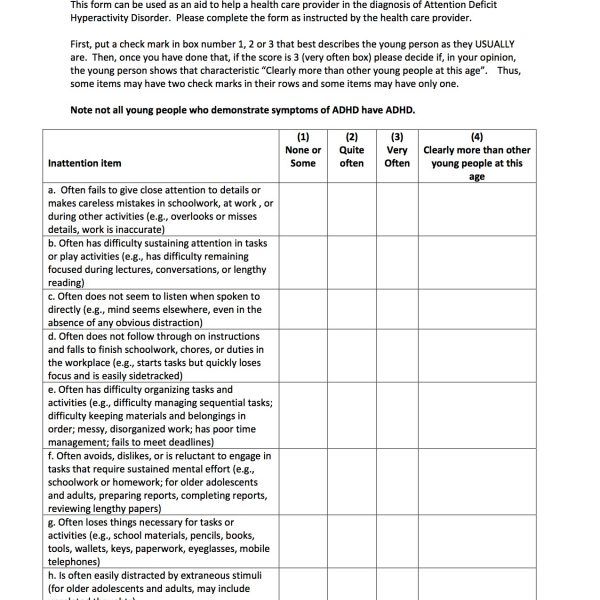
Attention deficit disorder checklist for children
Symptom Test for Kids, Tweens & Teens
Does My Child Have ADHD? Signs and Symptoms of ADHD in Kids
Common signs of attention deficit disorder (ADHD or ADD) in children include:
- difficulty focusing
- difficulty controlling impulses
- inability to make friends
- habitually disorganized and running late
- overly energetic
Your child will not (and should not) receive a formal ADHD diagnosis just because he is distractible or restless.
He or she must meet the criteria for ADHD symptoms in children outlined in the Diagnostic and Statistical Manual of Mental Disorders, which also specifies where and how often signs of ADD must be exhibited and the extent to which they must interfere with daily life before a diagnosis is warranted.
[Interactive Screener: Could Your Child Have Signs of ADHD?]
ADHD in Children: A Symptom Self-Test for Kids
Check off each of the following statements that applies to your child in the following ADHD test for kids:
NOTE: This ADHD test for kids is not intended to diagnose or to replace the care of a health care professional.
What Are the Signs of ADD Distractibility? Symptoms of ADHD with Inattention
The first part of the ADHD test for kids covers signs of distractibility. These signs are sometimes called inattentive symptoms, or previously, ADD symptoms in children.
- My child has trouble paying attention.
- My child makes careless mistakes.
- It’s very difficult for my child to stay focused on homework or other tasks.
- My child rarely completes an activity before moving to the next activity.
- Even when spoken to directly, my child seems to not listen.
- My child is disorganized and even with my help can’t seem to learn how to become organized.
- My child loses things necessary for tasks or activities, such as toys, homework assignments, pencils, books, and so on.
- My child tries to avoid activities or does them grudgingly when they require sustained concentration and a lot of mental effort.
- My child frequently forgets to do things, even when constantly reminded.
- Even the smallest distractions throw my child off task.
- My child has trouble following instructions and finishing tasks.
If you checked off five or more symptoms — and these symptoms have been a persistent problem interfering in your child’s life at home and at school — he or she may have inattentive type ADHD. It would be prudent to talk with a physician or a licensed mental health practitioner.
[Download: In-Depth Guide to Inattentive ADHD]
What Are the Signs of ADHD Hyperactivity in Kids?
The second part of the ADHD test for kids covers hyperactivity and impulsivity.
- Sometimes my child acts as if she/he is driven by a motor and is constantly “on the go.”
- My child always seems to be squirming in the chair or fidgeting.
- No matter how hard he/she tries, my child has problems remaining seated even when she/he is supposed to — he/she gets up, runs around, or climbs during class or in other situations where one should stay seated.
- My child talks a lot, even when she/he has nothing much to say.
- My child often interferes in the classroom because she/he has difficulty engaging in quiet activities without disturbing others.
- In class or at home, my child blurts out answers to questions before they are fully asked.
- My child has difficulty waiting patiently to take turns, and frequently butts ahead in lines or grabs toys from playmates.
- Sometimes my child seems intrusive. She/he interrupts constantly other peoples’ activities, conversations, and games.
If you checked off five or more symptoms — and these symptoms have been a persistent problem interfering in your child’s life at home and at school — he or she may have attention deficit disorder. It would be prudent to talk with a physician or a licensed mental health practitioner.
Take this form with you to the doctor’s office. Treatments are available for ADHD in children that can reduce substantially these neurologically based behaviors.
What To Do Next:
1. Download The Parents’ Guide to ADHD Medications
2. Take This Test: Does My Child Have ADHD / ADD?
3. Take This Test: Oppositional Defiant Disorder in Children
4. Take This Test: Sensory Processing Disorder in Children
5. Understand How ADHD is Diagnosed in Children65. Find an ADHD specialist nearby in our ADDitude Directory
6.Listen to Dr. William Dodson Explain How ADHD Shapes Perceptions, Emotions & Motivation
7.Consult Our Treatment Guide for Children
Previous Article Next Article
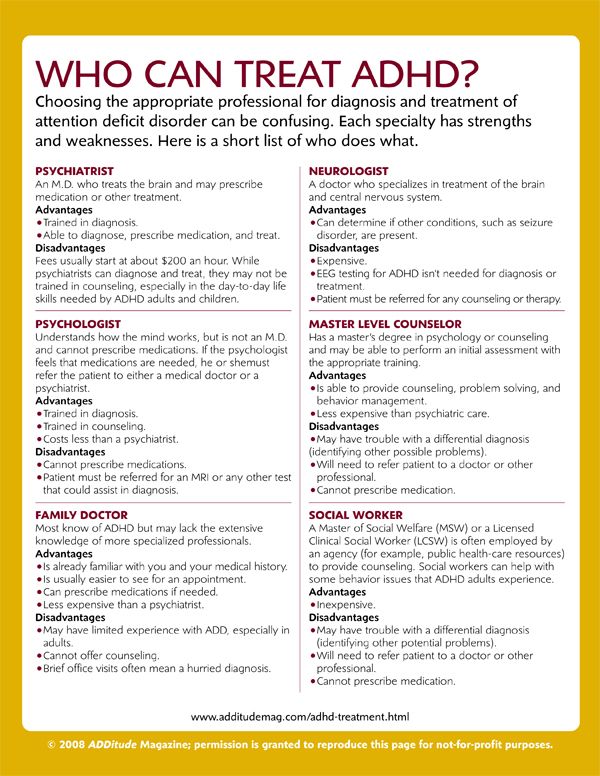
Tricity Family Medicine:
Centers for Disease Control and Prevention –http://www.cdc.gov
Familydoctor.org – http://familydoctor.org/familydoctor/en.html
HealthyWomen – http://www. healthywomen.org/
healthywomen.org/
Healthy Men – http://www.ahrq.gov/patients-consumers/patient-involvement/healthy-men/index.html
American Academy of Pediatrics – http://www.healthychildren.org
This comprehensive site from the American Academy of Pediatrics for parenting kids from prenatal until adulthood covers diseases, staying healthy, mental and social concerns, school problems, and safety. Parents of prospective and new teen drivers will appreciate the site’s Teen Driving Agreement.
SuperKids Nutrition – http://www.superkidsnutrition.com/
SuperKids Nutrition was founded by a registered dietician to promote good nutrition; it offers health information for parents, kids and health educators through a blog, activities and links to even more online resources. For parents, there are tips and toolkits to promote healthy living in the family. For kids, an animated SuperKids Crew teaches about nutrition, and there are fun activities to print and complete.
Teen Health – http://www.nlm.nih.gov/medlineplus/teenhealth.html
This MedlinePlus page was created for teens and parents. There are links to information on nutrition, emotions, body image, alcohol, drugs, sexuality, and other topics of interest to adolescents.
Academy of Nutrition and Dietetics–Eatright.org – http://www.eatright.org/
The Academy of Nutrition and Dietetics is the best source of accurate, credible and timely food and nutrition information for the public. The website includes information on nutrition throughout the lifecycle, advice for achieving and maintaining a healthy weight, information on prevention and management of diseases, and a searchable database of registered dietitian nutritionists.
Weight loss website – www.sparkpeople.com
It’s an online dieting community, but SparkPeople.com also places a huge emphasis on adopting a healthy lifestyle for long-term weight maintenance. The site is packed with useful tools and resources for you to explore. The fitness, recipe, and cooking videos are all easy to follow, and the motivational quizzes and success stories help to keep you on target with your goals.
The site is packed with useful tools and resources for you to explore. The fitness, recipe, and cooking videos are all easy to follow, and the motivational quizzes and success stories help to keep you on target with your goals.
Weight loss website –www.Calorie-Count.com
Calorie-Count.com lets you log your food intake and workouts, but also offers great tips for beginner exercisers and expert dieting advice. In addition, there’s a mobile-friendly version of the site so you can stay on top of recording what you’ve eaten even on the go.
Weight loss website – www.MyFitnessPal.com
MyFitnessPal.com Logs has easy-to-understand charts for tracking your progress and also shows you a count of how many calories you have “left” to consume for the day to keep you on track with your goals.
The AGS Foundation for Health in Aging – http://www.healthinaging.org
Health In Aging provides up-to-date information on healthcare and aging for older adults, caregivers, and providers. The site provides information and tip sheets on common health topics and resources to help find and communicate with geriatrics healthcare providers. Information is easy to understand and available in English only. The site was created by the American Geriatrics Society’s Health in Aging Foundation and is overseen by elder care experts.
The site provides information and tip sheets on common health topics and resources to help find and communicate with geriatrics healthcare providers. Information is easy to understand and available in English only. The site was created by the American Geriatrics Society’s Health in Aging Foundation and is overseen by elder care experts.
Benefits Checkup – https://www.benefitscheckup.org/
Benefits Checkup is a service aimed at helping older adults finds state, federal and private benefits programs to help pay for prescriptions, healthcare, food, and other services. Older adults can answer a series of questions and receive information and applications for programs for which they may be eligible. The site also contains links to forms and resources for local and national programs. Information is in English, although many forms are available in multiple languages. The site is a service of National Council on Aging, a non-profit and advocacy organization for older adults.
Eldercare Locator – http://www.eldercare.gov/
Eldercare Locator, service of the U. S. Administration on Aging, connects older adults and caregivers to services for seniors. The online search function provides lists of trusted local resources, organizations, and services. There are also factsheets and links to online information about medicine and health, advanced care planning, and other issues. A hotline and online chat connects to Eldercare information specialists who can answer detailed questions. Online information is available in English; information in other languages is available by phone.
The Family Caregiver Alliance – http://www.caregiver.org
Family Caregiver Alliance (FCA) provides information, services, and support for caregivers and families of persons with chronic, disabling health conditions. The website offers fact sheets on conditions such as dementia, Parkinson disease, and stroke as well as statistics, public policy information, and reports. It includes caregiver advice and tips and hosts online discussion groups. Information is available in English, Spanish, Chinese, Korean, and Vietnamese. The FCA is a nonprofit, community-based organization.
It includes caregiver advice and tips and hosts online discussion groups. Information is available in English, Spanish, Chinese, Korean, and Vietnamese. The FCA is a nonprofit, community-based organization.
Medicare.gov – http://www.medicare.gov/
The official U.S. government website provides a wealth of information on Medicare health plans, drug coverage, and costs. It also offers tools to find whether a test, item, or service is covered and for finding doctors, providers, hospitals, plan, and suppliers. Online forms are provided for applying to the program, replacing a Medicare card, or changing an address. Information is available in English and in Spanish.
Medicine Safety: A Toolkit for Families – http://www.learnaboutrxsafety.org/
This excellent resource encompasses safe use, storage, and disposal of drugs; questions for your doctor and pharmacist; drug interactions and side effects; plus drugs of special concern for seniors and links to other resources. Medicine Safety is produced by the Center for Improving Medication Management (CIMM) and the National Council on Patient Information and Education (NCPIE).
Medicine Safety is produced by the Center for Improving Medication Management (CIMM) and the National Council on Patient Information and Education (NCPIE).
Needy Meds – http://www.needymeds.org
Needy Meds is an information clearinghouse of the various assistance programs available from pharmaceutical manufacturers for patients who cannot afford medications. It also has information about government assistance programs and coupons.
RxList-The Internet Drug Index – http://www.rxlist.com
This site has information about prescription and non-prescription drugs, herbs, and supplements, and is searchable by generic and brand name. It also has a useful pill identifier tool, information and slide shows about diseases and health topics, and a medical dictionary.
National Center for Complementary and Integrative Health (NCCIH) – https://nccih.nih.gov/
The National Institutes of Health established NCCIH to study the safety and efficacy of complementary and alternative therapies.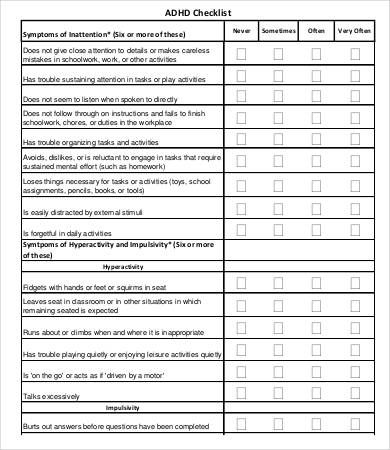 The website provides evidence-based information about these therapies, advice about choosing practitioners, and information about herbs and supplements.
The website provides evidence-based information about these therapies, advice about choosing practitioners, and information about herbs and supplements.
Patient Decision Aids: https://decisionaid.ohri.ca/AZlist.html
Diabetes Decision aid – https://diabetesdecisionaid.mayoclinic.org/
90,000 ADHD (Attention Deficit Hyperactivity Disorder). Lecture for teachers.Aleksandrova T.V., teacher-psychologist GBU DO TsPMSP Vasileostrovskiy district
various pathologies. Especially "lucky with advertising" neurological pathologies. They allegedly expand and multiply with indomitable speed, and some especially tabloid newspapers and magazines are very fond of throwing catchy headlines on the cover like “There are no more healthy children in St. Petersburg” or “A generation of freaks is coming!”. In some ways, they, newspapers and magazines, of course, can be understood, since competition in the publishing world is very high. Yes, and there are objective reasons for concern. But the attentive reader must approach all these "revelations" with great caution. And don't panic ahead of time. That's why. nine0007
Yes, and there are objective reasons for concern. But the attentive reader must approach all these "revelations" with great caution. And don't panic ahead of time. That's why. nine0007
- In the last two decades of the past century, the diagnosis of neurological diseases in young children has changed and improved dramatically. In addition to the traditional neurological hammer, new research methods have appeared and become widespread, such as ultrasound diagnostics, tomography, and sonography. Based on this, it can be assumed that many neurological defects in newborns and young children were simply not diagnosed before, and therefore were not included in the statistics. That is, there were fewer not sick, but diagnoses. nine0012
- New groups of drugs have appeared that improve blood circulation in the brain, stimulate learning and memory, and gently affect other higher integrative functions of the brain. At the same time, they have a minimum of side effects. Naturally, practitioners use them in a wider range of cases.
 A child with minimal disorders, who twenty or even ten years ago would have been left without treatment at all (or prescriptions would have been limited to massage and vitamin intake), is now receiving drug therapy (for example, some drug from the nootropic group that has a positive neurometabolic effect). nine0012
A child with minimal disorders, who twenty or even ten years ago would have been left without treatment at all (or prescriptions would have been limited to massage and vitamin intake), is now receiving drug therapy (for example, some drug from the nootropic group that has a positive neurometabolic effect). nine0012 - The common newspaper and magazine thesis that, they say, there used to be a wonderful ecology, everyone ate natural products, lived in nature and therefore were healthy, like astronauts, does not stand up to elementary criticism. We should not forget that even 159 years ago, the average life expectancy in Russia was about 40 years (mainly due to the colossal mortality of young children). Returning to psychoneurology, it is also worth remembering that in every small Russian village there was a “fool”, “relaxed” and a few simply “weak-minded”, and these were already grown-up characters. And how many of them were selected by "natural selection" during infancy and early childhood! So the stories about ancient blessed times, when everyone was smart and healthy, is just one of the variants of the legend about milk rivers with jelly banks, etc.
 (1 p.28)
(1 p.28)
So, how are things in reality?
The relevance of the study of attention deficit hyperactivity disorder is determined by the high prevalence of this disease and the high degree of social maladaptation that occurs against its background. Domestic data on the prevalence of ADHD:
- N.N. Zavadenko et al. (2005) show that out of the total number of examined Moscow schoolchildren, signs of ADHD are observed in 7.6% of children; nine0011 Results of comparative epidemiological studies conducted by I.P. Bryazgunov and E.V. Kasatkina (2001, 2002) show that ADHD occurred in 18% of cases in Moscow, in 15% of cases in Shatura, and in 17% of cases in Vladimir.
- The results of various epidemiological studies by Western scientists indicate a significant spread of data on the spread of the disease from 4 - 12%.
Such a wide range of values is due to the use of different diagnostic criteria and the lack of uniformity in the study groups.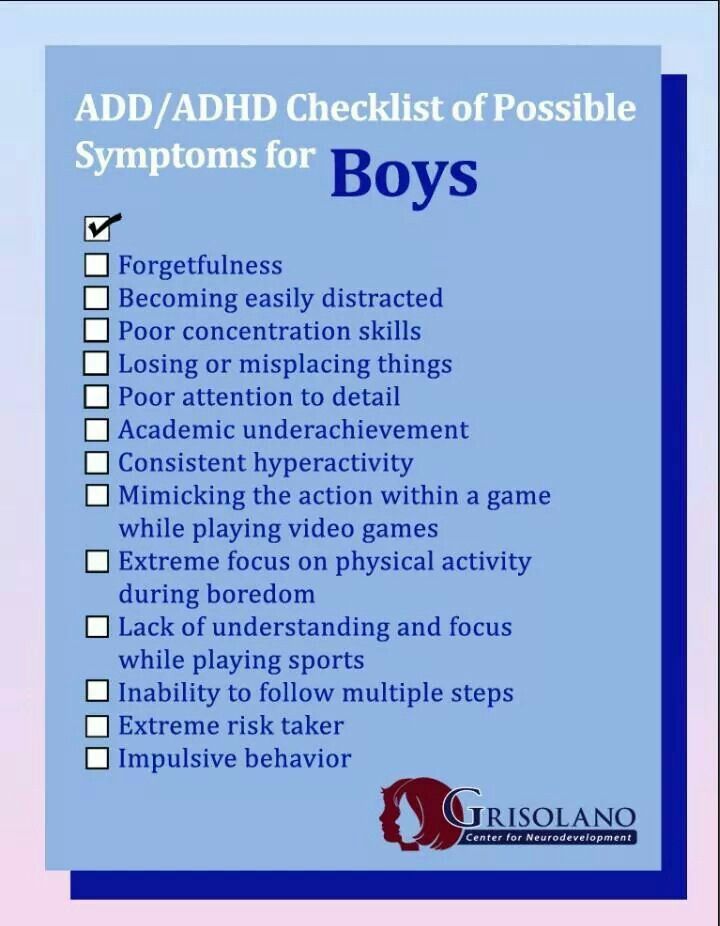 nine0007
nine0007
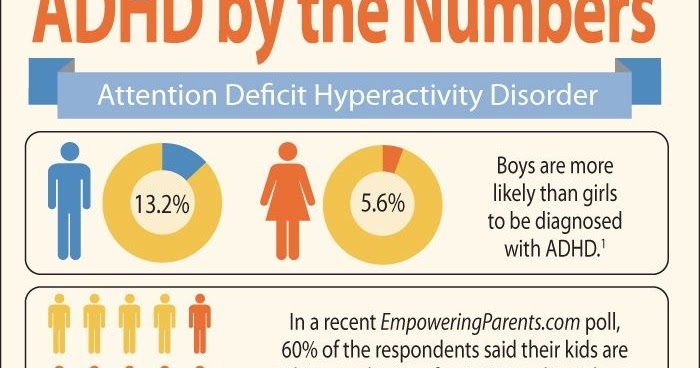
ADHD is 3-4 times more common in males. The relative predominance of ADHD among boys is explained by a number of reasons:
- the influence of genetic factors;
- higher vulnerability of male fetuses to various exposures;
- a greater degree of specialization of the cerebral hemispheres in boys compared to girls, which leads to a smaller reserve of compensatory capabilities in case of damage to brain systems that provide higher nervous activity. nine0012
- In addition, ADHD in boys is recorded more often due to their aggressive behavior, and inattention in girls is much less often accompanied by destructive behavior.
ADHD occurs in children of all socioeconomic groups. At the same time, a number of authors note that somewhat more often ADHD is recorded in low-income segments of the population. This fact can be explained by the fact that social factors often cause concomitant behavioral problems of a criminal nature. Also, ADHD is more common in regions with high population density.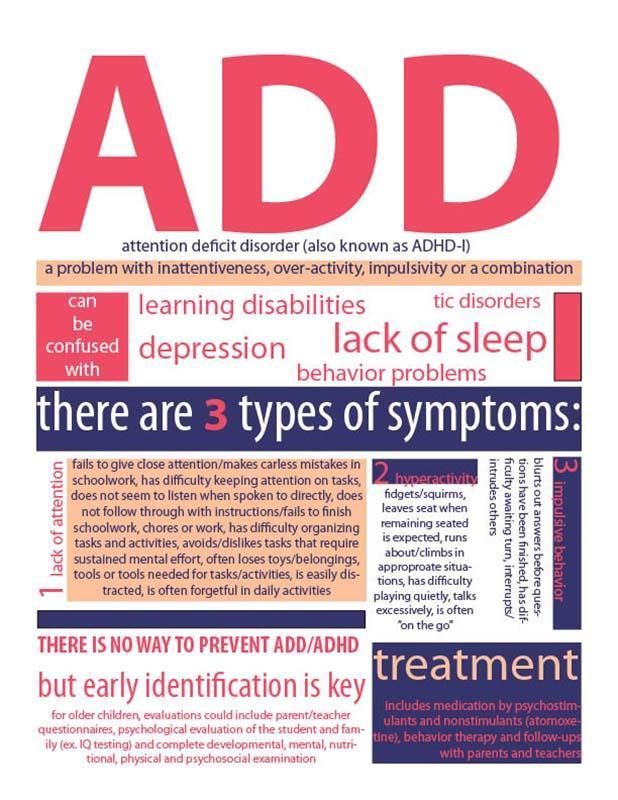 nine0007
nine0007
Clinical manifestations of the disease are determined by three main symptom complexes: inattention, hyperactivity and impulsivity.
- Carelessness. Speaking of ADHD, they most often mean increased distractibility and reduced concentration in such children.
- Hyperactivity. Hyperactivity in children with ADHD is usually understood as increased motor (motor) activity. Parents complain "it seems that a motor has been connected to the child." Unlike simply energetic children, activity in children with ADHD is aimless. nine0012
- Impulsivity. Impulsivity is understood as the impossibility of controlling one's impulses. Impulsive children cannot wait their turn when playing. In a learning situation, such children have an “impulsive work style”: they shout out answers in the lesson without fully answering them, interrupting other students or teachers. Due to impulsiveness, children often get into dangerous situations without thinking about the consequences.
 The propensity to take risks causes injuries and accidents. Impulsivity is often combined with aggressive and oppositional behavior. nine0012
The propensity to take risks causes injuries and accidents. Impulsivity is often combined with aggressive and oppositional behavior. nine0012
A number of researchers believe that in the case of hyperdynamic syndrome we are dealing only with the consequences of birth trauma. Others believe that along with a possible injury, there are also violations of the biochemical balance in the central nervous system. A group of doctors from St. Petersburg suggests that the key to this common disease lies in a violation of the blood circulation of the brain.
Neuroanatomical changes in ADHD affect mainly the connections between the frontal cortex and the basal ganglia, with predominant localization in the right hemisphere. The study of brain metabolism in ADHD using tomography showed a decrease in metabolic activity in the frontal areas of the brain. It is assumed that the identified neuroanatomical and hemodynamic disorders can cause a decrease in the inhibitory control of motor activity, which is provided mainly by the frontal cortex and the caudate nucleus. nine0007
nine0007
For parents and teachers, non-scientific terminology of specialists is much more important. It is important for them to understand what exactly happens to a child who has been diagnosed with hyperdynamic syndrome. Let's try to explain.
- For one reason or another, the brain of a child (usually a newborn) was slightly damaged, that is, part of the brain cells simply does not function.
- Nerve cells, as you know, do not recover, but immediately after an injury, other, healthy nerve cells begin to gradually take over the functions of the injured, that is, the recovery process begins immediately. nine0012
- At the same time, the process of normal age development of the child is going on. He learns to sit, walk, talk, etc. Both the recovery process and the process of normal age-related development require energy. Consequently, from the very beginning, the nervous system of our child with hyperdynamic syndrome works with a double load.
- In the event of stressful situations, prolonged tension (for example, preparation for an annual test or testing at a prestigious gymnasium), or after somatic diseases, a hyperdynamic child may experience a deterioration in the neurological condition, increased behavioral disturbances and learning problems.
 nine0012
nine0012 - There are two main processes in the nervous system - excitation and inhibition. In hyperdynamic syndrome, structures that provide the process of inhibition are affected. That is why our child has difficulty with concentration, voluntary attention and regulation of his activity.
- With a successful development of events, sooner or later the functions of all the affected cells will be "taken apart" by other, healthy cells, the necessary connections will be restored (usually this happens by the age of 14-15). The process of "restoring the economy" is completed, and the child (adolescent) no longer differs from his healthy peers. In scientific language, this process is called convalescence (reverse development) of the syndrome. nine0012
Control Characteristic features of the behavior of different categories of children
(see at the end of the text)
Well, what to do with it?
- It is generally accepted that the treatment of ADHD should be comprehensive , that is, it should include both drug therapy, psychotherapeutic methods, and an individual approach at school.
- More than other children, they need positive reinforcement for their success. nine0012
- In a clear formulation of the requirements for them, phased (setting goals for the child and slowly approaching them).
- Daily routine (which disciplines and helps the child gain experience in organizing his time and space)
- Practically all the people surrounding a hyperdynamic child (parents, teachers, even classmates) are in the inevitable confidence that the child can completely get rid of all problems and shortcomings, simply by "pulling himself together", "getting together", etc. Unfortunately they are wrong. nine0012
- For some time, each hyperdynamic child will meet the expectations of the people around him, "exert his will", "take care of himself" and follow other equally valuable advice. Gradually, however, both he and others are convinced that all this does not bring any success. Moreover, the more a child is shamed and scolded, the worse things get for him.
 N.s. The child's HD, already working with overload, receives an additional load.
N.s. The child's HD, already working with overload, receives an additional load.
Further, the situation can develop in several ways:
- the child gives up and simply spit on the opinions of others. He goes to the street, where his peers admire his recklessness, desire to assert himself, activity.
- another child with poorer health begins to suffer from many and varied somatic diseases.
- the third child is the strongest and most courageous, despite all the difficulties, continues to fight for a place under the sun, trying to somehow adapt to the circumstances in which, as if on purpose, everything is against him. Sometimes he succeeds - he becomes the forward of the school football team, or the singer in the school ensemble, or the "great chemist", or the school humorist's notebook, or just a cool jester. All this, as a rule, is done against the will of the family and the teaching staff. But when the place is found, everyone breathes a sigh of relief - the manifestation of the syndrome sharply subsides.
 nine0012
nine0012
When organizing educational activities, it is important to remember:
- the need to change activities
- Enable creative tasks
- children with ADHD often like to do things with their hands
- Working with the emotional state of the child
"Ambulance" when working with a hyperactive child
- Distract the child from his whims.
- Offer a choice (another activity that is currently possible). nine0012
- Ask an unexpected question.
- React in a way that is unexpected for the child (joking, repeating the child's action).
- Do not categorically forbid the child's action.
- Do not order, but ask (but do not fawn).
- Listen to what the child wants to say (otherwise he will not hear you).
- Automatically, with the same words, repeat your request many times (in a neutral tone). nine0012
- Leave alone in the room (if it is safe for his health).
- Do not insist that the child apologize at all costs.
- Do not read notations (the child still does not hear them).
LITERATURE
- Murashova E.V. Children-"mattresses" and children-"catastrophes": Hypodynamic and hyperdynamic syndrome. - Yekaterinburg: U-Factoria, 2005
- Monina G.B., Lyutova-Roberts E.K., Chutko L.S. Hyperactive children: psychological and pedagogical assistance. Monograph. - St. Petersburg: Speech, 2007
- Lyutova E.K., Monina G.B. Cheat sheet for parents: Psychocorrective work with hyperactive, aggressive, anxious and autistic children. - St. Petersburg: Publishing house "Rech"; "TC Sphere", 2002.
- Monina G.B., Panasyuk E.V. Interaction training with a failing student. - St. Petersburg: Rech Publishing House, 2006
Listen to your child
Take time today
And listen to what the child is trying to tell you.
Listen to him today, no matter how busy you are,
Or he won't listen to you.
Find out about his troubles,
Find out about his needs,
Celebrate his little triumphs with him,
Praise him for his exploits,
Listen to his chatter,
Make him laugh,
Ask him what the matter is,
Ask what happens next ,
But tell him every night that you love him.
And even scolding the child,
Do not forget to support him.
And say, “It's all right!
Tomorrow everything will be fine”,
Find time today
And listen to what the child is trying to tell you.
Listen to him today, no matter how busy you are,
And then he will come back to listen to you.
(Cherie Fuller "Choose the key to teaching your child." Minsk, 1998)
Characteristic features of the behavior of different categories of children
CHILD
- overly talkative
- works productively on operational cards
- refuses to play collectively nine0011 excessively mobile
- has high demands on himself
- does not understand the feelings and experiences of other people
- feels rejected
- loves rituals
- has low self-esteem
- often quarrels with adults
- creates conflict situations
- is behind in development
- overly suspicious
- spinning in place
- makes stereotypical mechanical movements
- controls his behavior
- overly worried about any events
- blame others
- restless in movements
- has somatic problems: abdominal pain, headaches
- often argues with adults
- fussy
- seems detached, indifferent to the environment
- likes to do puzzles, mosaics
- losing control
- refuses to comply with requests
- impulsive
- poorly oriented in space
- often fights
- has missing look
- often anticipates "bad"
- self-critical
- unable to adequately evaluate his own behavior
- has muscular tension - enjoys collecting
- has poor coordination
- afraid to enter into a new activity
- often deliberately annoying adults
- asks many questions but rarely waits for answers
- shy hello
- plays the same game for years
- sleeps little and restlessly
- refers to himself in the 2nd and 3rd person
- pushes, breaks, crushes everything around
- feels helpless
- hits and drops objects
- envious, vindictive nine0011 avoids direct stares
- behaves uniformly
- irritable
- easily distracted
- often suffers from headaches, spasms
- blames others for his mistakes
- seeks to piss off mom, caregivers
- avoids contact with adults
- afraid of losing control
- has good mechanical memory
- thinks he's as good as the others
- does not want to be separated from parents
- has a low level of empathy
- clumsy
- avoids contact with children
- often angry and refusing to do anything
Attention deficit hyperactivity disorder in children | Zinov'eva
1. Polanczyk G, de Lima MS, Horta BL, et al. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2007;164(6):942–8. DOI:
Polanczyk G, de Lima MS, Horta BL, et al. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2007;164(6):942–8. DOI:
2. Bryazgunov IP, Kasatikova EV. Attention deficit with hyperactivity in children. Moscow: Medpraktika; 2002. 128 [Bryazgunov IP, Kasatikova EV. Defitsit vnimaniya s giperaktivnost'yu u detei [Deficiency of attention with a hyperactivity at children] Moscow: Medpraktika; 2002. 128 p. (In Russ.)]
3. Zavadenko NN. Hyperactivity and deficiency of attention at children's age, Moscow: ACADEMIA, 2005, 256 p. In Russ.)]
4. Biederman J, Kwon A, Aleardi M, et al. Absence of gender effects on attention deficit hyperactivity disorder: findings in nonreferred subjects. Am J Psychiatry. 2005;162(6):1083–9. DOI: http://dx.doi.org/10.1176/appi.ajp.162.6.1083.
5. Diagnostic and Statistical Manual of Mental Disorders.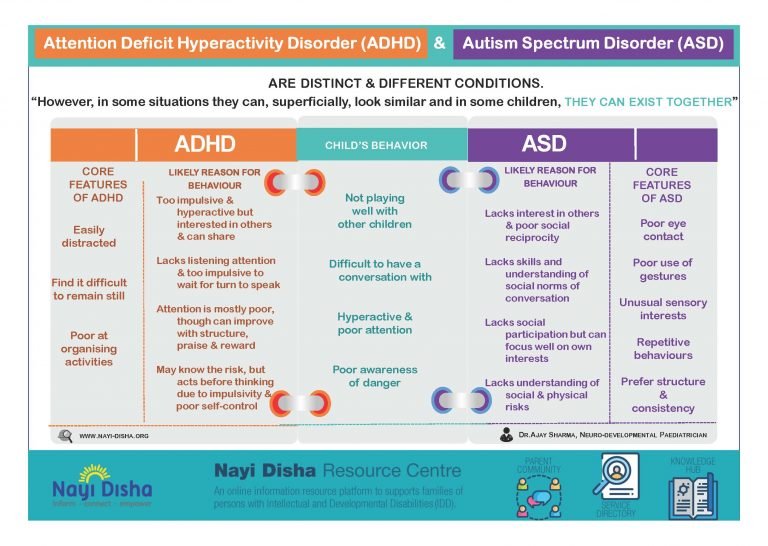 5th ed.: DSM-5. American Psychiatric Association. 2013.
5th ed.: DSM-5. American Psychiatric Association. 2013.
6. Aleksandrov AA, Karpina NV, Stankevich LN. Negativity of mismatch in evoked potentials of the brain in adolescents in the norm and with attention deficit upon presentation of acoustic stimuli of short duration. Russian Physiological Journal. THEM. Sechenov. 2003;33(7):671–5. [Aleksandrov AA, Karpina NV, Stankevich LN. Mismatch negativity in evoked brain potentials in adolescents in normal conditions and attention deficit in response to presentation of short-duration acoustic stimuli. Rossiiskii fiziologicheskii zhurnal im. I.M. Sechenova = Neuroscience and behavioral physiology. 2003;33(7):671–5. (In Russ.)]
7. Becker SP, Langberg JM, Vaughn AJ, Epstein JN. Clinical utility of the Vanderbilt ADHD diagnostic parent rating scale comorbidity screening scales. J Dev Behav Pediatr. 2012;33(3):221–8. DOI: 10.1097/DBP.0b013e318245615b.
8. Gorbachevskaya NL, Zavadenko NN, Sorokin AB, Grigorieva NV. Neurophysiological study of attention deficit hyperactivity disorder. Siberian Bulletin of Psychiatry and Narcology. 2003;(1):47–51. [Gorbachevskaya NL, Zavadenko NN, Sorokin AB, Grigor'eva NV. Neurophysiological research of a syndrome of deficiency of attention with a hyperactivity. Sibirskii vestnik psikhiatrii i narkologii. 2003;(1):47–51. (In Russ.)]
Siberian Bulletin of Psychiatry and Narcology. 2003;(1):47–51. [Gorbachevskaya NL, Zavadenko NN, Sorokin AB, Grigor'eva NV. Neurophysiological research of a syndrome of deficiency of attention with a hyperactivity. Sibirskii vestnik psikhiatrii i narkologii. 2003;(1):47–51. (In Russ.)]
9. Biederman J, Faraone S. Attention deficit hyperactivity disorder. Lancet. 2005;366(9481):237–48. DOI: http://dx.doi.org/10.1016/S0140-6736(05)66915-2.
10. Mick E, Faraone SV. Genetics of Attention Deficit Hyperactivity Disorder. Child Adolesc Psychiatr Clin N Am. 2008;17(2):261–84, vii-viii. DOI: 10.1016/j.chc.2007.11.011.
11. Haavik J, Blau N, Thö ny B. Mutations in human monoamine-related neurotransmitter pathway genes. Hum Mutat. 2008;29(7):891–902. DOI: 10.1002/humu.20700. nine0007
12. Schulz KP, Himelstein J, Halperin JM, Newcorn JH. Neurobiological models of attentiondeficit/hyperactivity disorder: a brief review of the empirical evidence. CNS spectra. 2000;5(6):34–44.
13. Arnsten AFT, Pliszka SR. Catecholamine influences on prefrontal cortical function: relevance to treatment of attention deficit hyperactivity disorder and related disorders. Pharmacol Biochem Behav. 2011;99(2):211–6. DOI: 10.1016/j.pbb.2011.01.020. Epub 2011 Feb 2.
14. McNally MA, Crocetti D, Mahone EM, et al. Corpus callosum segment circumference is associated with response control in children with attention-deficit hyperactivity disorder (ADHD). J Child Neurology. 2010;25(4):453–62. DOI: 10.1177/0883073809350221. Epub 2010 Feb 5.
15. Nakao T, Radua J, Rubia K, Mataix-Cols D. Gray matter volume abnormalities in ADHD: voxelbased meta-analysis exploring the effects of age and stimulant medication. Am J Psychiatry. 2011;168(11):1154–63. DOI: 10.1176/appi.ajp.2011.11020281. Epub 2011 Aug 24.
16. Valera EM, Faraone SV, Murray KE, Seidman LJ. Meta-analysis of structural imaging findings in attention-deficit/hyperactivity disorder. Biol Psychiatry. 2007;61(12):1361–9. DOI: http://dx.doi.org/10.1016/j.biopsych.2006.06.011. Epub 2006 Sep 1.
DOI: http://dx.doi.org/10.1016/j.biopsych.2006.06.011. Epub 2006 Sep 1.
17. Finger AB. Lectures on developmental neurology. Moscow: MEDpressinform; 2012. 376 p. [Pal'chik AB. Lektsii po nevrologii razvitiya [Lectures on development neurology]. Moscow: MEDprecsinform; 2012. 376 p. (In Russ.)]
18. Reddy DS. Neurosteroids: Endogenous role in the human brian and therapeutic potentials. Prog. Brain Res. 2010;186:113–137.
19. Shaw P, Eckstrand K, Sharp W, et al. Attention-deficit/hyperactivity disorder is characterized by a delay in cortical maturation. Proc Natl Acad Sci USA. 2007;104(49):19649–54. DOI: http://dx.doi.org/10.1073/pnas.0707741104. Epub 2007 Nov 16.
20. Fair DA, Posner J, Nagel BJ, et al. Atypical default network connectivity in youth with attention-deficit hyperactivity disorder. Biological psychology. 2010;68(12):1084–91. DOI: 10.1016/j.biopsych.2010.07.003. Epub 2010 Aug 21.
21. Makris N, Biederman J, Monuteaux MC, Seidman LJ. Towards Conceptualizing a Neural Systems-Based Anatomy of Attention-Deficit/Hyperactivity Disorder. Dev Neurosci. 2009;31(1–2):36–49. DOI: 10.1159/000207492. Epub 2009 Apr 17.
Dev Neurosci. 2009;31(1–2):36–49. DOI: 10.1159/000207492. Epub 2009 Apr 17.
22. Kaplan RF, Stevens MC. A review of adult ADHD: a neuropsychological and neuroimaging perspective. CNS Spectrums. 2002;7(5):355–62.
23. Krause J. SPECT and PET of the dopamine transporter in attention-deficit/hyperactivity disorder. Expert Rev Neurother. 2008;8(4):611–25. DOI: 10.1586/14737175.8.4.611.
24. Zametkin A, Liebenauer L, Fitzgerald G, et al. Brain metabolism in teenagers with attention deficit hyperactivity disorder. Arch Gen Psychiatry. nineteen93;50:333–40. DOI: http://dx.doi.org/10.1001/archpsyc.1993.01820170011002.
25. Arns M, Conners CK, Kraemer HC. A decade of EEG Theta/Beta ratio research in ADHD – a meta-analysis. J Atten Discord. 2013;17(5):374–83. DOI: 10.1177/1087054712460087. Epub 2012 Oct 19.
26. Anjana Y, Khaliq F, Vaney N. Event-related potentials study in attention deficit hyperactivity disorder. Funct Neurol. 2010;25(2):87–92.
27. Oades RD, Dittman-Balcar A, Schepker R, et al. Auditory event-related potentials (ERPs) and mismatch negativity (MMN) in healthy children and those with attention-deficit or tourettetic symptoms. Biol Psychol. nineteen96;43(2):163–85. DOI: http://dx.doi.org/10.1016/0301-0511(96)05189-7.
Oades RD, Dittman-Balcar A, Schepker R, et al. Auditory event-related potentials (ERPs) and mismatch negativity (MMN) in healthy children and those with attention-deficit or tourettetic symptoms. Biol Psychol. nineteen96;43(2):163–85. DOI: http://dx.doi.org/10.1016/0301-0511(96)05189-7.
28. Meisel V, Servera M, Garcia-Banda G, et al. Neurofeedback and standard pharmacological intervention in ADHD: a randomized controlled trial with six-month follow-up. Biol Psychol. 2013;94(1):12–21. DOI: http://dx.doi.org/10.1016/j.biopsycho.2013.04.015.
29. Wilens T, Spencer T, Biederman J. A large, double-blind, randomized clinical trial of methylphenidate in the treatment of adults with attention-deficit/hyperactivity disorder. Biol Psychiatry. 2005;57(5):456–63. DOI: http://dx.doi.org/10.1016/j.biopsych.2004.11.043. nine0007
30. Lee SS, Humphreys KL, Flory K. Prospective association of childhood attention-deficit/hyperactivity disorder (ADHD) and substance use and abuse/dependence: a meta-analytic review.