Aversive conditioning in psychology
What It Is, Efficacy, Controversy, and More
Aversion therapy, sometimes called aversive therapy or aversive conditioning, is used to help a person give up a behavior or habit by having them associate it with something unpleasant.
Aversion therapy is most known for treating people with addictive behaviors, like those found in alcohol use disorder. Most research has been focused on its benefits relating to substance use.
This type of therapy is controversial and research is mixed. Aversion therapy isn’t often a first-line treatment and other therapies are preferred.
How long the therapy lasts for has also been criticized, as outside of the therapy, relapse may occur.
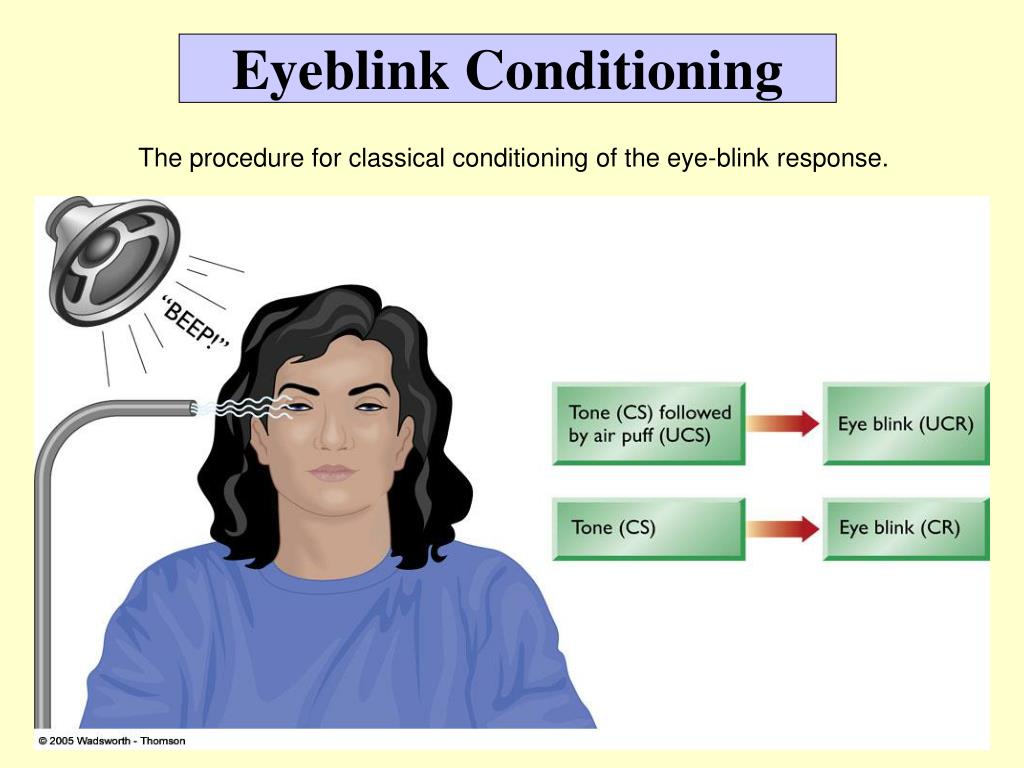
Aversion therapy is based off the theory of classical conditioning. Classical conditioning is when you unconsciously or automatically learn a behavior due to a specific stimuli. In other words, you learn to respond to something based on repeated interactions with it.
Aversion therapy uses conditioning but focuses on creating a negative response to an undesirable stimulus, such as drinking alcohol or using drugs.
Many times, in people with substance use disorders, the body is conditioned to get pleasure from the substance — for instance, it tastes good and makes you feel good. In aversion therapy, the idea is to change that.
The exact way aversion therapy is performed depends on the undesirable behavior or habit that’s being treated. One commonly used aversive therapy is chemical aversion for alcohol use disorder. The goal is to reduce a person’s craving for alcohol with chemically-induced nausea.
In chemical aversion, a doctor administers a drug that causes nausea or vomiting if the person being treated drinks alcohol. They then give them alcohol so that the person gets sick. This is repeated until the person begins to associate drinking alcohol with feeling ill and thus no longer craves alcohol.
Other methods that have been used for aversion therapy include:
- electrical shock
- another type of physical shock, like from a rubber band snapping
- an unpleasant smell or taste
- negative imagery (sometimes through visualization)
- shame
Can you do aversion therapy at home?Traditional aversion therapy is done under the supervision of a psychologist or other therapist.
You can, however, use aversion conditioning at-home for simple bad habits, such as biting your nails.
To do this, you can place a clear coat of nail polish on your nails, which will taste bad when you go to bite them.
Aversion therapy is believed to be helpful for people wanting to quit a behavior or habit, typically one that’s interfering with their life negatively.
While a lot of research has been done on aversion therapy and alcohol use disorder, other uses for this type of therapy have included:
- other substance use disorders
- smoking
- eating disorders
- oral habits, such as nail biting
- self-injurious and aggressive behaviors
- certain inappropriate sexual behaviors, such as voyeuristic disorder
Research on these applications is mixed. Some, like lifestyle behaviors, have been generally shown as ineffective. More promise has been found for addiction when using chemical aversion.
Some research has shown that aversion therapy is effective for treating alcohol use disorder.
Recent research found that participants who craved alcohol prior to the therapy reported avoiding alcohol 30 and 90 days after treatment.
Yet, research is still mixed on the effectiveness of aversion therapy. While many studies have shown promising short-term results, the long-term effectiveness is questionable.
While the previously mentioned study found that 69 percent of participants reported sobriety 1 year after treatment, a longer-term study would help to see if it lasted past that first year.
In some of the most comprehensive research on aversion therapy in the 1950s, researchers noted a decline in abstinence over time. After 1 year, 60 percent remained alcohol-free, but it was only 51 percent after 2 years, 38 percent after 5 years, and 23 percent after 10 years or more.
It’s believed that the lack of long-term benefit occurs because most aversion therapy happens in-office. When you’re away from the office, the aversion is harder to maintain.
While aversion therapy may be effective in the short-term for alcohol, there have been mixed results for other uses.
Most research has found aversion therapy to be unhelpful for smoking cessation, especially when the therapy involves rapid smoking. For example, a person would be asked to smoke an entire pack of cigarettes in a very short amount of time until they feel ill.
Aversion therapy has also been considered for treating obesity, but it was extremely hard to generalize to all foods and maintain outside of the therapy.
Aversion therapy has had backlash in the past for several reasons.
Some experts believe that using negative stimulus in aversion therapy is equal to using punishment as a form of therapy, which is unethical.
Before the American Psychiatric Association (APA) deemed it an ethical violation, some researchers used aversion therapy to “treat” homosexuality.
Prior to 1973, homosexuality was considered a mental illness in the Diagnostic and Statistical Manual of Mental Disorders (DSM). Some medical professionals believed that it was possible to “cure” it. A homosexual person could be imprisoned or potentially forced into a program of aversion therapy for revealing their orientation.
A homosexual person could be imprisoned or potentially forced into a program of aversion therapy for revealing their orientation.
Some people did voluntarily seek this or other types of psychiatric therapy for homosexuality. This was often due to shame and guilt, as well as societal stigma and discrimination. However, evidence showed that this “treatment” was both ineffective and harmful.
After the APA removed homosexuality as a disorder due no scientific evidence, most research on aversion therapy for homosexuality stopped. Yet, this harmful and unethical use of aversion therapy left it with a bad reputation.
Aversion therapy may be helpful for stopping specific types of unwanted behaviors or habits. Yet, experts believe that even if used, it shouldn’t be used alone.
Aversion therapy is a type of counterconditioning treatment. A second one is called exposure therapy, which works by exposing a person to something they fear. Sometimes these two types of therapies can be combined for a better outcome.
Therapists may also recommend other types of behavioral therapy, along with in or outpatient rehabilitation programs for substance use disorders. For many people who experience addiction, support networks can also help to keep them on track with recovery.
Medication may be prescribed in some cases, including for smoking cessation, mental health conditions, and obesity.
Aversion therapy aims to help people stop undesirable behaviors or habits. Research is mixed on its uses, and many doctors may not recommend it due to criticism and controversy.
You and your healthcare provider can discuss the right treatment plan for you, whether that includes aversion therapy or not. Often, a combination of treatments including talk therapy and medication can help you cope with your concern.
If you have a substance use disorder or believe you may be experiencing addiction, reach out to a healthcare provider. If you’re not sure where to start, you can call SAMHSA’s National Helpline at 800-662-4357.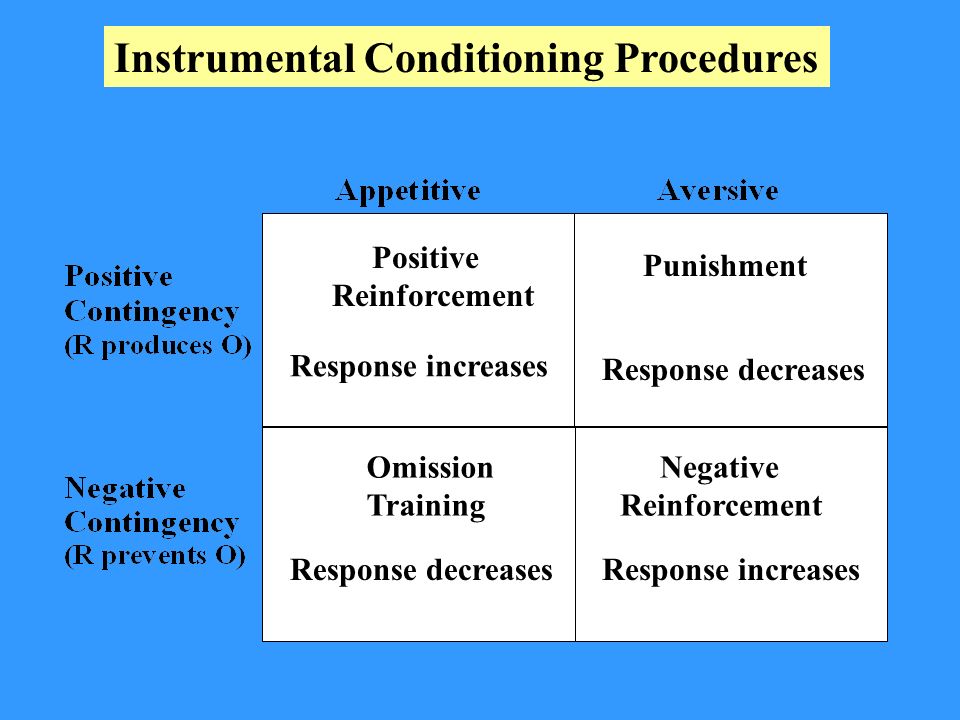
Understanding Aversive Conditioning With Examples
Are you plagued by a bad habit that you just can’t seem to get rid of? Understanding how aversive conditioning works might be of some help to you. In this PsycholoGenie post, we will discuss a couple of examples of this psychology concept, to make it easier for you to get the hang of it.
Trivia
Stanley Kubrick’s film A Clockwork Orange has one the best depictions of aversive conditioning in popular culture.
In his 1971 film, A Clockwork Orange, Kubrick introduced us to a fictional therapy known as the Ludovico technique. It was used to condition the protagonist Alex DeLarge, to experience severe nausea every time he experiences violence or thinks about it, by forcing him to watch violent images under the effect of a nausea-inducing drug. While Kubrick’s Ludovico technique was a fictional therapy, its striking resemblance to aversive conditioning is difficult to miss.
What is Aversive Conditioning?
By definition, aversive conditioning―or aversive therapy to be precise―is a form of conditioning, wherein, the subject is simultaneously exposed to a stimulus (particular behavior) and discomfort, as a result of which he starts associating the two and stops the said behavior. Simply put, the harmful stimulus that acts as a trigger of the bad behavior is paired with a new negative response, which helps suppress the said behavior. The concept revolves around the fact that, if behavior can be learned, it can also be unlearned. You just need to employ the correct technique.
Simply put, the harmful stimulus that acts as a trigger of the bad behavior is paired with a new negative response, which helps suppress the said behavior. The concept revolves around the fact that, if behavior can be learned, it can also be unlearned. You just need to employ the correct technique.
Aversive conditioning can be an effective treatment for a variety of addictions and bad habits, one of the most popular being cussing. A simple but effective method of getting rid of this habit will be to put a rubber band around your wrist and snap it on the inner side of your wrist every time you cuss. It will be more annoying than painful, and eventually, you will refrain from cussing to avoid it.
At times, the subject imagines the association between an undesirable behavior and an unpleasant consequence, instead of actually engaging in it, and avoids it altogether, in what is known as covert sensitization. It is used for the treatment of alcoholism, obesity, etc. As opposed to this, cases where nausea- or fear-inducing drugs are used are considered cases of overt sensitization.
Aversive Conditioning Examples
✦ Nail biting, or onychophagia, is one of the several bad habits that can be treated using the aversive conditioning technique of unlearning. In this case, a foul- or bitter-tasting liquid is applied to the nails of a habitual nail biter. So, every time the person takes his hand to his mouth, he tastes it. The unpleasant experience helps in reducing nail biting―the undesired behavior in this case.
✦ It also comes handy when it comes to alcohol abuse and smoking. In the case of aversive conditioning for alcoholics, a nausea-inducing agent is added to alcohol. The unpleasant experience that follows reduces the positive feelings associated with alcohol. Over the course of time, even the thought of consuming alcohol makes the person nauseous, and therefore, he is able to get rid of this habit.
✦ In children, aversive conditioning is used for the treatment for enuresis or bed-wetting. A wetness sensor-equipped pad is placed in the child’s bed and connected to an alarm. The moment the child starts wetting the bed, the alarm goes off, forcing the child to wake up and go to the bathroom. With time, the child starts associating the act of bed-wetting with the inconvenience it causes, and stops it.
The moment the child starts wetting the bed, the alarm goes off, forcing the child to wake up and go to the bathroom. With time, the child starts associating the act of bed-wetting with the inconvenience it causes, and stops it.
Similarly, the technique can also be used to get rid of the habit of thumb-sucking in children, by applying a foul-tasting liquid on their thumb.
The use of aversive conditioning as a therapeutic technique is on a decline, mainly because of the fact that its effects are context-specific. If conditioned to do so, an individual may stop consuming alcohol in clinical settings―even that will be for a specific time, but the same cannot be said about situations outside the clinic.
Like it? Share it!
Uncategorized
Get Updates Right to Your Inbox
Sign up to receive the latest and greatest articles from our site automatically each week (give or take)...right to your inbox.
Blog UpdatesEmail Address *
Aversive conditioning - Psikhologos
Aversive conditioning - replacement of a positive conditioned response with a negative one, conditioning through negative reinforcement, and even more precisely - through the development of aversion (aversion - disgust). This form of behavioral psychotherapy is based on the formation of a connection between unwanted behavior and a subjectively unpleasant experience. The procedure of aversive psychotherapy consists in the fact that stimuli that cause the patient extremely unpleasant, but not dangerous for his life, sensations (electric shock, pain, horror, frustration of needs), are presented in temporal proximity with such stimuli (for example, alcohol) that provoke unacceptable and therefore inhibited behavior. In accordance with the scheme of classical conditioning, the stimulus that triggers the unwanted behavior is associated with the aversive stimulus and is saturated with negative affects. Currently, symbolic aversive conditioning is increasingly used, when the irritant of unacceptable behavior is associated with negative ideal ideas (ideal ideas about illness, social isolation, etc.). When an operant conditioning scheme is used, the aversive stimulus is associated not with a stimulus but with a response, such as in bedwetting or self-injurious behavior.
This form of behavioral psychotherapy is based on the formation of a connection between unwanted behavior and a subjectively unpleasant experience. The procedure of aversive psychotherapy consists in the fact that stimuli that cause the patient extremely unpleasant, but not dangerous for his life, sensations (electric shock, pain, horror, frustration of needs), are presented in temporal proximity with such stimuli (for example, alcohol) that provoke unacceptable and therefore inhibited behavior. In accordance with the scheme of classical conditioning, the stimulus that triggers the unwanted behavior is associated with the aversive stimulus and is saturated with negative affects. Currently, symbolic aversive conditioning is increasingly used, when the irritant of unacceptable behavior is associated with negative ideal ideas (ideal ideas about illness, social isolation, etc.). When an operant conditioning scheme is used, the aversive stimulus is associated not with a stimulus but with a response, such as in bedwetting or self-injurious behavior. Most often, aversive psychotherapy is used in the treatment of alcoholism, smoking, sexual disorders (here, as a rule, undesirable behavior is presented in videos).
Most often, aversive psychotherapy is used in the treatment of alcoholism, smoking, sexual disorders (here, as a rule, undesirable behavior is presented in videos).
How is it done?
For example, in the fight against overeating, a simple device with a battery is attached to the Big Mac, a person bites the Big Mac and receives a weak discharge. A trifle, but unpleasant. Similarly - if the hand reaches for a cigarette, we get a discharge for a cigarette. Coding for alcoholism is the same principle, although the gag reflex is more often used here. A glass to your mouth - and an attack of nausea or a feeling that you are dying.
It's unpleasant, but in a situation of choice - the future normal life or the loss of a family, or, even more so, a prison, people willingly go for it and get the desired result.
It is interesting that enuresis is treated in the same way: the child lies down on the bed, humidity sensors are placed under the sheets. The child has described himself - the light is turned on, the diaper is changed for the child. The child does not want to wake up. but this always happens, and usually enough to stop the enuresis. A few repetitions - the problem is solved.
The child does not want to wake up. but this always happens, and usually enough to stop the enuresis. A few repetitions - the problem is solved.
Once upon a time, at the dawn of research, they tried to use weak shocks of electric current as a negative reinforcement. Life has shown that there is no need for this: the usual diaper change is on time! - this function is fully performed.
Or, for example, unwanted sexual behavior, such as engaging in masturbation while replaying episodes of past exhibitionism in the mind, is repeatedly accompanied by an aversive stimulus. It can be, for example, a painful but harmless electric shock, or a nausea-inducing drug, or a very unpleasant odor. Similarly, an aversive stimulus may be presented to a person while viewing photographs or color slides depicting paraphilic behavior.
A recent study reports some success with the aversive conditioning technique in treating exhibitionism. Several such male perpetrators were instructed to carry smelling salt (a very unpleasant odor) with them, which they were to inhale deeply whenever they felt the urge to expose their genitals. This approach has helped some of the perpetrators develop some control over their paraphilic behavior. This was due to their association between the disgusting smell and their deviant fantasies/urges (Marshall et all., 1991).
This approach has helped some of the perpetrators develop some control over their paraphilic behavior. This was due to their association between the disgusting smell and their deviant fantasies/urges (Marshall et all., 1991).
Aversive conditioning is a rather unpleasant procedure. And you may wonder why a paraphilic would agree to be subjected to it voluntarily. The answer is that aversive conditioning as a treatment for coercive paraphilias is most often applied to men who have been sentenced to coercive treatment by a court order. But sometimes family pressure or personal dissatisfaction with the complications associated with paraphilic behavior lead some men to voluntarily seek therapeutic intervention.
Aversive therapy
02/13/2012
Aversive therapeutic techniques (lat. aversio - disgust) underlay the practical application of experimental learning theories. Currently, they can be divided into methods based on the I. P. Pavlov model (classical conditioning) and on the Skinner model (operant conditioning).
P. Pavlov model (classical conditioning) and on the Skinner model (operant conditioning).
Techniques based on classical conditioning combine an attractive stimulus (such as alcohol or a large meal) with a painful, unpleasant, aversive stimulus (apomorphine injection causing vomiting, electrical shock causing severe pain, etc.) . The technique is criticized due to ethical considerations. However, most authors recognize the possibility and necessity of using it for health reasons, for example, in severe cases of obsessive self-harm, pressure on the eyes, etc.
The conditions for successful application are the same as in the punishment technique. The aversive stimulus should be applied immediately after the response to be extinguished. At the first stage, it is necessary to apply a constant extinction scheme, gradually switching to the irregular use of the aversive stimulus. Treatment should continue for some time after the disappearance of the symptom. An adequate indicator for discontinuation of treatment is the emergence of adaptive behavior. The use of this technique assumes the presence of clear-cut and time-limited symptoms.
The use of this technique assumes the presence of clear-cut and time-limited symptoms.
Techniques that use the operant model are based on the principle of successfully solving a problem that relieves the patient of unpleasant stimuli, such as an electric shock. So, in the treatment of the tremor form of writing spasm, the patient masters the task of getting a metal stick into a series of holes of ever-decreasing diameter. The presence of tremor leads to getting into the edges of the holes and to the closure of the electrical circuit; the patient receives an electric shock. An accurate hit in these holes saves him from an electrical discharge. In the spastic form of writing spasm, the patient uses a special fountain pen, excessive pressure on which also leads to an electrical circuit and, consequently, to punishment. In the process of training, the patient learns to relax the desired muscle groups.
With appropriate technical ingenuity, for almost every symptom, it is possible to create a technique based on the principle of problem solving, i. e., preventing the impact of an aversive stimulus. An example is a patient who suffered from hysterical paralysis of the legs and loss of sensation in the legs. Electrodes were placed on the legs and two fingers of her hand: on the fingers of the hand - electrodes through which the patient could receive a painful electrical discharge, and on the legs - electrodes through which weak electrical stimulation was carried out, captured with intact sensitivity and not bearing a painful character. The patient was given instructions: if you get any sensations from the electrodes on your legs, press the switch, otherwise, after 5 seconds, a strong, painful electric discharge will follow in your fingers. The patient had to solve the problem of distinguishing between a weak stimulus, involuntarily lowering the threshold of pain sensitivity. During the first procedure, the patient showed no avoidance reactions and received several painful electric shocks. During the second procedure, after the first electrical discharge, pronounced vegetative reactions and even vomiting appeared.
e., preventing the impact of an aversive stimulus. An example is a patient who suffered from hysterical paralysis of the legs and loss of sensation in the legs. Electrodes were placed on the legs and two fingers of her hand: on the fingers of the hand - electrodes through which the patient could receive a painful electrical discharge, and on the legs - electrodes through which weak electrical stimulation was carried out, captured with intact sensitivity and not bearing a painful character. The patient was given instructions: if you get any sensations from the electrodes on your legs, press the switch, otherwise, after 5 seconds, a strong, painful electric discharge will follow in your fingers. The patient had to solve the problem of distinguishing between a weak stimulus, involuntarily lowering the threshold of pain sensitivity. During the first procedure, the patient showed no avoidance reactions and received several painful electric shocks. During the second procedure, after the first electrical discharge, pronounced vegetative reactions and even vomiting appeared. During the third procedure, the patient pressed the switch button twice in a row, preventing the delivery of a painful electric discharge in time, and noted at the same time that she had sensitivity in her legs. At the same time, she developed voluntary movements in her legs, and the patient was able to go to the ward on her own. Subsequently, there was no recurrence of symptoms, and after a few days she was discharged.
During the third procedure, the patient pressed the switch button twice in a row, preventing the delivery of a painful electric discharge in time, and noted at the same time that she had sensitivity in her legs. At the same time, she developed voluntary movements in her legs, and the patient was able to go to the ward on her own. Subsequently, there was no recurrence of symptoms, and after a few days she was discharged.
Aversive therapy is used in the treatment of alcoholism, chronic nicotinism and other diseases.
Keywords: Therapy
Source: B. Karvasarsky, Psychotherapeutic Encyclopedia
| Related materials |
|---|
| Body-oriented therapy exercises Starshenbaum G.V., Group psychotherapist |
| Psychosocial therapy and rehabilitation of patients with schizophrenia Psychiatry.    Copyright © · The Wright Initiative · Articles · Site Map 
|