Am i schizoaffective test
FREE 3-Minute Schizophrenia Test & Screening: Get Instant Results
Schizophrenia
Do I have schizophrenia? Take this schizophrenia quiz to see if you may benefit from diagnosis and treatment from a mental health professional
Medical ReviewerRandy Bressler, PsyD
Who Is This Schizophrenia Quiz For?
Below is a list of 10 questions designed for people who are concerned about schizophrenia. Read each question carefully, and indicate how often you have experienced the same or similar challenges.
If you have any been struggling for a month or more and those struggles have caused difficulties in functioning for the past six months, let your doctor know. This interactive quiz has been structured in a manner to allow for a short and simple self-assessment. The questions relate to life experiences common among people who have been diagnosed with schizophrenia and are based on criteria in the DSM-5.
How Accurate Is It?
This quiz is NOT a diagnostic tool. Mental health disorders can only be diagnosed by licensed healthcare professionals. Schizophrenia is a chronic brain disorder that is difficult to diagnose. Just over 1% of the US population is estimated to have schizophrenia.
Psycom believes assessments can be a valuable first step toward getting treatment. All too often people stop short of seeking help out of fear their concerns aren't legitimate or severe enough to warrant professional intervention.
Learn More About Schizophrenia
The American Psychiatric Association offers an in-depth guide to the disorder for patients and their families.
The National Alliance on Mental Health (NAMI) has an overview including symptoms, causes and treatment options.
Mental Health America offers some early warning signs of the disorder and contact info for The Schizophrenia & Psychosis Action Alliance (formerly called the National Schizophrenia Foundation) and National Institute of Mental Health, among other resources.
How to Get a Diagnosis
Schizophrenia can only be diagnosed by a medical doctor or mental health professional. A doctor may use tests like MRIs, CT scans or blood tests to check for physical causes for your symptoms. If those can be ruled out, a psychiatric evaluation will be given in which a health care professional will ask about the symptoms you are experiencing, as well as for a family medical history.
The diagnostic criteria for schizophrenia come from the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association.
Your privacy is important to use. All results are completely anonymous.
Professional survey solutions - Alchemer. Please take my survey now
If you think you may have schizophrenia, Psycom strongly recommends that you seek help from a doctor in order to receive a proper diagnosis and support.
Schizophrenia FAQs
How do doctors test for schizophrenia?
There are no laboratory tests to diagnose schizophrenia. Instead, a doctor will perform a physical evaluation, review your medical history, and may use various diagnostic tests, such as a blood test, MRI, or CT scan to rule out any other conditions. If there are no physical reasons for the symptoms, the individual is referred to a psychiatrist or psychologist, for further assessment. A diagnosis is made based on the symptoms the person is experienced and the psychiatrist’s observation of their behavior.
Instead, a doctor will perform a physical evaluation, review your medical history, and may use various diagnostic tests, such as a blood test, MRI, or CT scan to rule out any other conditions. If there are no physical reasons for the symptoms, the individual is referred to a psychiatrist or psychologist, for further assessment. A diagnosis is made based on the symptoms the person is experienced and the psychiatrist’s observation of their behavior.
Is schizophrenia genetic?
Genetics are just one factor in the cause of schizophrenia. Doctors do not believe that one gene is responsible, but that it takes many genetic mutations to raise your chances of having the disorder. While schizophrenia does tend to run in families, it is possible for people with no family history of schizophrenia to be diagnosed with it themselves. Research suggests that a combination of genetic, physical, psychological, and environmental factors make it more likely to be diagnosed with schizophrenia.
What is the major difference between a diagnosis of schizophrenia and schizoaffective disorder?
The main difference between schizophrenia and schizoaffective disorder is the presence of a mood disorder. For people with schizoaffective disorder, the mood disorder is a prominent and persistent part of their condition. People with schizophrenia may experience mood episodes, but the total duration of the mood symptoms is brief and psychotic symptoms are more frequently present.
For people with schizoaffective disorder, the mood disorder is a prominent and persistent part of their condition. People with schizophrenia may experience mood episodes, but the total duration of the mood symptoms is brief and psychotic symptoms are more frequently present.
What type of schizophrenia has the most favorable diagnosis?
The prognosis of schizophrenia is more dependent on the factors relating to the individual themselves, rather than the sub-type of schizophrenia they are diagnosed with. Research suggests multiple factors are associated with a more favorable prognosis: being female, rapid onset of symptoms, older age of first episode, and the presence of predominantly positive symptoms are all examples of such factors.
What co-morbid disorders can often accompany a diagnosis of schizophrenia?
Schizophrenia can co-occur with and be exacerbated by a variety of other mental health disorders including depression, anxiety, obsessive compulsive disorder, substance use disorder, panic disorder, and post-traumatic stress disorder. Some studies have identified depression as the most common comorbidity to occur with Schizophrenia, with up to half of patients with Schizophrenia also experiencing depression.
Some studies have identified depression as the most common comorbidity to occur with Schizophrenia, with up to half of patients with Schizophrenia also experiencing depression.
What are the early signs of schizophrenia?
The most common early signs of schizophrenia may include social withdrawal, depression, hostility, oversleeping or insomnia, inability to cry or express joy, and deterioration of personal hygiene. The early stage of the schizophrenia is called ‘the prodromal phase’. It is difficult to diagnose schizophrenia during this early stage, as these symptoms could result from a number of other problems.
Can someone with schizophrenia live a normal life?
While schizophrenia cannot be cured, with the right treatment plan many people with schizophrenia can live relatively normal lives outside of a healthcare setting. The treatment must be ongoing for the person with schizophrenia to continue to live a productive, fulfilling life, including maintaining a job or socializing with friends and family.
At what age is schizophrenia diagnosed?
Schizophrenia usually develops after puberty, with most people being diagnosed with schizophrenia in their late teens to early 30s. The typical age of onset and diagnosis also varies between males and females. Males are more likely to be diagnosed in their late teens to early 20s, while females are more likely to be diagnosed in their late 20s to early 30s.
Can you see schizophrenia on a brain scan?
Brain scans cannot single-handedly reveal schizophrenia. Brain scans can help doctors to make the right diagnosis for a variety of mental health disorders, but they are not yet intricate enough to reliably diagnose mental health conditions on their own.
- National Institute of Mental Health. Schizophrenia. Accessed July 13, 2021.
- American Psychiatric Association. What is Schizophrenia? Accessed July 13, 2021.
- Buckley, P. F., Miller, B. J., Lehrer, D. S., & Castle, D. J. (2009). Psychiatric comorbidities and schizophrenia.
- Schizophrenia bulletin, 35(2), 383–402. https://doi.org/10.1093/schbul/sbn135. Accessed 4/11/2021.
Notes: This article was originally published June 16, 2021 and most recently updated January 26, 2022.
FREE 3-Minute Schizophrenia Test & Screening: Get Instant Results
Schizophrenia
Do I have schizophrenia? Take this schizophrenia quiz to see if you may benefit from diagnosis and treatment from a mental health professional
Medical ReviewerRandy Bressler, PsyD
Who Is This Schizophrenia Quiz For?
Below is a list of 10 questions designed for people who are concerned about schizophrenia. Read each question carefully, and indicate how often you have experienced the same or similar challenges.
If you have any been struggling for a month or more and those struggles have caused difficulties in functioning for the past six months, let your doctor know. This interactive quiz has been structured in a manner to allow for a short and simple self-assessment. The questions relate to life experiences common among people who have been diagnosed with schizophrenia and are based on criteria in the DSM-5.
This interactive quiz has been structured in a manner to allow for a short and simple self-assessment. The questions relate to life experiences common among people who have been diagnosed with schizophrenia and are based on criteria in the DSM-5.
How Accurate Is It?
This quiz is NOT a diagnostic tool. Mental health disorders can only be diagnosed by licensed healthcare professionals. Schizophrenia is a chronic brain disorder that is difficult to diagnose. Just over 1% of the US population is estimated to have schizophrenia.
Psycom believes assessments can be a valuable first step toward getting treatment. All too often people stop short of seeking help out of fear their concerns aren't legitimate or severe enough to warrant professional intervention.
Learn More About Schizophrenia
The American Psychiatric Association offers an in-depth guide to the disorder for patients and their families.
The National Alliance on Mental Health (NAMI) has an overview including symptoms, causes and treatment options.

Mental Health America offers some early warning signs of the disorder and contact info for The Schizophrenia & Psychosis Action Alliance (formerly called the National Schizophrenia Foundation) and National Institute of Mental Health, among other resources.
How to Get a Diagnosis
Schizophrenia can only be diagnosed by a medical doctor or mental health professional. A doctor may use tests like MRIs, CT scans or blood tests to check for physical causes for your symptoms. If those can be ruled out, a psychiatric evaluation will be given in which a health care professional will ask about the symptoms you are experiencing, as well as for a family medical history.
The diagnostic criteria for schizophrenia come from the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association.
Your privacy is important to use. All results are completely anonymous.
Professional survey solutions - Alchemer. Please take my survey now
Please take my survey now
If you think you may have schizophrenia, Psycom strongly recommends that you seek help from a doctor in order to receive a proper diagnosis and support.
Schizophrenia FAQs
How do doctors test for schizophrenia?
There are no laboratory tests to diagnose schizophrenia. Instead, a doctor will perform a physical evaluation, review your medical history, and may use various diagnostic tests, such as a blood test, MRI, or CT scan to rule out any other conditions. If there are no physical reasons for the symptoms, the individual is referred to a psychiatrist or psychologist, for further assessment. A diagnosis is made based on the symptoms the person is experienced and the psychiatrist’s observation of their behavior.
Is schizophrenia genetic?
Genetics are just one factor in the cause of schizophrenia. Doctors do not believe that one gene is responsible, but that it takes many genetic mutations to raise your chances of having the disorder. While schizophrenia does tend to run in families, it is possible for people with no family history of schizophrenia to be diagnosed with it themselves. Research suggests that a combination of genetic, physical, psychological, and environmental factors make it more likely to be diagnosed with schizophrenia.
While schizophrenia does tend to run in families, it is possible for people with no family history of schizophrenia to be diagnosed with it themselves. Research suggests that a combination of genetic, physical, psychological, and environmental factors make it more likely to be diagnosed with schizophrenia.
What is the major difference between a diagnosis of schizophrenia and schizoaffective disorder?
The main difference between schizophrenia and schizoaffective disorder is the presence of a mood disorder. For people with schizoaffective disorder, the mood disorder is a prominent and persistent part of their condition. People with schizophrenia may experience mood episodes, but the total duration of the mood symptoms is brief and psychotic symptoms are more frequently present.
What type of schizophrenia has the most favorable diagnosis?
The prognosis of schizophrenia is more dependent on the factors relating to the individual themselves, rather than the sub-type of schizophrenia they are diagnosed with. Research suggests multiple factors are associated with a more favorable prognosis: being female, rapid onset of symptoms, older age of first episode, and the presence of predominantly positive symptoms are all examples of such factors.
Research suggests multiple factors are associated with a more favorable prognosis: being female, rapid onset of symptoms, older age of first episode, and the presence of predominantly positive symptoms are all examples of such factors.
What co-morbid disorders can often accompany a diagnosis of schizophrenia?
Schizophrenia can co-occur with and be exacerbated by a variety of other mental health disorders including depression, anxiety, obsessive compulsive disorder, substance use disorder, panic disorder, and post-traumatic stress disorder. Some studies have identified depression as the most common comorbidity to occur with Schizophrenia, with up to half of patients with Schizophrenia also experiencing depression.
What are the early signs of schizophrenia?
The most common early signs of schizophrenia may include social withdrawal, depression, hostility, oversleeping or insomnia, inability to cry or express joy, and deterioration of personal hygiene. The early stage of the schizophrenia is called ‘the prodromal phase’. It is difficult to diagnose schizophrenia during this early stage, as these symptoms could result from a number of other problems.
It is difficult to diagnose schizophrenia during this early stage, as these symptoms could result from a number of other problems.
Can someone with schizophrenia live a normal life?
While schizophrenia cannot be cured, with the right treatment plan many people with schizophrenia can live relatively normal lives outside of a healthcare setting. The treatment must be ongoing for the person with schizophrenia to continue to live a productive, fulfilling life, including maintaining a job or socializing with friends and family.
At what age is schizophrenia diagnosed?
Schizophrenia usually develops after puberty, with most people being diagnosed with schizophrenia in their late teens to early 30s. The typical age of onset and diagnosis also varies between males and females. Males are more likely to be diagnosed in their late teens to early 20s, while females are more likely to be diagnosed in their late 20s to early 30s.
Can you see schizophrenia on a brain scan?
Brain scans cannot single-handedly reveal schizophrenia. Brain scans can help doctors to make the right diagnosis for a variety of mental health disorders, but they are not yet intricate enough to reliably diagnose mental health conditions on their own.
Brain scans can help doctors to make the right diagnosis for a variety of mental health disorders, but they are not yet intricate enough to reliably diagnose mental health conditions on their own.
- National Institute of Mental Health. Schizophrenia. Accessed July 13, 2021.
- American Psychiatric Association. What is Schizophrenia? Accessed July 13, 2021.
- Buckley, P. F., Miller, B. J., Lehrer, D. S., & Castle, D. J. (2009). Psychiatric comorbidities and schizophrenia.
- Schizophrenia bulletin, 35(2), 383–402. https://doi.org/10.1093/schbul/sbn135. Accessed 4/11/2021.
Notes: This article was originally published June 16, 2021 and most recently updated January 26, 2022.
Schizoaffective disorder - symptoms, causes, treatment
Schizoaffective disorder accounts for less than one percent of the disease statistics among the population, but still deserves special attention. It was already at the end of the 20th - beginning of the 21st centuries that this disease was distinguished into a separate type. Most often, schizoaffective disorder begins to manifest itself at the age of 16-30 years, in most cases in women.
Most often, schizoaffective disorder begins to manifest itself at the age of 16-30 years, in most cases in women.
Disease definition - schizoaffective disorder
Schizoaffective disorder is a mental illness characterized by episodic disorders with prominent manic and schizophrenic symptoms. In the International Classification of Diseases of the 10th revision (ICD-10), schizoaffective disorder is coded F25 in the group: schizophrenia, schizotypal states and delusional disorders (F20-F29).
The disease is otherwise called recurrent schizophrenia, intermittent schizophrenia, circular schizophrenia or schizoaffective psychosis. In any case, it is serious and requires the supervision of an experienced specialist. It manifests itself both as regular attacks with different duration (from several days to several years), and episodically, with long periods of remission. As statistics show, a third of patients suffered an attack of schizoaffective disorder only once in their entire lives.
Schizoaffective personality disorder is a disease in which attacks appear periodically, differing in each individual case in duration and symptoms of manifestation.
Symptoms
Symptoms of schizoaffective personality disorder are manifested individually and with their own characteristics. In general, this is the presence in the patient's life of hallucinations, scattered thinking, mood swings, depressive states, obsessions and fantasies.
Since schizoaffective disorder is a borderline condition between schizophrenia, manic disorder and depression, the symptoms are distinguished by three signs.
Signs of schizoaffective disorder:
- Manic - exceeded: vital activity, talkativeness, sexual attention. The patient has accelerated speech, lack of sleep, impulsivity and aggressiveness.
- Depressive - changes in appetite and body weight (often with a big minus), lack of desire to do anything (the patient most often sleeps or wants to rest as soon as possible), haunting feelings of guilt and hopelessness, suicidal thoughts.
- Mixed - hallucinations, delusions, atypical behavior, speech impairment and lethargy, lack of emotion and slowness of movement.
During periods of the peak of the disease, the patient does not see the difference between reality and fantasies, cannot distinguish them on his own.
Causes of disease
The causes of schizoaffective disorder have not been fully identified.
Depending on the individual manifestation and the specific case, general cases of the onset of schizoaffective disorder are distinguished:
- Genetic - a gene for the risk of schizophrenic diseases has been isolated. Every person has this gene, but it either does not appear until certain events, or does not make itself felt until the end of life.
- Prenatal - a pattern was revealed that most often patients born in early spring and late autumn suffer from schizoaffective disorder.
- Social - various stressful events can wake up the "sleeping" gene: life on the verge of begging, conditions of war and constant fear for one's life, loneliness.
 This also includes an asocial lifestyle and all kinds of addictions, especially alcohol and drugs.
This also includes an asocial lifestyle and all kinds of addictions, especially alcohol and drugs.
The pathogenesis of schizoaffective disorder is also not fully understood. The complexity of this disease lies in the fact that it is impossible to isolate specific changes in the body that indicate this disease. Each patient undergoes a thorough examination before such a diagnosis is made.
Not so long ago, scientists tried to find out the biochemical feature of diseases of the F25 group, but they still failed to give a clear answer, what exactly is missing in the body or is in excess.
Only correct observation of the patient gives the psychiatrist accurate grounds for talking about schizoaffective psychosis in the patient.
Stages and classification of the disease
Schizoaffective disorder goes through 2 stages. Each of them is characterized by its own characteristics, which make it possible to understand how to help a patient with a given manifestation of the disease.
Stages of schizoaffective psychosis:
- Stage 1 - the initial period. The patient has vegetosomatic disorders, affective fluctuations, sleep and dream disorders, episodic self-perception disorders. It can last from several weeks to several months.
- Stage 2 - active period. Accompanied by acute psychotic attacks.
Seizures also develop in stages and come in different types. The most frequent - the expanded type (an attack of oneiroid catatonia) - is characterized by stupor and arousal, in which the patient performs incomprehensible actions. Further, this state passes into an illusory-fantastic state.
The development of an attack may stop with the appearance of delirium. Such attacks are called affective-delusional. If the attack is limited to persecutory delusions with depression, then this is a depressive-paranoid attack.
You also need to remember that each case is individual. Patients may have both mixed types of seizures and dual states.
- Stage 3 - residual period. May not leave any residual disturbances and personality changes, however, there is a decrease in activity, concern for one's psychological health.
The classification of schizoaffective disorder is divided into types:
- Manic type (F 25.0) - a disorder in which schizophrenic and manic symptoms are pronounced. The most complex type of disease, has unfavorable prognosis in treatment. Often the behavior of the patient is a danger to him and others.
- Depressive type (F25.1) - a disorder in which both schizophrenic and depressive symptoms are pronounced. Accompanied by symptoms of moderate or severe depression.
- Mixed type (F25.2) - also called cyclic schizophrenia or mixed schizophrenic, and affective psychosis - symptoms of bipolar affective disorder are expressed.
An accurate diagnosis can only be made by an experienced psychiatrist in a specialized clinic.
Complications of the disease
The consequences of schizoaffective disorder can significantly worsen the patient's condition and reduce the quality of life.
- With the onset of remission, patients feel a sense of detachment from the world and life, a sense of shame.
- Serious manic problems such as excessive sexual behavior may appear.
- Drug addiction, drug addiction. Since the drugs are strong enough, the patient may experience euphoria, followed by apathy.
- One of the most serious complications of schizoaffective psychosis is suicidal behavior.
To avoid such complications, the patient's relatives need to contact a specialized clinic for help as soon as possible. It is important to learn how to respond correctly to the behavior of the patient, to know exactly when the attack begins and how to provide first aid.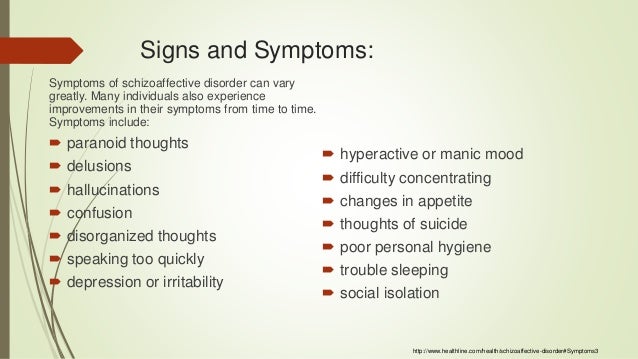
Schizoaffective disorder is not a sentence, it is treated quite successfully, and relatives and friends are one of the important factors helping patients to return to normal faster.
Seeing a psychiatrist is the first step towards recognizing that there is a problem and that it needs to be treated. Unfortunately, in our society, psychiatric clinics and specialists are still perceived as a punitive method, and not a method of help.
The main thing is to understand that schizoaffective disorder has different manifestations and each patient has his own symptoms, and often the opposite: from fantasy illusions to silent inhibition. Therefore, if your loved one began to behave strangely - talking to fictional characters, getting lost in reality, saying things that do not correspond to reality, became aggressive, shows excessive sexual interest, try to convince him or go to the doctors yourself. Particular attention should be paid to such behavior if negative events have occurred in the life of the alleged patient.
The most important thing is not to try to treat yourself and remember that schizoaffective disorder does not go away on its own. The patient needs specialized individual treatment under the supervision of a professional doctor.
Diagnosis
Diagnosis of schizoaffective disorder is carried out by a psychiatrist by monitoring the patient's condition. To make such a diagnosis, the doctor must state that the alleged patient has psychotic symptoms within 2 weeks, as well as the presence of an attack.
Criteria for the diagnosis of schizoaffective disorder:
- There are signs of affective disorders.
- At least 1 of the following is present:
- auditory hallucinations in the form of extraneous voices commenting or leading dialogues;
- delusions of control and influence;
- a feeling of telepathy, that is, the reception or transmission of thoughts at a distance, their openness or withdrawal;
- broken speech and neologisms;
- persistent delusions that are not characteristic of the patient's subculture;
- frequent and transient appearance of catatonic symptoms;
- Symptoms of schizophrenia and affective disorders are presented simultaneously with one exacerbation.
- The patient is not taking drugs or steroids at the time the condition is diagnosed.
- The patient does not have a seizure disorder.
Diagnosis - schizoaffective disorder, can only be a doctor of a specialized clinic.
Treatment
Treatment for schizoaffective disorder depends on the manifestation and symptoms of the illness.
In manic and depressive states, especially during attacks, schizoaffective psychosis requires inpatient treatment with the use of medications - antipsychotic drugs (atypical and traditional), antidepressants (monoamine oxidase inhibitors, tetracyclic and tricyclic), neuroleptics, anxiolytics and mood stabilizers. Electroconvulsive therapy (electric shock) may also be used.
In conjunction with drug treatment, psychotherapy is used, which enhances the effectiveness of drugs.
During the rehabilitation period, work is carried out not only with the patient, but also with relatives and relatives of the patient. Such activities help them interact with each other during remission.
Such activities help them interact with each other during remission.
Clinical guidelines for schizoaffective disorder include recommendations on daily routine, physical activity, mental stress, and taking special medications. Compliance with all prescriptions and constant monitoring by a psychiatrist makes it possible for a stable remission to occur, when the patient can return to normal habitual life and his professional activities.
+7 (495) 121-48-31
References:
- McWilliams N., reflections on schizoid dynamics
- T.A. Solokhina, prof. V.S. Yastrebov, L.S. Shevchenko - A model of organizing socio-psychological care for patients with schizophrenia.
- World Health Organization. International Classification of Diseases (10th Revision): Classification of Mental and Behavioral Disorders: Clinical Description and Diagnostic Guidelines.
- Weiner M., "Practical Psychotherapy"
- Roger McKinnon, Robert Michaels and Peter Buckley "Psychiatric interview in clinical practice" - effective treatment and keeping records and journals
- Kuzmenok G.
 F. Collection “Ways of Understanding. Collection of articles for the 15th anniversary of the Society for Psychoanalytic Psychotherapy” - about the combination of therapy and pharmacology.
F. Collection “Ways of Understanding. Collection of articles for the 15th anniversary of the Society for Psychoanalytic Psychotherapy” - about the combination of therapy and pharmacology. - Tiganov A.S. Guide to Psychiatry - M. Medicine
- Bukhanovsky A.O., Kutyavin Yu.A., Litvak M.E. General psychopathology
- A.V. Snezhnevsky - Clinical psychiatry.
Schizophrenia test online How prone are you to schizophrenia? An exact answer can only be obtained at a psychiatrist's consultation - make an appointment with a doctor to understand your mental state for sure.
If you're not sure it's time to seek medical help, take our quiz.
note
Test results are approximate, indicative. An experienced doctor can both confirm them and refute them. If you are concerned about your mental state, do not put off a visit to a psychotherapist or psychiatrist.
| No. | Question | Yes | Not |
|---|---|---|---|
| one | I always have someone to meet and spend time with | Yes | Not |
| 2 | I believe that life is meaningless | Yes | Not |
| 3 | I don't usually ask for help when I'm doing a job. | Yes | Not |
| four | I often tell my friends: “I just had a wonderful time (spent) this time” | Yes | Not |
| 5 | I have a poor or unsatisfactory sex life | Yes | Not |
| 6 | Some people think I'm weird or crazy | Yes | Not |
| 7 | When others cry or laugh, I remain calm | Yes | Not |
| eight | Wherever I am (at home, on the street or in society), I am always deeply immersed in my thoughts | Yes | Not |
| 9 | I am indifferent to praise | Yes | Not |
| ten | I am never loving, affectionate or tender | Yes | Not |
| eleven | I do not like to work in a team and I am not suitable for such work | Yes | Not |
| 12 | I love life and enjoy it | Yes | Not |
| 13 | I find it difficult to congratulate people on their birthday, holiday or special date | Yes | Not |
| fourteen | If someone scolds me, humiliates me or does not appreciate me enough, I usually ignore it. | Yes | Not |
| fifteen | If someone offends or insults me, I know how to protect myself | Yes | Not |
| 16 | I don't have much success with the opposite sex | Yes | Not |
| 17 | I like spending holidays in the countryside | Yes | Not |
| eighteen | I would rather fail than struggle | Yes | Not |
| 19 | I'm fairly focused on myself | Yes | Not |
| twenty | I'm not interested in friendship and new acquaintances | Yes | Not |
| 21 | It's not easy for me to laugh or smile | Yes | Not |
| 22 | I don't like being part of my family, and I am unrestrained | Yes | Not |
| 23 | Attending the funeral of people I knew does not affect my emotional state | Yes | Not |
| 24 | I feel strong attachment to some people | Yes | Not |
| 25 | I know how my friends live, but they don't know much about me and how I live | Yes | Not |
| 26 | I prefer to do what I can do alone rather than work in a group | Yes | Not |
| 27 | I have few friends - fewer than fingers on one hand (or none at all) | Yes | Not |
| 28 | Sometimes I'm just too lazy to do my daily chores | Yes | Not |
| 29 | Most conversations bore me or seem boring.    Copyright © · The Wright Initiative · Articles · Site Map 
|