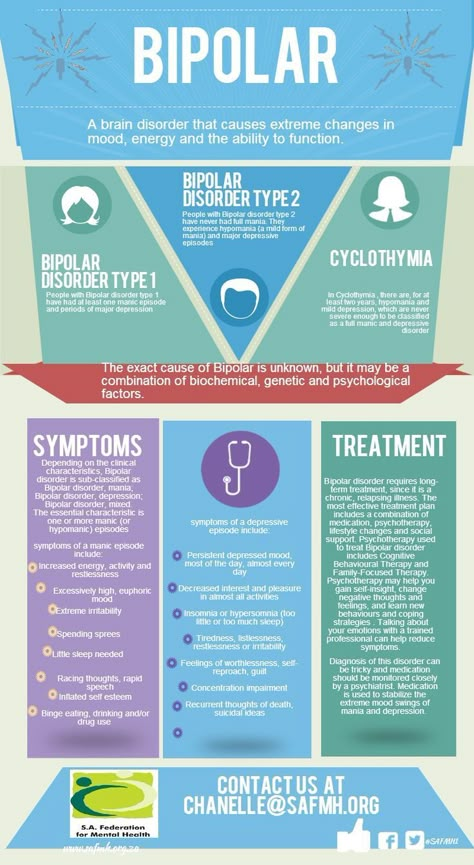 But with properly selected medication and psychotherapy, the quality of life is significantly improved and the periods between phases are lengthened. The person remains socialized and able to work.
But with properly selected medication and psychotherapy, the quality of life is significantly improved and the periods between phases are lengthened. The person remains socialized and able to work.
Symptoms and signs
From the name it is clear that we are talking about two different poles of affective manifestations, that is, mood manifestations. One of these conditions is depression. Depression in bipolar disorder is pronounced, with vivid symptoms. It can last up to a year and is manifested not only by low mood, lack of ability to enjoy and interest in ongoing events, but also by psychosis, when ideas of self-accusation arise, the patient feels inferior, unnecessary, poisoning the life of others. There are also nihilistic thoughts about suffering from some kind of severe illness, despite medical evidence to the contrary. There may be delusional thoughts, as well as suicidal thoughts and even attempts.
The other pole of bipolar disorder is a hypomanic state or hypomania, the characteristic features of which are an increased euphoric emotional background, the patient is constantly on the move, hyperactive, and is distinguished by very fast, associative speech.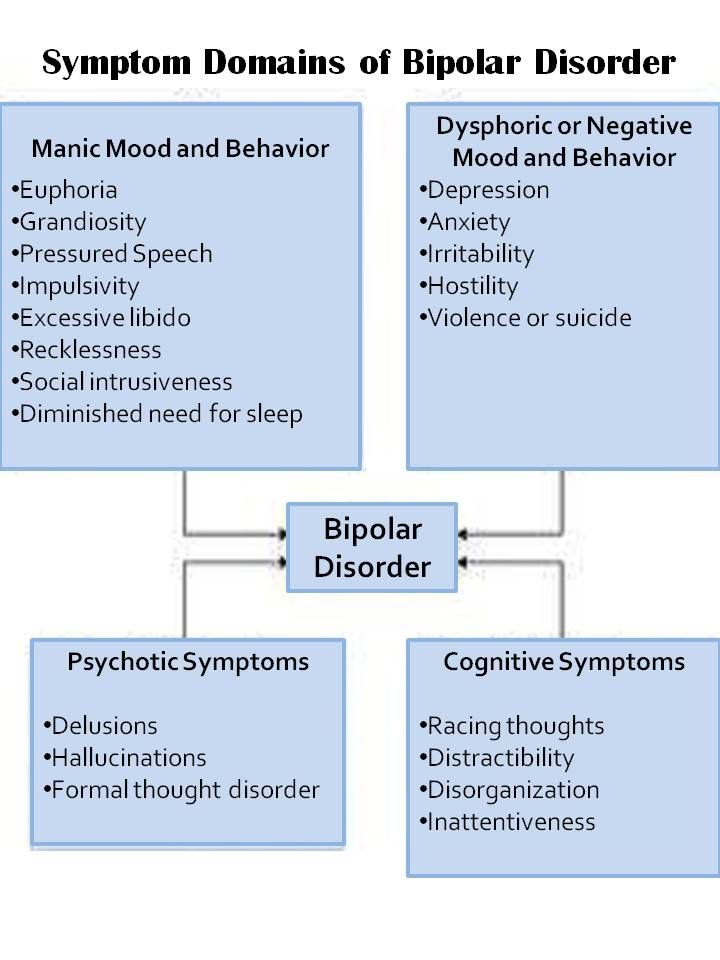 The patient is constantly cheerful, often hypersexual, almost always awake or sleeping 2-3 hours a day.
The patient is constantly cheerful, often hypersexual, almost always awake or sleeping 2-3 hours a day.
Hypomania is often followed by a manic bipolar state with psychotic manifestations. The patient develops convictions in his own greatness, he believes that he is capable of anything, feels that he has a special calling in this world or that he is a descendant of great people. In extended manic episodes of mania with psychotic manifestations, anger, irritability, and direct aggression often occur. This condition leads the patient into extremely unpleasant and sometimes dangerous situations.
In addition to the typical symptoms of the disease, there are a large number of comorbid mental disorders. Comorbid mental disorders are those that accompany the underlying disease. The most common disorder of this kind is anxiety, which is manifested, among other things, by nonspecific autonomic symptoms, including sweating, palpitations, tremors of the limbs, various disorders of the gastrointestinal tract, dizziness, headaches, suffocation, and many others. In the case when these symptoms occur suddenly, mainly in public places, they are called panic attacks.
In the case when these symptoms occur suddenly, mainly in public places, they are called panic attacks.
Types of Bipolar Disorder
Bipolar disorder can be Ι and ΙΙ types.
Bipolar I disorder is a condition in which the patient has persistent manias, i.e. overexcitation, enthusiastic inappropriate behavior, manic psychosis, as well as severe depressions. Symptoms of this type are more severe, so hospitalization is indicated in most cases.
Bipolar I disorder is characterized by short periods of hypomania followed by periods of deep depression. Hypomania is a pre-manic state with less active manifestations. Hypomania lasts a very short period of time - from several days to several hours, so sometimes patients do not even notice them and do not inform the doctor about it. Only careful, painstaking work with the patient makes it possible to identify hypomania, make the correct diagnosis and prescribe treatment.
Phases of bipolar disorder
There are several phases of bipolar personality disorder:
- Depressive (unipolar depression).
 People experience a depressed mood, despair and despondency, complain of a lack of energy and mental concentration, they can either eat too much or too little and sleep.
People experience a depressed mood, despair and despondency, complain of a lack of energy and mental concentration, they can either eat too much or too little and sleep.
Depersonalization and derealization may occur at the peak of bipolar depressive disorder. The boundaries of their own "I" and the world around them become blurred, patients experience difficulties in perceiving what is happening. Familiar places seem new, the colors of the surrounding world change, the patient constantly experiences a feeling of "déjà vu". Sounds become muffled, even if someone is talking very close, it seems to the patient that the voice is coming from afar.
- Manic (hypomanic). In this state, patients are full of energy, overly happy or optimistic, euphoric, and have extremely high self-esteem. At first glance, these are positive signs, but when a person experiences large-scale manic episodes, these symptoms and such an emotional state can reach dangerous extremes.
 A patient in this phase may indiscriminately spend huge amounts of money or behave carelessly, not realizing the full danger. In conversation, people may choke on words, speak at a high speed, or jump from one thought to another. These episodes may also be accompanied by delusions of grandeur or the adoption of serious decisions without thinking about the further consequences.
A patient in this phase may indiscriminately spend huge amounts of money or behave carelessly, not realizing the full danger. In conversation, people may choke on words, speak at a high speed, or jump from one thought to another. These episodes may also be accompanied by delusions of grandeur or the adoption of serious decisions without thinking about the further consequences.
In the development of the manic phase, the following stages of development can be distinguished:
- Hypomania - increased excitement, emotional upsurge.
- Mania - all signs are more pronounced, aggression, irritability, irascibility and rage are possible.
- Phase peak. The patient constantly experiences nervous excitement, he cannot relax. All his emotions are "heated" to the limit, coordination of movements is disturbed, thoughts are illogical and abrupt, in speech he constantly jumps from one sentence to another.
- Relief of symptoms. The patient gradually calms down.
 Movement disorders are on the decline. The speed of thinking and increased emotional mood remain unchanged.
Movement disorders are on the decline. The speed of thinking and increased emotional mood remain unchanged. - Return to normal.
- Mixed. Sometimes people have complaints that are characteristic of both depression and mania at the same time. They may also experience frequent phasing—4 or more episodes in one year.
In the intervals between depressive and manic phases in bipolar disorder, there is a light period during which the general background of mood becomes relatively stable, the person continues to adequately respond to certain events, the emotional sphere is under his control. This is the main criterion for remission of bipolar disease.
Bipolar disorder in women
According to statistics, bipolar Ι disorder occurs with the same frequency in men and women, and type ΙΙ disease is more often diagnosed in women. It is also known that the female course of the disease is characterized by rapid cycles and mixed episodes. Comorbidities often include eating disorders, borderline personality disorder, alcohol or drug addiction, and psychotropic drug abuse. Women are more susceptible to such somatic diseases as migraine (intense headaches), thyroid pathologies, diabetes, and obesity.
Comorbidities often include eating disorders, borderline personality disorder, alcohol or drug addiction, and psychotropic drug abuse. Women are more susceptible to such somatic diseases as migraine (intense headaches), thyroid pathologies, diabetes, and obesity.
For women, a special technique is being developed to alleviate this disorder, since from adolescence to menopause there are specific changes in hormonal levels that must be taken into account. In addition, psychotropic substances, which are supposed to stabilize the condition, can adversely affect the intrauterine development of the fetus if the woman is in position. It is noted that in the first trimester of pregnancy this disorder is milder, but after childbirth they often have to deal with postpartum depression. Thus, at each stage of the development of the female body, a competent doctor must review and adjust the treatment regimen. Often in the treatment of women, a complex method is used that combines drug therapy and cognitive-behavioral or interpersonal therapy with a psychotherapist. This approach gives the fastest results.
This approach gives the fastest results.
Treatment for bipolar disorder
Attempts to get rid of bipolar disorder on your own do not bring the desired result and, ultimately, lead to an aggravation of the situation, including the development of drug or alcohol dependence. In the diagnosis of the disease, keeping a mood diary can help, where the patient records all his thoughts, emotions, feelings, changes in mood. Such records will help the doctor to assess the mental state in detail and make the correct diagnosis. If you suspect bipolar disorder, you should consult a doctor, and the sooner a person realizes that he has a disease and comes to the clinic for help, the sooner professional help will be provided to him and painful symptoms will be replaced by a stable condition. It is impossible to get rid of the disease on your own, since a person cannot fully adequately assess not only his actions, but also the alternation of the phases of the disease.
Bipolar disorder is one of the few mental disorders in which medication is indicated in 100% of cases, and psychotherapy is an auxiliary tool. This disease is incurable, but its diagnosis and treatment is extremely important. Treatment can reduce the number of episodes, their severity and intensity, as well as prevent negative life events, help prevent relationship breakups, job loss, and even suicidal attempts. Thus, the quality of life of a patient with bipolar disorder who is undergoing treatment will be several times higher than that of a person who neglects treatment. If the patient loses touch with reality and harms himself and others, he is subject to hospitalization, outpatient treatment in this case is not permissible.
This disease is incurable, but its diagnosis and treatment is extremely important. Treatment can reduce the number of episodes, their severity and intensity, as well as prevent negative life events, help prevent relationship breakups, job loss, and even suicidal attempts. Thus, the quality of life of a patient with bipolar disorder who is undergoing treatment will be several times higher than that of a person who neglects treatment. If the patient loses touch with reality and harms himself and others, he is subject to hospitalization, outpatient treatment in this case is not permissible.
If you have a disease, it is recommended to exclude coffee, strong tea, alcoholic and energy drinks from your diet in order not to provoke an overexcited state. If possible, you should stop smoking and in no case should you take even soft drugs. It is also very important to establish a sleep pattern, sleep at least 8 hours a day and try to go to bed at about the same time. You should learn to recognize mood swings and notice the early manifestations of new episodes.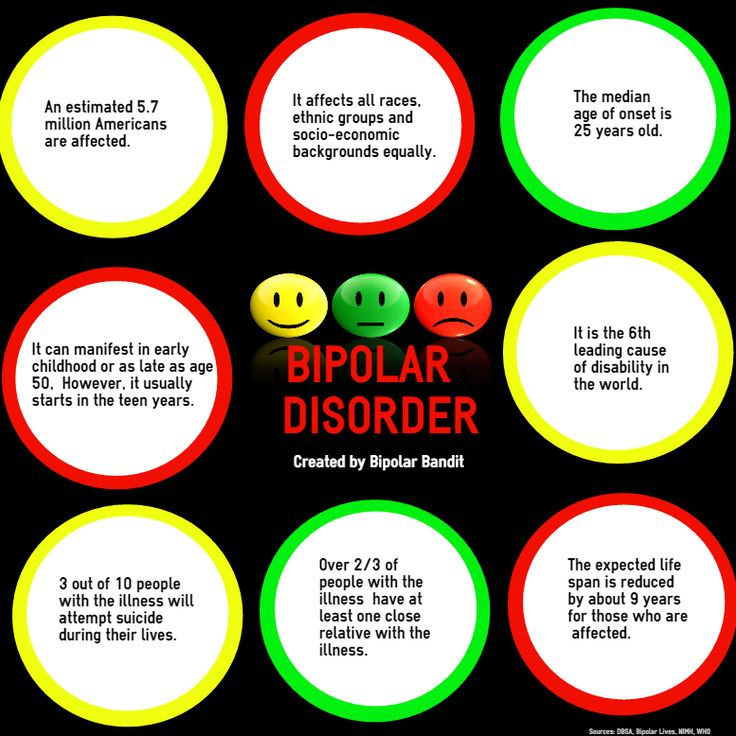
If you suspect that you have bipolar personality disorder, there is no need to panic, only a doctor can diagnose the disease, so you need to make an appointment with a psychotherapist with extensive experience in managing such patients at our MedAstrum clinic. If the diagnosis is confirmed, the doctor will make the necessary medication, if necessary, prescribe psychotherapeutic sessions and give recommendations for further lifestyle adjustments. You can make an appointment yourself on the website or by contacting our administrators.
You might be interested
Autumn depressionBipolar disorder | Symptoms, complications, diagnosis and treatment
Bipolar disorder, formerly called manic depression, is a mental health condition that causes extreme mood swings that include emotional highs (mania or hypomania) and lows (depression). Episodes of mood swings may occur infrequently or several times a year.
When you become depressed, you may feel sad or hopeless and lose interest or pleasure in most activities. When the mood shifts to mania or hypomania (less extreme than mania), you may feel euphoric, full of energy or unusually irritable. These mood swings can affect sleep, energy, alertness, judgment, behavior, and the ability to think clearly.
When the mood shifts to mania or hypomania (less extreme than mania), you may feel euphoric, full of energy or unusually irritable. These mood swings can affect sleep, energy, alertness, judgment, behavior, and the ability to think clearly.
Although bipolar disorder is a lifelong condition, you can manage your mood swings and other symptoms by following a treatment plan. In most cases, bipolar disorder is treated with medication and psychological counseling (psychotherapy).
Symptoms
There are several types of bipolar and related disorders. These may include mania, hypomania, and depression. Symptoms can lead to unpredictable changes in mood and behavior, leading to significant stress and difficulty in life.
- Bipolar disorder I. You have had at least one manic episode, which may be preceded or accompanied by hypomanic or major depressive episodes. In some cases, mania can cause a break with reality (psychosis).
- Bipolar disorder II. You have had at least one major depressive episode and at least one hypomanic episode, but never had a manic episode.
- Cyclothymic disorder. You have had at least two years - or one year in children and adolescents - many periods of hypomanic symptoms and periods of depressive symptoms (though less severe than major depression).
- Other types. These include, for example, bipolar and related disorders caused by certain drugs or alcohol or due to health conditions such as Cushing's disease, multiple sclerosis or stroke.
Bipolar II is not a milder form of Bipolar I but is a separate diagnosis. Although bipolar I manic episodes can be severe and dangerous, people with bipolar II can be depressed for longer periods of time, which can cause significant impairment.
Although bipolar disorder can occur at any age, it is usually diagnosed in adolescence or early twenties. Symptoms can vary from person to person, and symptoms can change over time.
Symptoms can vary from person to person, and symptoms can change over time.
Mania and hypomania
Mania and hypomania are two different types of episodes, but they share the same symptoms. Mania is more pronounced than hypomania and causes more noticeable problems at work, school, and social activities, as well as relationship difficulties. Mania can also cause a break with reality (psychosis) and require hospitalization.
Both a manic and a hypomanic episode include three or more of these symptoms:
- Abnormally optimistic or nervous
- Increased activity, energy or excitement
- Exaggerated sense of well-being and self-confidence (euphoria)
- Reduced need for sleep
- Unusual talkativeness
- Distractibility
- Poor decision-making - for example, in speculation, in sexual encounters, or in irrational investments
Major depressive episode
A major depressive episode includes symptoms that are severe enough to cause noticeable difficulty in daily activities such as work, school, social activities, or relationships. Episode includes five or more of these symptoms:
Episode includes five or more of these symptoms:
- Depressed mood, such as feeling sad, empty, hopeless, or tearful (in children and adolescents, depressed mood may present as irritability)
- Marked loss of interest or feeling of displeasure in all (or nearly all) activities
- Significant weight loss with no diet, weight gain, or decreased or increased appetite (in children, failure to gain weight as expected may be a sign of depression)
- Either insomnia or sleeping too much
- Either anxiety or slow behavior
- Fatigue or loss of energy
- Feelings of worthlessness or excessive or inappropriate guilt
- Decreased ability to think or concentrate, or indecisiveness
- Thinking, planning or attempting suicide
Other features of bipolar disorder
Signs and symptoms of bipolar I and bipolar II disorder may include other signs such as anxiety disorder, melancholia, psychosis, or others.