Behavioral concerns icd 10
Unspecified behavioral and emotional disorders with onset usually occurring in childhood and adolescence
- ICD-10-CM Codes ›
- F01-F99 ›
- F90-F98 ›
- F98- ›
- 2023 ICD-10-CM Diagnosis Code F98.9
Unspecified behavioral and emotional disorders with onset usually occurring in childhood and adolescence
- 2016 2017 2018 2019 2020 2021 2022 2023 Billable/Specific Code
- F98.9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
- Short description: Unsp behav/emotn disord w onst usly occur in chldhd and adol
- The 2023 edition of ICD-10-CM F98.9 became effective on October 1, 2022.
- This is the American ICD-10-CM version of F98.
9 - other international versions of ICD-10 F98.9 may differ.
The following code(s) above F98.9 contain annotation back-references
Annotation Back-References
In this context, annotation back-references refer to codes that contain:
- Applicable To annotations, or
- Code Also annotations, or
- Code First annotations, or
- Excludes1 annotations, or
- Excludes2 annotations, or
- Includes annotations, or
- Note annotations, or
- Use Additional annotations
that may be applicable to F98.9:
- F01-F99
2023 ICD-10-CM Range F01-F99
Mental, Behavioral and Neurodevelopmental disorders
Includes
- disorders of psychological development
Type 2 Excludes
- symptoms, signs and abnormal clinical laboratory findings, not elsewhere classified (R00-R99)
- F90-F98
2023 ICD-10-CM Range F90-F98
Behavioral and emotional disorders with onset usually occurring in childhood and adolescence
Note
- Codes within categories F90-F98 may be used regardless of the age of a patient.
 These disorders generally have onset within the childhood or adolescent years, but may continue throughout life or not be diagnosed until adulthood
These disorders generally have onset within the childhood or adolescent years, but may continue throughout life or not be diagnosed until adulthood
- Codes within categories F90-F98 may be used regardless of the age of a patient.
- F98
ICD-10-CM Diagnosis Code F98
Other behavioral and emotional disorders with onset usually occurring in childhood and adolescence
- 2016 2017 2018 2019 2020 2021 2022 2023 Non-Billable/Non-Specific Code
Type 2 Excludes
- breath-holding spells (R06.89)
- gender identity disorder of childhood (F64.2)
- Kleine-Levin syndrome (G47.13)
- obsessive-compulsive disorder (F42.-)
- sleep disorders not due to a substance or known physiological condition (F51.-)
Approximate Synonyms
- Behavior disorder, disruptive
- Behavioral and emotional disorder with onset in childhood
- Communication disorder, nonorganic
- Disruptive behavior disorder
- Disruptive behaviour disorder
- Emotional disturbance childhood or adolescence
- Mental disorder of infancy, childhood or adolescence
- Non-organic communication disorder
ICD-10-CM F98. 9 is grouped within Diagnostic Related Group(s) (MS-DRG v40.0):
9 is grouped within Diagnostic Related Group(s) (MS-DRG v40.0):
- 886 Behavioral and developmental disorders
Convert F98.9 to ICD-9-CM
Code History
- 2016 (effective 10/1/2015): New code (first year of non-draft ICD-10-CM)
- 2017 (effective 10/1/2016): No change
- 2018 (effective 10/1/2017): No change
- 2019 (effective 10/1/2018): No change
- 2020 (effective 10/1/2019): No change
- 2021 (effective 10/1/2020): No change
- 2022 (effective 10/1/2021): No change
- 2023 (effective 10/1/2022): No change
Diagnosis Index entries containing back-references to F98. 9:
9:
ICD-10-CM Codes Adjacent To F98.9
F98 Other behavioral and emotional disorders with onset usually occurring in childhood and adolescence
F98.0 Enuresis not due to a substance or known physiological condition
F98.1 Encopresis not due to a substance or known physiological condition
F98.2 Other feeding disorders of infancy and childhood
F98. 21 Rumination disorder of infancy
21 Rumination disorder of infancy
F98.29 Other feeding disorders of infancy and early childhood
F98.3 Pica of infancy and childhood
F98.4 Stereotyped movement disorders
F98.5 Adult onset fluency disorder
F98.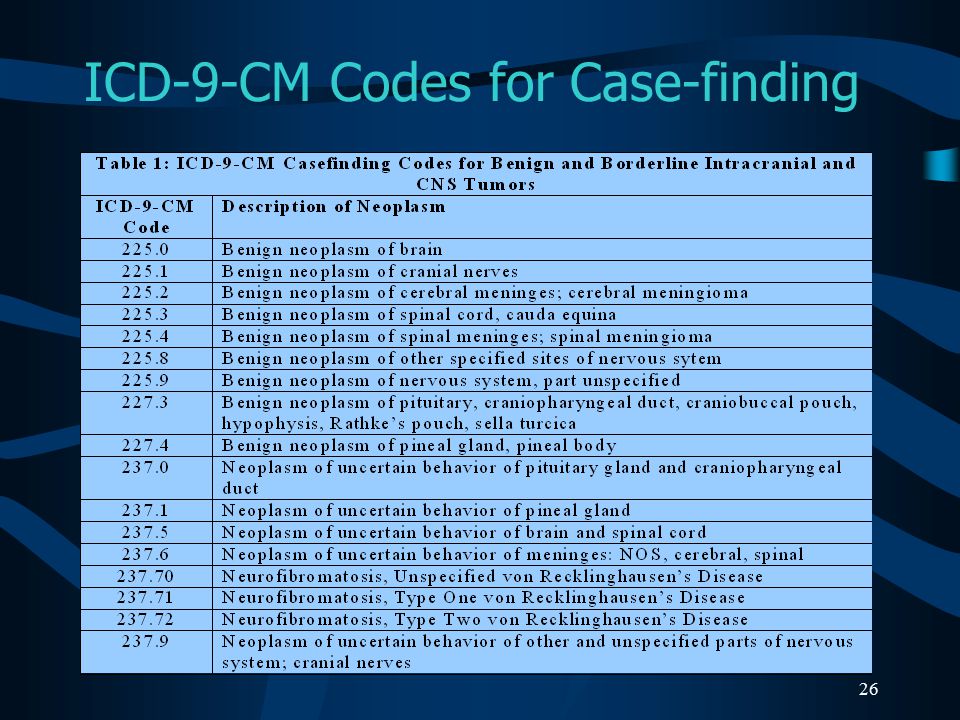 8 Other specified behavioral and emotional disorders with onset usually occurring in childhood and adolescence
8 Other specified behavioral and emotional disorders with onset usually occurring in childhood and adolescence
F98.9 Unspecified behavioral and emotional disorders with onset usually occurring in childhood and adolescence
F99 Mental disorder, not otherwise specified
G00 Bacterial meningitis, not elsewhere classified
G00. 0 Hemophilus meningitis
0 Hemophilus meningitis
G00.1 Pneumococcal meningitis
G00.2 Streptococcal meningitis
G00.3 Staphylococcal meningitis
G00.8 Other bacterial meningitis
G00.9 Bacterial meningitis, unspecified
G01 Meningitis in bacterial diseases classified elsewhere
G02 Meningitis in other infectious and parasitic diseases classified elsewhere
Reimbursement claims with a date of service on or after October 1, 2015 require the use of ICD-10-CM codes.
2023 ICD-10-CM Diagnosis Code F91.9: Conduct disorder, unspecified
- ICD-10-CM Codes ›
- F01-F99 ›
- F90-F98 ›
- F91- ›
- 2023 ICD-10-CM Diagnosis Code F91.9
Conduct disorder, unspecified
- 2016 2017 2018 2019 2020 2021 2022 2023 Billable/Specific Code
- F91.9 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
- The 2023 edition of ICD-10-CM F91.9 became effective on October 1, 2022.
- This is the American ICD-10-CM version of F91.9 - other international versions of ICD-10 F91.9 may differ.
Applicable To
- Behavioral disorder NOS
- Conduct disorder NOS
- Disruptive behavior disorder NOS
- Disruptive disorder NOS
The following code(s) above F91. 9 contain annotation back-references
9 contain annotation back-references
Annotation Back-References
In this context, annotation back-references refer to codes that contain:
- Applicable To annotations, or
- Code Also annotations, or
- Code First annotations, or
- Excludes1 annotations, or
- Excludes2 annotations, or
- Includes annotations, or
- Note annotations, or
- Use Additional annotations
that may be applicable to F91.9:
- F01-F99
2023 ICD-10-CM Range F01-F99
Mental, Behavioral and Neurodevelopmental disorders
Includes
- disorders of psychological development
Type 2 Excludes
- symptoms, signs and abnormal clinical laboratory findings, not elsewhere classified (R00-R99)
- F90-F98
2023 ICD-10-CM Range F90-F98
Behavioral and emotional disorders with onset usually occurring in childhood and adolescence
Note
- Codes within categories F90-F98 may be used regardless of the age of a patient.
 These disorders generally have onset within the childhood or adolescent years, but may continue throughout life or not be diagnosed until adulthood
These disorders generally have onset within the childhood or adolescent years, but may continue throughout life or not be diagnosed until adulthood
- Codes within categories F90-F98 may be used regardless of the age of a patient.
- F91
ICD-10-CM Diagnosis Code F91
Conduct disorders
- 2016 2017 2018 2019 2020 2021 2022 2023 Non-Billable/Non-Specific Code
Type 1 Excludes
- antisocial behavior (Z72.81-)
- antisocial personality disorder (F60.2)
Type 2 Excludes
- conduct problems associated with attention-deficit hyperactivity disorder (F90.-)
- mood [affective] disorders (F30-F39)
- pervasive developmental disorders (F84.-)
- schizophrenia (F20.-)
Approximate Synonyms
- Abnormal behavior
- Abnormal behaviour
- Behavior disorder
- Conduct disorder
- Stroke, late effects, behavioral/cognitive disorder
Clinical Information
- A classification of disorders in the diagnostic and statistical manual of mental disorders (dsm) that are usually diagnosed in infancy, childhood or adolescence and are characterized by an individual's inability to behave in a cooperative manner.
- A disorder diagnosed in childhood or adolescence age group characterized by aggressive behavior, deceitfulness, destruction of property or violation of rules that is persistent and repetitive, and within a one year period.
- A repetitive and persistent pattern of behavior in which the basic rights of others or major age-appropriate societal norms or rules are violated. These behaviors include aggressive conduct that causes or threatens physical harm to other people or animals, nonaggressive conduct that causes property loss or damage, deceitfulness or theft, and serious violations of rules. The onset is before age 18. (from dsm-iv, 1994)
- Any of various conditions characterized by impairment of an individual's normal behavioral functioning, and caused by social, psychological, biochemical, genetic, or other factors, such as infection or head trauma.
- Disorders characterized by persistent and repetitive patterns of behavior that violate societal norms or rules or that seriously impair a person's functioning.
 Compare behavior problems.
Compare behavior problems. - Mental disorder of childhood and adolescence characterized by repetitive and persistent patterns of conduct in which rights of others and age-appropriate societal rules are violated; the conduct is more serious than ordinary mischief and pranks.
- Repetitive and persistent aggressive or nonaggressive behavior in which basic rights of others or social norms are violated. Self esteem is generally low, and an inability to develop social relationships and lack of concern for others may or may not be present.
ICD-10-CM F91.9 is grouped within Diagnostic Related Group(s) (MS-DRG v40.0):
- 886 Behavioral and developmental disorders
Convert F91.9 to ICD-9-CM
Code History
- 2016 (effective 10/1/2015): New code (first year of non-draft ICD-10-CM)
- 2017 (effective 10/1/2016): No change
- 2018 (effective 10/1/2017): No change
- 2019 (effective 10/1/2018): No change
- 2020 (effective 10/1/2019): No change
- 2021 (effective 10/1/2020): No change
- 2022 (effective 10/1/2021): No change
- 2023 (effective 10/1/2022): No change
Diagnosis Index entries containing back-references to F91. 9:
9:
- Disorder (of) - see also Disease
- conduct (childhood) F91.9
- disruptive F91.9
- Disturbance(s) - see also Disease
- conduct F91.9 - see also Disorder, conduct
- disruptive F91.9
- conduct F91.9 - see also Disorder, conduct
ICD-10-CM Codes Adjacent To F91.9
F90.1 Attention-deficit hyperactivity disorder, predominantly hyperactive type
F90.2 Attention-deficit hyperactivity disorder, combined type
F90.8 Attention-deficit hyperactivity disorder, other type
F90. 9 Attention-deficit hyperactivity disorder, unspecified type
9 Attention-deficit hyperactivity disorder, unspecified type
F91 Conduct disorders
F91.0 Conduct disorder confined to family context
F91.1 Conduct disorder, childhood-onset type
F91.2 Conduct disorder, adolescent-onset type
F91.3 Oppositional defiant disorder
F91. 8 Other conduct disorders
8 Other conduct disorders
F91.9 Conduct disorder, unspecified
F93 Emotional disorders with onset specific to childhood
F93.0 Separation anxiety disorder of childhood
F93.8 Other childhood emotional disorders
F93. 9 Childhood emotional disorder, unspecified
9 Childhood emotional disorder, unspecified
F94 Disorders of social functioning with onset specific to childhood and adolescence
F94.0 Selective mutism
F94.1 Reactive attachment disorder of childhood
F94.2 Disinhibited attachment disorder of childhood
F94. 8 Other childhood disorders of social functioning
8 Other childhood disorders of social functioning
F94.9 Childhood disorder of social functioning, unspecified
Reimbursement claims with a date of service on or after October 1, 2015 require the use of ICD-10-CM codes.
10 | Classification of mental disorders
ICD-10 Preface
ICD-10 Preface.
In the early 1960s, the World Health Organization began an active program to improve the diagnosis and classification of mental disorders. At that time, WHO held a series of meetings at which representatives of various disciplines and psychiatric schools from around the world summarized the then existing knowledge in this area. WHO has stimulated and conducted a study on classification criteria and diagnostic reproducibility. In addition, procedures for collaborative diagnostic assessments of clinical material based on the study of video interviews with patients and other methods were developed and disseminated.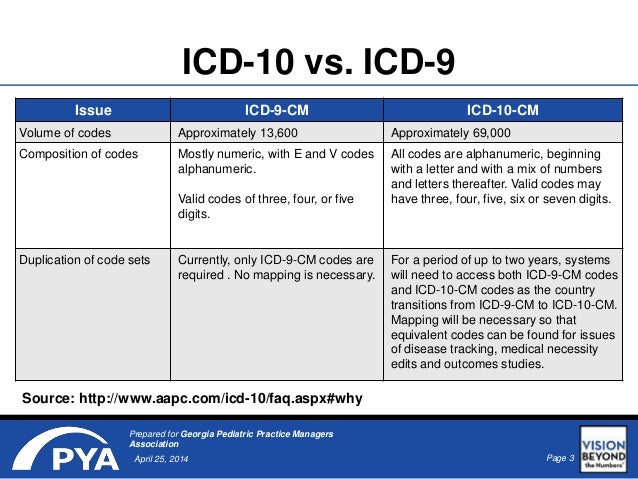 As a result of numerous proposals for improving the classification of mental disorders, the 8th revision of the International Classification of Disease (ICD-8) was carried out during the widest consultations. A special glossary was developed with the definition of each category of mental disorders in the ICD-8. The work on the above program also led to the creation of a team of individuals and a network of national centers dealing with the problems of improving psychiatric classification. nine0003
As a result of numerous proposals for improving the classification of mental disorders, the 8th revision of the International Classification of Disease (ICD-8) was carried out during the widest consultations. A special glossary was developed with the definition of each category of mental disorders in the ICD-8. The work on the above program also led to the creation of a team of individuals and a network of national centers dealing with the problems of improving psychiatric classification. nine0003
In the 1970s there was an increasing interest in improving the psychiatric systematics around the world. This was facilitated by the expansion of international contacts, the organization of several international collaborative studies and the emergence of the possibility of new forms of therapy. In a number of countries, the development of specific classification criteria has been encouraged to improve diagnostic reproducibility. In particular, the American Psychiatric Association developed and disseminated the 3rd revision of the Diagnostic and Statistical Manual, which included the use of operational criteria in its classification system.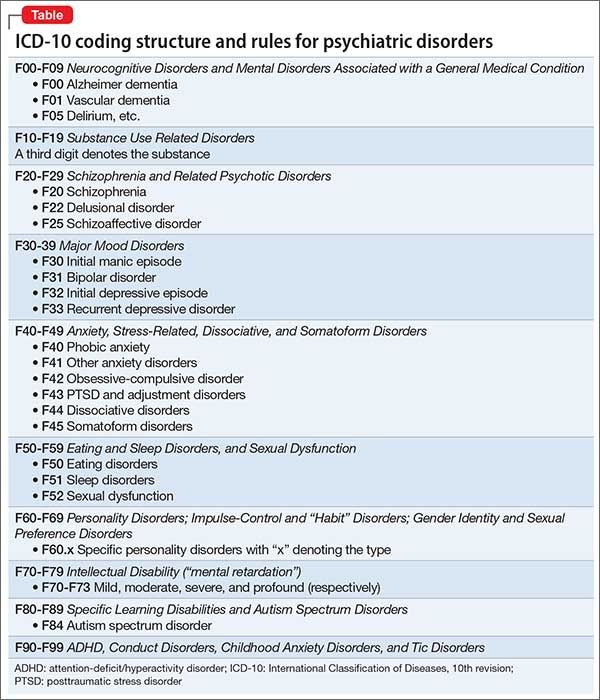 nine0003
nine0003
In 1978, WHO entered into a long-term project with the United States Administration of Mental Health and Alcohol and Drug Abuse to further improve the classification and diagnosis of mental disorders and problems related to alcohol and drug use. A series of workshops that brought together scholars from different psychiatric traditions reviewed the knowledge in the respective fields and developed recommendations for further research. These recommendations were summarized at a major international conference in Copenhagen (Denmark) at 1982 year.
Several major studies have been undertaken to implement the recommendations of the Copenhagen Conference. One of them, which involved centers from 17 countries, aimed at developing the Consolidated International Diagnostic Interview, a tool that would be suitable for conducting epidemiological studies of mental disorders in general populations of various countries. Another major project focused on the development of an assessment tool suitable for use by clinicians. Another study was devoted to the development of a tool for assessing personality disorders in various countries. nine0003
Another study was devoted to the development of a tool for assessing personality disorders in various countries. nine0003
In addition, several more dictionaries with clear definitions of terms have been prepared and are being prepared. The work on these projects has been fruitfully associated with the development of definitions for mental and behavioral disorders in the International Statistical Classification of Diseases and Related Health Problems (ICD-10). The translation of diagnostic criteria into diagnostic algorithms included in the assessment tools has been useful in identifying inconsistencies, points of contention and repetitions that can be eliminated. On the other hand, the work on the ICD-10 helped shape the assessment tools. The final result has been the creation of a clear system of criteria for ICD-10 and scoring tools that can provide the data needed to classify disorders according to the criteria included in Chapter V (F) of ICD-10. nine0003
The Copenhagen Conference also recommended that the positions of the various psychiatric schools be presented in publications on the sources of the ICD-10 classification. As a result, several major publications have appeared.
As a result, several major publications have appeared.
The first book of publications compiled on the basis of chapter V (F) of ICD-10 was the glossary "Clinical descriptions and diagnostic guidelines". It represents the completion of the efforts of many people who have worked on it over the years. In the course of this work, several large projects were prepared, each of which came out after numerous consultations with expert groups, national and international psychiatric associations and individual consultants. Project 1987 served as the basis for trials in 40 national centers, which was an unprecedented study of its kind aimed at improving psychiatric diagnosis. The results of these trials were used to prepare the final version of the clinical guidelines.
The text presented in this book has also been extensively tested. It involved researchers and clinicians from 32 countries. Future publications will include a version for general practitioners, a multi-axis variant of the classification, a series of publications detailing more specific issues (for example, on the assessment and classification of mental retardation), as well as reference materials that allow comparison of relevant terms in ICD-10, ICD- nineand ICD-8.
With the accumulation of experience and the expansion of our knowledge, it should be possible to further improve the classification of mental disorders. This task will be entrusted mainly to those WHO centers that have been involved in the preparation of this classification.
There are numerous publications from national centers on and in connection with ICD-10 research. A complete list and reprints of the articles are available on request from the Department of Mental Health, WHO, 1211 Geneva 27, Switzerland. nine0003
Classification is a way of seeing the world at a certain time stage. Without a doubt, scientific progress and experience in the application of these research criteria will require their revision and updating. I hope that such a revision will be the result of the same cordial and productive international scientific cooperation as in the preparation of this classification.
Norman Sartorius
Director of Mental Health WHO
ICD-10 Notes
ICD-10 Notes.
1. The content of the Investigative Diagnostic Criteria (IDC-10) is derived from chapter V (P) of the ICD-10. It provides specific criteria for diagnoses from the Clinical Descriptions and Diagnostic Guidelines (COD) glossary, which has been prepared for clinicians, educators of psychiatry, and other mental health professionals.
2. IDK-10, although they are fully compatible with CODE and ICD-10, differ in style of presentation. They are not intended to be used in isolation, so researchers should familiarize themselves with CODEs. The IIR-10 does not contain descriptions of the clinical concepts on which the research criteria are based, or any commentary on commonly associated symptoms that, while not necessary for diagnosis, may be of value to both clinicians and investigators. Information and comments about these symptoms can be found in the introductory chapters of CODE. It is expected that every psychiatrist using the IDK-10 will also have a copy of the CODE. nine0003
nine0003
3. For adequate use of IDK-10, some other differences from KODU should be noted.
-
a) Like other published research diagnostic criteria, the IDK-10 criteria are intentionally narrow: their use allows selection of groups of patients whose symptoms and other characteristics are similar in a number of certain respects. This contributes to the homogenization of groups of patients, but limits the possible generalizations. Researchers wishing to study partial similarities between diagnostic units, or to define boundaries between them, may therefore need additional criteria to allow inclusion of atypical cases in the study. nine0003
-
b) Due to inadequacy, detailed criteria are not provided for the rubrics for unspecified disorders (.9) and, as a rule, for the rubrics for "other" disorders (.8). Annex 1 provides proposals with criteria for some headings for which there are conflicting data and which require further study.
-
c) Depending on the objectives of the study, different research projects have different requirements for exclusion criteria and the possibility of comorbidity.
 Therefore, IIR-10 provides only some of the most obvious and commonly used exclusion criteria for reminder and ease of use, and more details can be found in the CODE if necessary. nine0003
Therefore, IIR-10 provides only some of the most obvious and commonly used exclusion criteria for reminder and ease of use, and more details can be found in the CODE if necessary. nine0003
4. The impact of the disorder on social role performance was not generally used as a diagnostic criterion in ICD-10, but there are some unavoidable exceptions, the most obvious of which are dementia, simple schizophrenia and antisocial personality disorder. Once the decision was made to include these disorders in the classification, it was decided to do so without modification of the relevant concepts, and as a result it became necessary to include social role obstruction as a diagnostic criterion for these disorders. Subsequent research and experience will show the justification for such a decision. nine0003
Among the diagnostic criteria for many disorders of childhood and adolescence, some forms of the influence of disorders on social relationships and behavior have found their place. This may at first appear to be contrary to the above general rules of the ICD. However, a closer look at the disorders classified in F80-89 and F90-F98 reveals that the need for a social criterion here is due to the more complex nature of the disorders. Children often show distress and frustration, but there are rarely specific complaints and symptoms equivalent to those that characterize disorders in adults. Many disorders in F80-F89and F90-F98 are comorbidities that can only be described by an indication of how they affect roles in the family, school, and peer group.
5. For the same reason as in 3(c) above, definitions of remission, relapse, and episode duration are only rarely given. Corresponding proposals are being prepared in the glossary of terms for chapter V (P) of the ICD-10 "Classification of mental and behavioral disorders"
6. Criteria are marked with letters and/or numbers to indicate their degree of importance. General criteria that must be met in all rubrics of the relevant group of disorders (for example, general criteria for all types of dementia or major forms of schizophrenia) are marked with a capital G followed by the corresponding number. Mandatory criteria for individual disorders are marked only in capital letters (A, B, C, etc.). Numbers (1, 2, 3, etc.) and lowercase letters (a, b, etc.) indicate groups and subgroups of characteristics, of which only a few are required for diagnosis. In order not to use "and (or)" when one of the two criteria is required, it is always understood that the presence of both criteria also satisfies the diagnosis. nine0003
Mandatory criteria for individual disorders are marked only in capital letters (A, B, C, etc.). Numbers (1, 2, 3, etc.) and lowercase letters (a, b, etc.) indicate groups and subgroups of characteristics, of which only a few are required for diagnosis. In order not to use "and (or)" when one of the two criteria is required, it is always understood that the presence of both criteria also satisfies the diagnosis. nine0003
7. When using ICD-10 on patients suffering from neurological disorders, investigators may also use the neurological chapter of ICD-10 with an appropriate glossary.
8. The two annexes to the DCO-10 deal with disorders of uncertain status, which are provisional in nature. Appendix 1 deals with some affective disorders that have been the subject of recent research and some personality disorders. Although their respective concepts are considered clinically relevant in some countries, from an international perspective, these disorders themselves are of uncertain standing; it is hoped that their inclusion here will facilitate the study of their suitability. nine0003
nine0003
Appendix 2 provides pre-written descriptions of a number of disorders often referred to as "culturally specific". There are reasons to believe that they are better considered as cultural variants of the disorders already included in Chapter V (P) of the ICD-10, but there is still a lack of reliable and detailed clinical information for definite conclusions about them. Classification trials in some national centers have encountered significant practical difficulties in assessing cases of these disorders, but including their descriptions in the IIR-10 may facilitate research by psychiatrists who are familiar with the language and culture of the cases. The information in the appendix will be complemented by a terminological dictionary on cross-cultural psychiatry, which is expected to be published in 1994 year.
9. Please note that in the category names, instead of "and (or)" there is only one word "and".
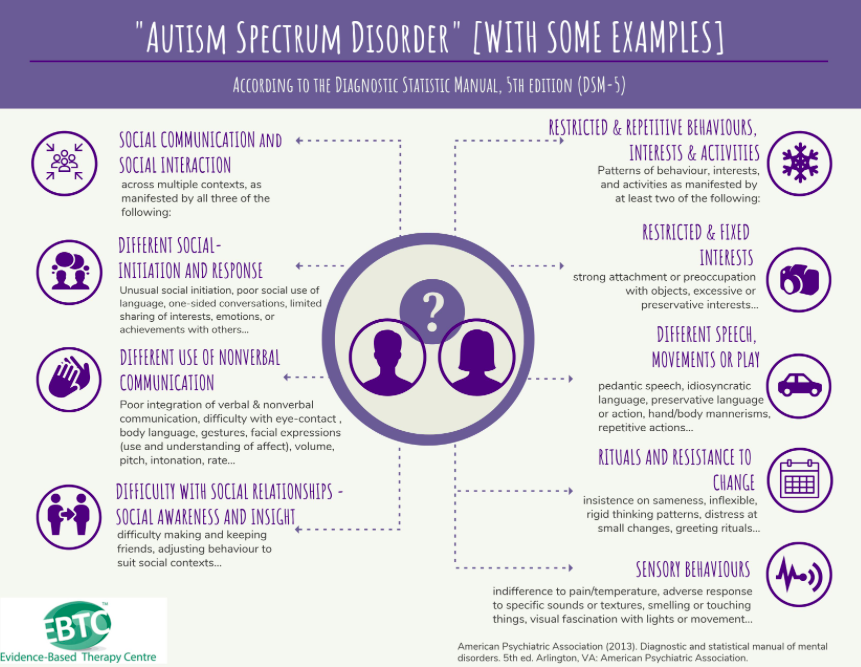
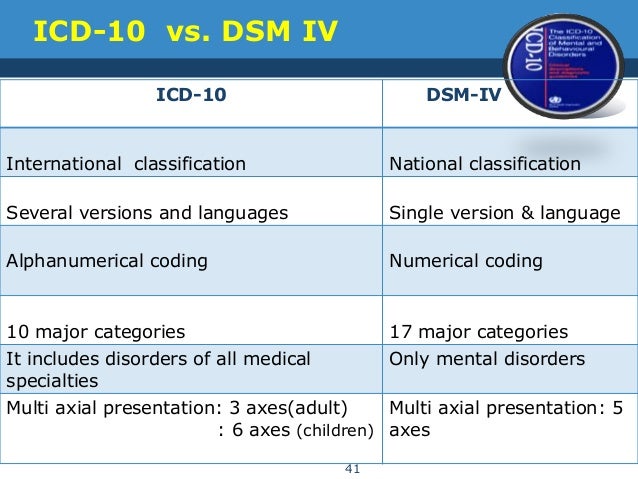
ICD-10 and DSM-V: differences in the diagnosis of ED
“Today there are 2 main guidelines that specialists from different countries rely on to classify and diagnose all existing diseases, including eating disorders.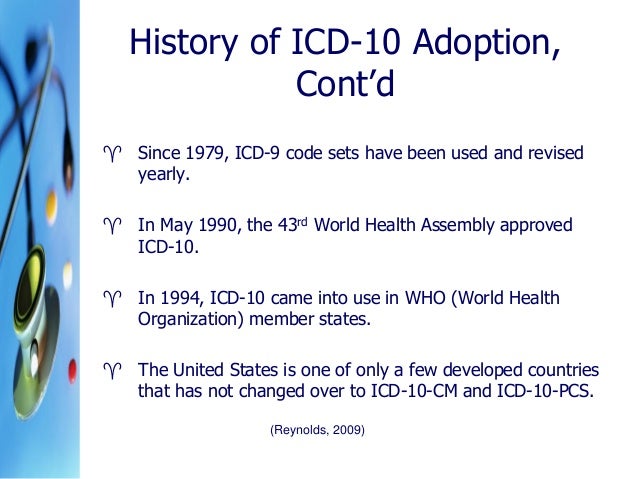 These are the ICD (International Statistical Classification of Diseases and Related Health Problems) and the DSM (Diagnostic and Statistical Manual of Mental Disorders). nine0003
These are the ICD (International Statistical Classification of Diseases and Related Health Problems) and the DSM (Diagnostic and Statistical Manual of Mental Disorders). nine0003
Of course, there are also national guidelines and classifications. For example, in Soviet psychiatry, such a type of schizophrenia as sluggish schizophrenia was separately distinguished, although such a diagnosis is generally absent in international classifications.
Nevertheless, qualified specialists are guided by the ICD or DSM in their work.
The ICD has more than three hundred years of history and is currently the official normative document of the World Health Organization. nine0003
ICD went through 10 editions. The current ICD-10 is used, which has been in use in WHO Member States since 1994. And work is already underway on the ICD-11, which is planned to be introduced after 2018.
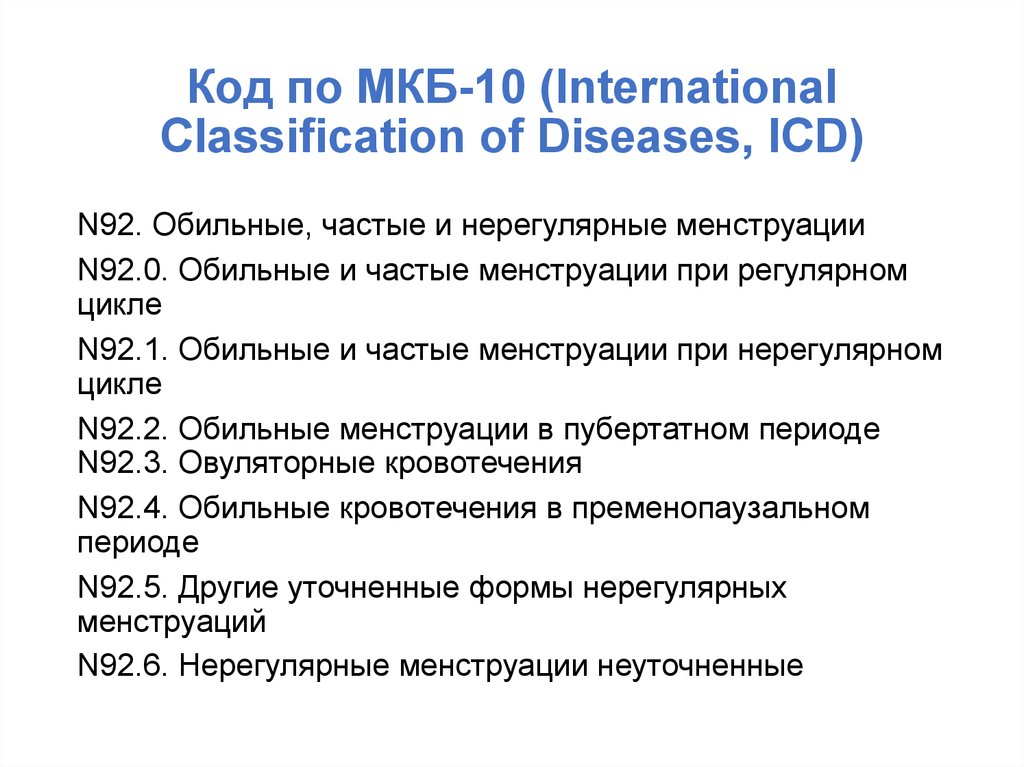
It is important to note that ICD-10 covers all diseases. Mental and behavioral disorders are presented there only in a separate chapter.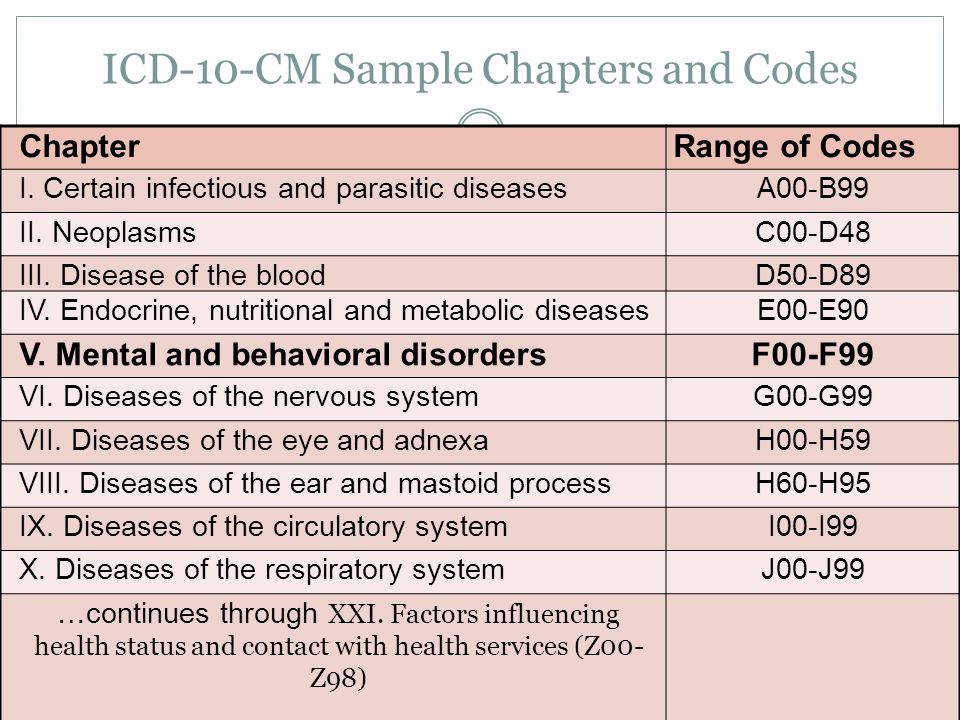 And eating disorders are not singled out in a separate rubric in this chapter, but are included in a broader rubric - Behavioral Syndromes Associated with Physiological Disorders and Physical Factors. nine0003
And eating disorders are not singled out in a separate rubric in this chapter, but are included in a broader rubric - Behavioral Syndromes Associated with Physiological Disorders and Physical Factors. nine0003
This heading has a subheading "Eating Disorders" (code F50), which includes:
- anorexia nervosa
- bulimia nervosa
- overeating associated with other psychological disorders
- vomiting associated with other psychological disorders
- other eating disorders
- Eating disorder, unspecified
The fundamental point is that in ICD-10 there is only a classification and key features of eating disorders. And that's it! Data on detailed description of criteria, prevalence, differential diagnosis, etc. in the ICD, unfortunately, you will not find. nine0003
Regarding the DSM, this guide was originally developed by the American Psychiatric Association. The first edition (DSM-I) was in 1952. Now the 5th edition (DSM-V), released in 2013, is already in use.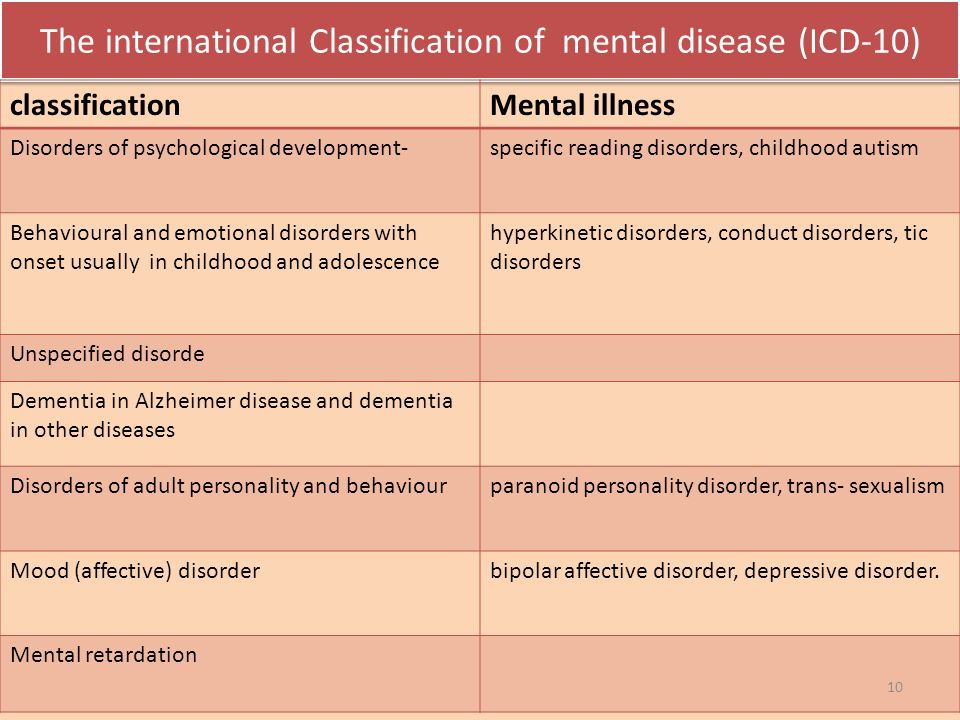 This edition is not available in Russian.
This edition is not available in Russian.
A distinctive feature of this manual is the detailed classification and, most importantly, the description of mental disorders (hence the name).
In particular, there is a separate section devoted to eating disorders. nine0003
The following eating disorders are distinguished in it:
- "peak" (perverted appetite)
- chewing disorder
- avoidant/restrictive eating disorder
- anorexia nervosa
- bulimia nervosa
- overeating
- other specific eating or eating disorders
- non-specific eating or eating disorders nine0081
- criteria for diagnosing eating disorders
- extended explanation for each criterion
- subtypes or severity of disorder
- diagnostic features
- data on the prevalence of the disorder
- information on the course and development of the disease
- risk factors
- specific diagnostic markers
- suicide risk data
- consequences of eating disorders
- differential diagnosis
- association with other psychiatric disorders (not related to eating disorders).
An important difference of the DSM-V is that, unlike the ICD-10, for each of the major eating disorders are given:
In addition, DSM-V is the most current version released in 2013. It presents the latest data on the criteria for mental disorders, some of which differ from those in earlier versions of the guide. nine0003
This also applies to eating disorders.”
The author of the article is Sergei Leonov, source https://www.b17.ru/article/mkb10-i-dsm5-otlichiya-v-diagnostike/
* — required fields
By submitting an application, you agree to the terms
of the privacy policy
Read also
Interview of the head physician to the portal anorexia.pro
Maksim Sologub, head physician of the Moscow Center for the Study of Eating Disorders, tells…
Read more »
Anorexia. The plot of the program "Live healthy" on Channel One
We are on the first!
Read more »
Release of the Good Morning program on Channel One
Watch the episode of the Good Morning program on Channel One dedicated to the Day of Struggle against …
Read more »
Live Healthy program on Channel One
On October 13, the program “Live Healthy” was released, where the psychiatrist of the Center took part .