Adhd dsm 4
| Disorder Class: Disorders Usually Diagnosed in Infancy, Childhood, and Adolescence | Disorder Class: Neurodevelopmental Disorders |
| A. Either (1) or (2): | A. A persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development, as characterized by (1) and/or (2): |
| 1. Six (or more) of the following symptoms of inattention have persisted for at least 6 months to a degree that is maladaptive and inconsistent with developmental level: | 1. Inattention: Six (or more) of the following symptoms have persisted for at least 6 months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/occupational activities: |
| Note: The symptoms are not solely a manifestation of oppositional behavior, defiance, hostility, or failure to understand tasks or instructions. For older adolescents and adults (age 17 or older), at least five symptoms are required. | |
| Inattention | |
| a. often fails to give close attention to details or makes careless mistakes in schoolwork, work, or other activities | a. Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or during other activities (e.g., overlooks or misses details, work is inaccurate). |
| b. often has difficulty sustaining attention in tasks or play activity | b. Often has difficulty sustaining attention in tasks or play activities (e.g., has difficulty remaining focused during lectures, conversations, or lengthy reading). |
| c. often does not seem to listen when spoken to directly | c. Often does not seem to listen when spoken to directly (e.g., mind seems elsewhere, even in the absence of any obvious distraction). |
| d. often does not follow through on instructions and fails to finish schoolwork, chores or duties in the workplace (not due to oppositional behavior or failure to understand instructions) | d. Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (e.g., starts tasks but quickly loses focus and is easily sidetracked). |
| e. often has difficulty organizing tasks and activities | e. Often has difficulty organizing tasks and activities (e.g., difficulty managing sequential tasks; difficulty keeping materials and belongings in order; messy, disorganized work; has poor time management; fails to meet deadlines). |
| f. often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (such as schoolwork or homework) | f. Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (e. g., schoolwork or homework; for older adolescents and adults, preparing reports, completing forms, reviewing lengthy papers). g., schoolwork or homework; for older adolescents and adults, preparing reports, completing forms, reviewing lengthy papers). |
| g. often loses things necessary for tasks or activities (e.g., toys, school assignments, pencils, books or tools) | g. Often loses things necessary for tasks or activities (e.g., school materials, pencils, books, tools, wallets, keys, paperwork, eyeglasses, mobile telephones). |
| h. is often easily distracted by extraneous stimuli | h. Is often easily distracted by extraneous stimuli (for older adolescents and adults, may include unrelated thoughts). |
i. is often forgetful in daily activities is often forgetful in daily activities | i. Is often forgetful in daily activities (e.g., doing chores, running errands; for older adolescents and adults, returning calls, paying bills, keeping appointments). |
| 2. Six (or more) of the following symptoms of hyperactivity-impulsivity have persisted for at least 6 months to a degree that is maladaptive and inconsistent with developmental level: | 2. Hyperactivity and impulsivity: Six (or more) of the following symptoms have persisted for at least 6 months to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/occupational activities: |
Note: The symptoms are not solely a manifestation of oppositional behavior, defiance, hostility, or a failure to understand tasks or instructions. For older adolescents and adults (age 17 or older), at least five symptoms are required. For older adolescents and adults (age 17 or older), at least five symptoms are required. | |
| Hyperactivity | |
| a. Often fidgets with hands or feet or squirms in seat | a. Often fidgets with or taps hands or feet or squirms in seat. |
| b. Often leaves seat in classroom or in other situations in which remaining seated is expected | b. Often leaves seat in situations when remaining seated is expected (e.g., leaves his or her place in the classroom, in the office or other workplace, or in other situations that require remaining in place). |
| c. Often runs about or climbs excessively in situations in which it is inappropriate (in adolescents or adults, may be limited to subjective feelings of restlessness) | c. Often runs about or climbs in situations where it is inappropriate. (Note: In adolescents or adults, may be limited to feeling restless). |
| d. Often has difficulty playing or engaging in leisure activities quietly | d. Often unable to play or take part in leisure activities quietly. |
| e. Is often “on the go” or often acts as if “driven by a motor” | e. Is often “on the go” acting as if “driven by a motor” (e.g., is unable to be or uncomfortable being still for extended time, as in restaurants, meetings; may be experienced by others as being restless or difficult to keep up with). |
| f. Often talks excessively | f. Often talks excessively. |
| Impulsivity | |
| g. Often blurts out answers before questions have been completed | g. Often blurts out an answer before a question has been completed (e.g., completes people’s sentences; cannot wait for turn in conversation). |
| h. Often has difficulty awaiting turn | h. Often has trouble waiting his/her turn (e.g., while waiting in line). |
| i. Often interrupts or intrudes on others (e.g., butts into conversations or games) | i. Often interrupts or intrudes on others (e.g., butts into conversations, games, or activities; may start using other people’s things without asking or receiving permission; for adolescents and adults, may intrude into or take over what others are doing). |
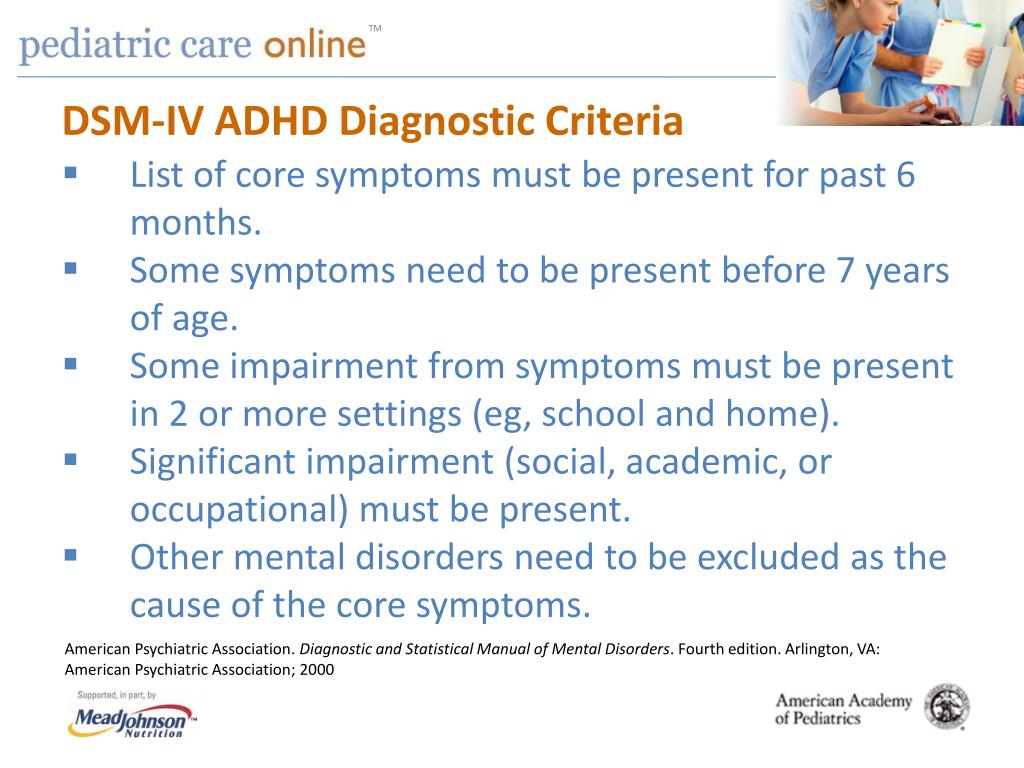
| B. Some hyperactive-impulsive or inattentive symptoms must have been present before age 7 years. | B. Several inattentive or hyperactive-impulsive symptoms were present before age 12 years. |
| C. Some impairment from the symptoms is present in at least two settings (e.g., at school [or work] and at home). | C. Several inattentive or hyperactive-impulsive symptoms are present in two or more settings, (e.g., at home, school or work; with friends or relatives; in other activities). |
| D. There must be clear evidence of clinically significant impairment in social, academic or occupational functioning. | D. There is clear evidence that the symptoms interfere with, or reduce the quality of, social, school, or work functioning. |
E. The symptoms do not occur exclusively during the course of a pervasive developmental disorder, schizophrenia, or other psychotic disorders and is not better accounted for by another mental disorder (e.g., mood disorder, anxiety disorder, dissociative disorder, or a personality disorder). The symptoms do not occur exclusively during the course of a pervasive developmental disorder, schizophrenia, or other psychotic disorders and is not better accounted for by another mental disorder (e.g., mood disorder, anxiety disorder, dissociative disorder, or a personality disorder). | E. The symptoms do not occur exclusively during the course of schizophrenia or another psychotic disorder and are not better explained by another mental disorder (e.g., mood disorder, anxiety disorder, dissociative disorder, personality disorder, substance intoxication or withdrawal). |
Code based on type:
| Specify whether:
|
 01 Attention-Deficit/Hyperactivity Disorder, Predominantly Hyperactive-Impulsive Type: if Criterion A2 is met but Criterion A1 is not met for the past 6 months
01 Attention-Deficit/Hyperactivity Disorder, Predominantly Hyperactive-Impulsive Type: if Criterion A2 is met but Criterion A1 is not met for the past 6 months
Symptoms and Diagnosis of ADHD
COVID-19: Information for parenting children with ADHD
Learn more
Deciding if a child has ADHD is a process with several steps. This page gives you an overview of how ADHD is diagnosed. There is no single test to diagnose ADHD, and many other problems, like sleep disorders, anxiety, depression, and certain types of learning disabilities, can have similar symptoms.
If you are concerned about whether a child might have ADHD, the first step is to talk with a healthcare provider to find out if the symptoms fit the diagnosis. The diagnosis can be made by a mental health professional, like a psychologist or psychiatrist, or by a primary care provider, like a pediatrician.
The American Academy of Pediatrics (AAP) recommends that healthcare providers ask parents, teachers, and other adults who care for the child about the child’s behavior in different settings, like at home, school, or with peers. Read more about the recommendations.
The healthcare provider should also determine whether the child has another condition that can either explain the symptoms better, or that occurs at the same time as ADHD. Read more about other concerns and conditions.
Why Family Health History is Important if Your Child has Attention and Learning Problems
How is ADHD diagnosed?
Healthcare providers use the guidelines in the American Psychiatric Association’s Diagnostic and Statistical Manual, Fifth edition (DSM-5)1, to help diagnose ADHD. This diagnostic standard helps ensure that people are appropriately diagnosed and treated for ADHD. Using the same standard across communities can also help determine how many children have ADHD, and how public health is impacted by this condition.
This diagnostic standard helps ensure that people are appropriately diagnosed and treated for ADHD. Using the same standard across communities can also help determine how many children have ADHD, and how public health is impacted by this condition.
Here are the criteria in shortened form. Please note that they are presented just for your information. Only trained healthcare providers can diagnose or treat ADHD.
Get information and support from the National Resource Center on ADHD
DSM-5 Criteria for ADHD
People with ADHD show a persistent pattern of inattention and/or hyperactivity–impulsivity that interferes with functioning or development:
- Inattention: Six or more symptoms of inattention for children up to age 16 years, or five or more for adolescents age 17 years and older and adults; symptoms of inattention have been present for at least 6 months, and they are inappropriate for developmental level:
- Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or with other activities.
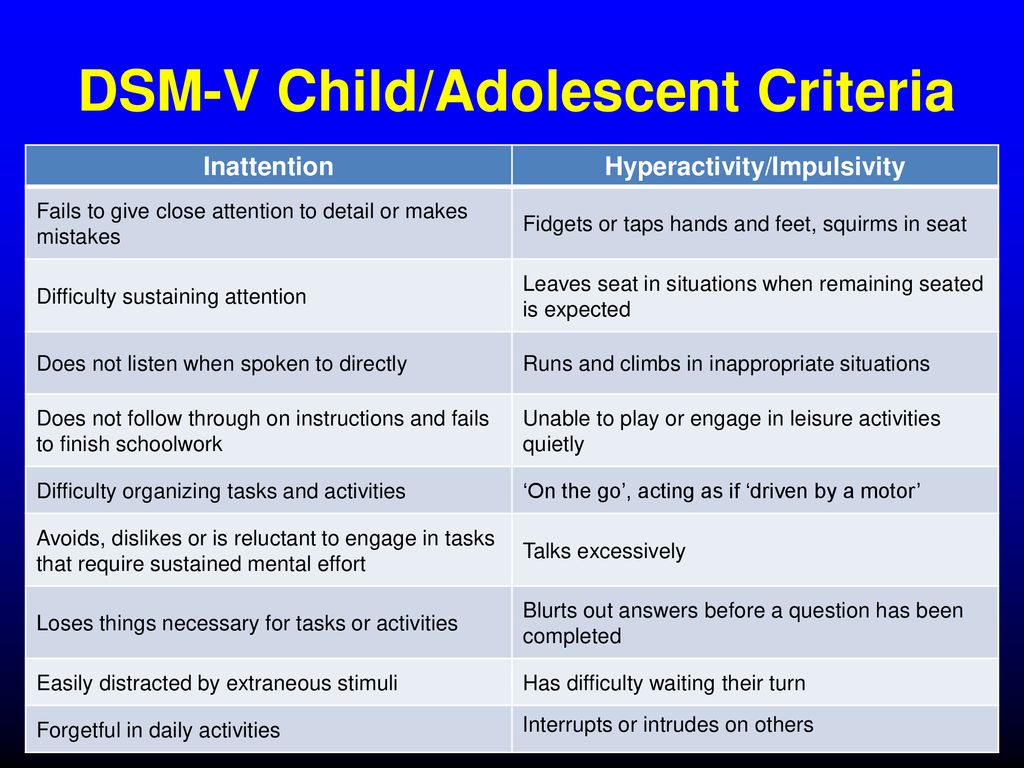
- Often has trouble holding attention on tasks or play activities.
- Often does not seem to listen when spoken to directly.
- Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (e.g., loses focus, side-tracked).
- Often has trouble organizing tasks and activities.
- Often avoids, dislikes, or is reluctant to do tasks that require mental effort over a long period of time (such as schoolwork or homework).
- Often loses things necessary for tasks and activities (e.g. school materials, pencils, books, tools, wallets, keys, paperwork, eyeglasses, mobile telephones).
- Is often easily distracted
- Is often forgetful in daily activities.
- Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or with other activities.
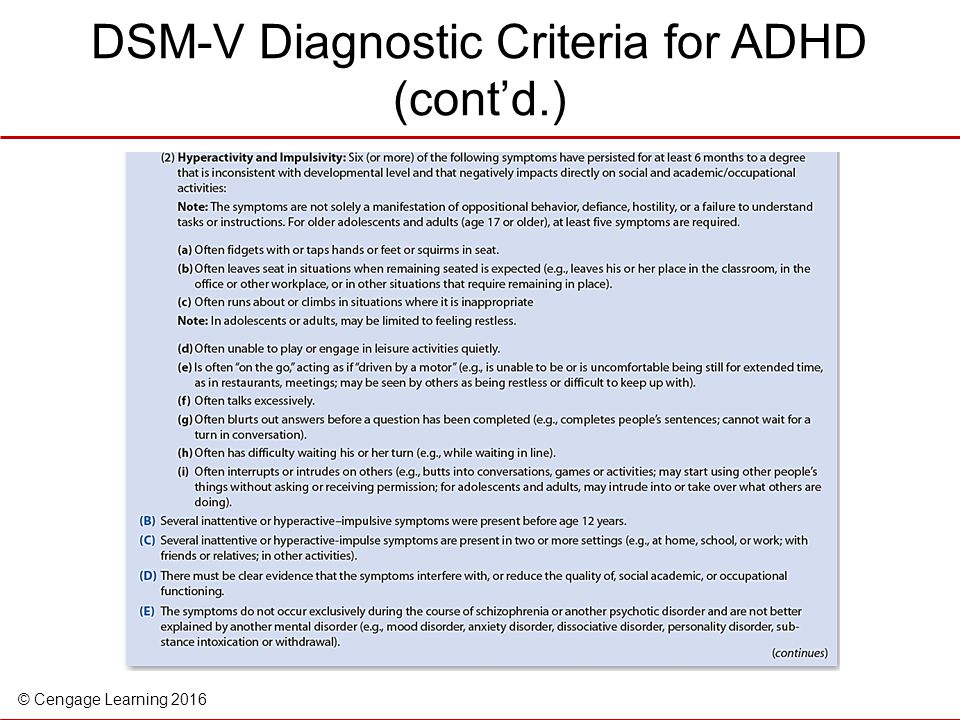
- Hyperactivity and Impulsivity: Six or more symptoms of hyperactivity-impulsivity for children up to age 16 years, or five or more for adolescents age 17 years and older and adults; symptoms of hyperactivity-impulsivity have been present for at least 6 months to an extent that is disruptive and inappropriate for the person’s developmental level:
- Often fidgets with or taps hands or feet, or squirms in seat.
- Often leaves seat in situations when remaining seated is expected.
- Often runs about or climbs in situations where it is not appropriate (adolescents or adults may be limited to feeling restless).
- Often unable to play or take part in leisure activities quietly.
- Is often “on the go” acting as if “driven by a motor”.
- Often talks excessively.
- Often blurts out an answer before a question has been completed.
- Often has trouble waiting their turn.
- Often interrupts or intrudes on others (e.g., butts into conversations or games)
- Often fidgets with or taps hands or feet, or squirms in seat.
In addition, the following conditions must be met:
- Several inattentive or hyperactive-impulsive symptoms were present before age 12 years.
- Several symptoms are present in two or more settings, (such as at home, school or work; with friends or relatives; in other activities).
- There is clear evidence that the symptoms interfere with, or reduce the quality of, social, school, or work functioning.
- The symptoms are not better explained by another mental disorder (such as a mood disorder, anxiety disorder, dissociative disorder, or a personality disorder). The symptoms do not happen only during the course of schizophrenia or another psychotic disorder.
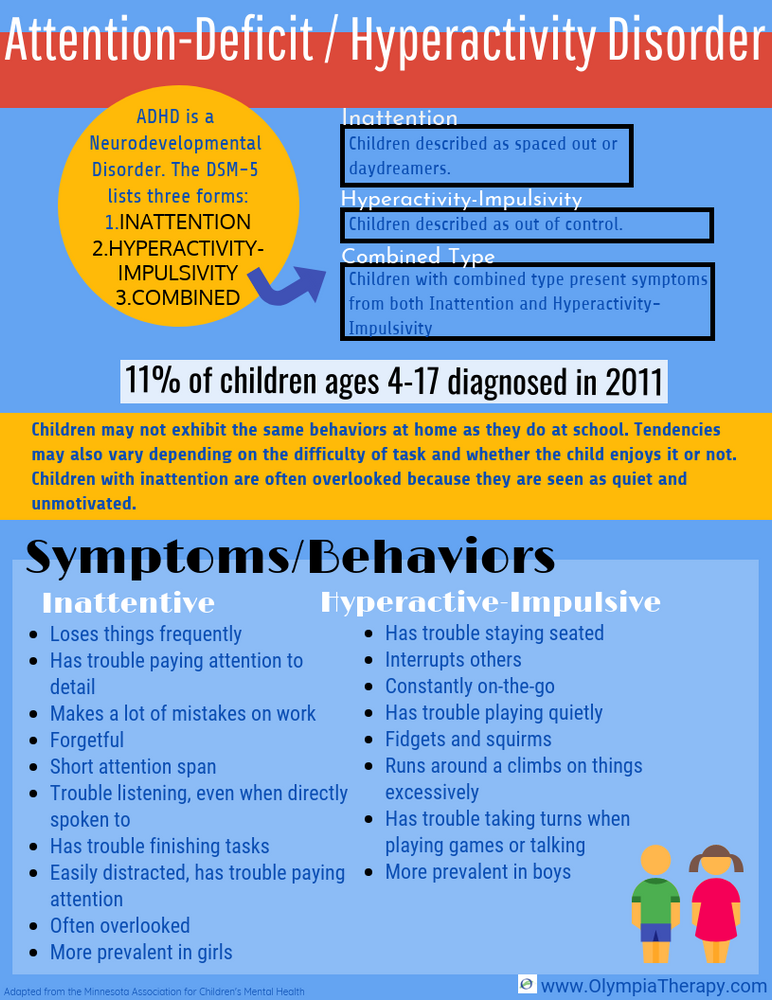
Based on the types of symptoms, three kinds (presentations) of ADHD can occur:
- Combined Presentation: if enough symptoms of both criteria inattention and hyperactivity-impulsivity were present for the past 6 months
- Predominantly Inattentive Presentation: if enough symptoms of inattention, but not hyperactivity-impulsivity, were present for the past six months
- Predominantly Hyperactive-Impulsive Presentation: if enough symptoms of hyperactivity-impulsivity, but not inattention, were present for the past six months.
Because symptoms can change over time, the presentation may change over time as well.
Diagnosing ADHD in Adults
ADHD often lasts into adulthood. To diagnose ADHD in adults and adolescents age 17 years or older, only 5 symptoms are needed instead of the 6 needed for younger children. Symptoms might look different at older ages. For example, in adults, hyperactivity may appear as extreme restlessness or wearing others out with their activity.
To diagnose ADHD in adults and adolescents age 17 years or older, only 5 symptoms are needed instead of the 6 needed for younger children. Symptoms might look different at older ages. For example, in adults, hyperactivity may appear as extreme restlessness or wearing others out with their activity.
For more information about diagnosis and treatment throughout the lifespan, please visit the websites of the National Resource Center on ADHD and the National Institutes of Mental Health.
Reference
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th edition. Arlington, VA., American Psychiatric Association, 2013.
Diagnostic criteria for ADHD according to the DSM-IV classification
Attention-Deficit/Hyperactivity Disorder (ADHD) . [1] [2] [3] . Manifested by symptoms such as difficulty concentrating, hyperactivity and poorly controlled impulsivity. [4]
ADHD and its treatment have been controversial since the 1970s. [5] [6] [7] [8] The existence of ADHD is questioned by a number of health professionals, teachers, politicians, parents and the media. Some believe that ADHD does not exist at all, others believe that there are genetic and physiological causes of this condition. Many people disagree with the use of stimulant drugs for the treatment of ADHD. [6]
[5] [6] [7] [8] The existence of ADHD is questioned by a number of health professionals, teachers, politicians, parents and the media. Some believe that ADHD does not exist at all, others believe that there are genetic and physiological causes of this condition. Many people disagree with the use of stimulant drugs for the treatment of ADHD. [6]
|
Contents
|
 1 Russian
1 Russian General information
From a neurological point of view, ADHD is regarded as a persistent and chronic syndrome for which no cure has been found. According to the population of the United States, this disorder is present in 3-5% of people, including both children and adults. [9]
According to the current (early 2007) diagnostic criteria, ADHD can be diagnosed starting in late preschool or school age, as assessment of the child's behavior in at least two settings (e.g., home and school) is required to fulfill the diagnosis requirements. The presence of learning disabilities and social functioning is a necessary criterion for establishing a diagnosis of ADHD. nine0009 [10] The question of the objectivity of the diagnosis of ADHD and sufficient grounds for prescribing drug treatment remains debatable, due to the lack of uniform diagnostic criteria and methods for assessing the symptoms of the disease.
Prevalence
ADHD is more common in boys. The relative prevalence among boys and girls ranges from 3:1 to 9:1, depending on the criteria for diagnosis, study methods, and study groups (children who were referred to a doctor; schoolchildren; the general population). The estimates of the prevalence of ADHD also depend on these factors (from 1-2% to 25-30%). According to some data, the prevalence of the syndrome among younger schoolchildren is about 10-15%, in boys it occurred 2.8-3 times more often than in girls. nine0017
Definition and criteria for diagnosis
Currently, the basis for establishing a diagnosis is a phenomenological psychological characteristic. Many of the signs of ADHD appear only occasionally.
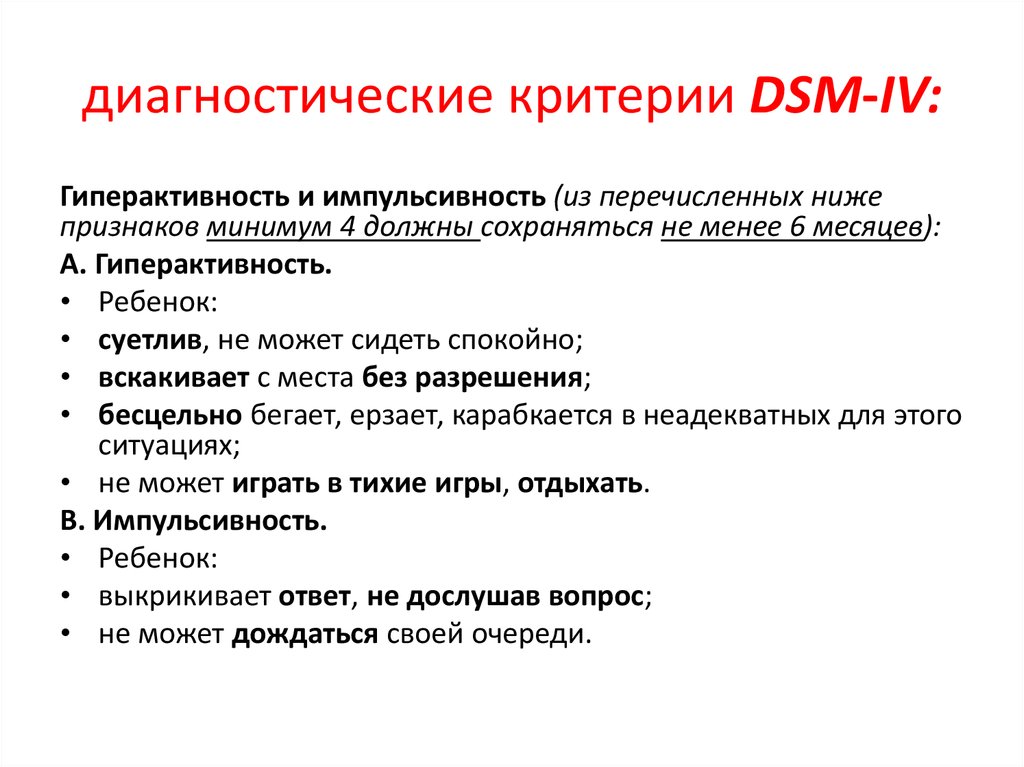
Impulsivity
One of the main signs of ADHD, along with attention disorders, is impulsivity - lack of control of behavior in response to specific demands. Clinically, these children are often characterized as reacting quickly to situations, not waiting for directions and instructions to complete the task, and inadequately assessing the requirements of the task. As a result, they are very careless, inattentive, careless and frivolous. These children often fail to consider the potentially negative, harmful, or destructive (and even dangerous) consequences that may be associated with certain situations or their actions. Often they expose themselves to unreasonable, unnecessary risks in order to show their courage, whims and quirks, especially in front of their peers. As a result, accidents with poisoning and injuries are not uncommon. Children with ADHD may carelessly damage or destroy someone's property much more often than children without signs of ADHD. nine0017
As a result, they are very careless, inattentive, careless and frivolous. These children often fail to consider the potentially negative, harmful, or destructive (and even dangerous) consequences that may be associated with certain situations or their actions. Often they expose themselves to unreasonable, unnecessary risks in order to show their courage, whims and quirks, especially in front of their peers. As a result, accidents with poisoning and injuries are not uncommon. Children with ADHD may carelessly damage or destroy someone's property much more often than children without signs of ADHD. nine0017
One of the difficulties in diagnosing ADHD is that it is often accompanied by other problems. A small group of people with ADHD suffer from a rare disorder called Tourette's syndrome.
DSM-IV Diagnostic Criteria for ADHD
I. Choice of option A or B:
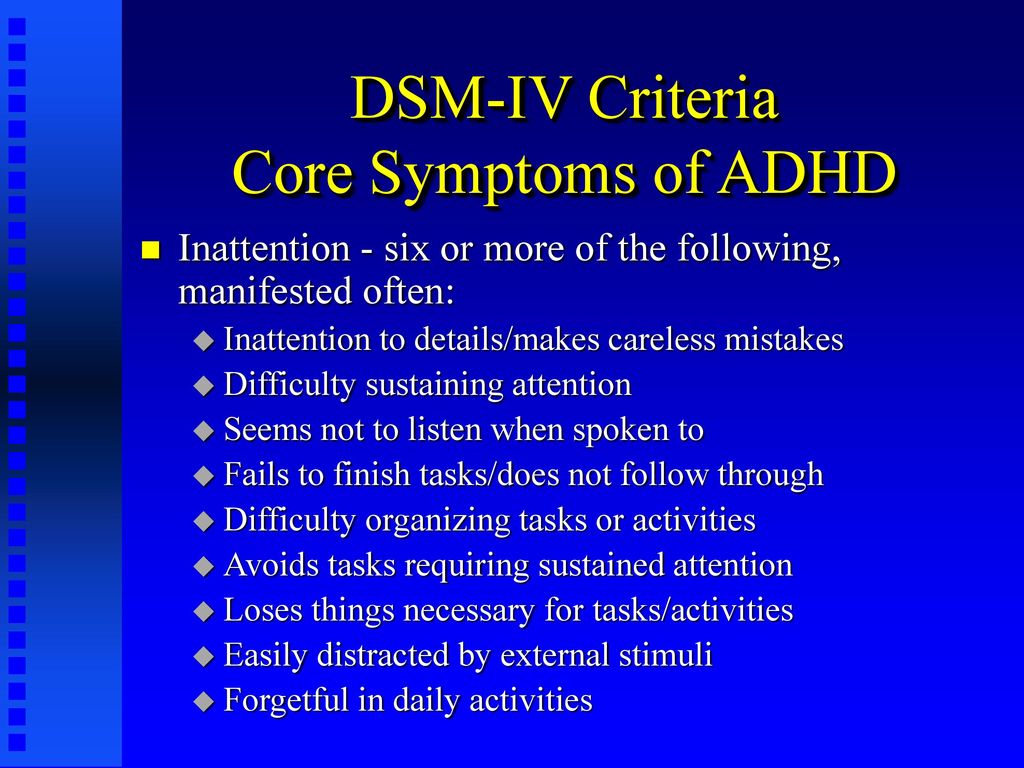
A. INATTENTION Diagnosis requires six or more of the following symptoms of inattention that persist for at least six months and are severe enough to indicate a lack of adjustment and inconsistency with normal age characteristics:
- Often unable to pay attention to details; due to negligence, frivolity, makes mistakes in school assignments, in work performed and other activities.
- Usually has difficulty maintaining attention when performing tasks or playing games.
- It often seems that the child does not listen to the speech addressed to him.
- Often fails to follow the instructions given and to complete the lessons, homework or duties at the workplace (which has nothing to do with negative or protest behavior, inability to understand the task). nine0039
- Often has difficulty organizing tasks and other activities independently.
- Usually avoids involvement in tasks that require sustained mental effort (eg, schoolwork, homework).
- Frequently loses things needed at school and at home (eg toys, school supplies, pencils, books, work tools).
- Easily distracted by extraneous stimuli. nine0038 Often shows forgetfulness in everyday situations.
B. HYPERACTIVITY . The presence of six or more of the following symptoms of hyperactivity and impulsivity that persist for at least six months and are so pronounced that they indicate a lack of adaptation and inconsistency with normal age characteristics:
- Restless movements in the hands and feet are often observed; sitting on a chair, spinning, spinning.
 nine0039
nine0039 - Often gets up from his seat in class during lessons or other situations where he needs to stay put.
- Often shows aimless motor activity: runs, spins, tries to climb somewhere, and in such situations when it is unacceptable.
- Usually unable to play quietly, calmly, or engage in leisure activities.
- Is often in constant motion and behaves "as if a motor were attached to it".
- Often talkative. nine0039
IMPULSITY
- Often answers questions without thinking, without listening to the end.
- Usually has difficulty waiting for his turn in various situations.
- Often interferes with others, sticks to others (for example, interferes in conversations or games).
II. ( B. ) Some of the symptoms of impulsivity, hyperactivity, and inattention begin to disturb others before the age of seven. nine0017
III. ( C. ) Problems associated with the above symptoms occur in two or more settings (eg, school and home).
IV. ( D. ) There is strong evidence of clinically significant impairments in social contacts or schooling.
Adult ADHD
It turns out that more than half of the children suffering from this disorder continue to suffer from it into adulthood. In 30-70% of cases, ADHD symptoms continue into adulthood. Many adults who did not have this problem in childhood do not realize that this is precisely the reason for their inability to maintain attention, difficulties in learning new material, in organizing the space around them and in interpersonal relationships. nine0017
Treatments for ADHD
Approaches to the treatment and management of ADHD and the methods available may differ from country to country. However, despite these differences, most experts consider the most effective integrated approach, which combines several methods, individually selected in each case. Methods of behavior modification, psychotherapy, pedagogical and neuropsychological correction are used. "Drug therapy is indicated on an individual basis when the cognitive and behavioral problems in a child with ADHD cannot be managed by non-drug methods alone." nine0009 [11] In the USA, addictive [12] [13] [14] Ritalin is used for treatment.
"Drug therapy is indicated on an individual basis when the cognitive and behavioral problems in a child with ADHD cannot be managed by non-drug methods alone." nine0009 [11] In the USA, addictive [12] [13] [14] Ritalin is used for treatment.
Currently, there are several approaches to the treatment of ADHD
- Neuropsychological . When, with the help of various exercises, we return to the previous stages of ontogenesis and rebuild those functions that were formed archaically incorrectly and have already been fixed. To do this, they need, like any other ineffective pathological skill, to purposefully reveal, disinhibit, destroy and create a new skill that is more consistent with effective work. And this is carried out on all three floors of mental activity. This is a laborious, multi-month job. The child is born 9months. And neuropsychological correction is designed for this period. And then the brain begins to work more efficiently, with less energy costs.
 Old archaic connections, relations between the hemispheres are normalizing. Energy, management, active attention are built.
Old archaic connections, relations between the hemispheres are normalizing. Energy, management, active attention are built.
- Syndromic . Let's imagine that a personally mature child wants to behave in accordance with the norms, wants to learn, to perceive knowledge. His parents raised him well. He must sit quietly in class. Must be attentive and listen, control yourself. Three difficult tasks at the same time. Not a single adult person is able to perform three tasks that are difficult for him. Therefore, syndromic work is that the child is given an interesting activity (voluntary). But in this activity there is post-voluntary attention (when we become interested in something and delved into it, we already strain without additional costs). Therefore, when they say that children with ADHD are able to sit at the computer for a very long time, then this is a completely different attention. nine0039
There are outdoor games that require only the effort of attention.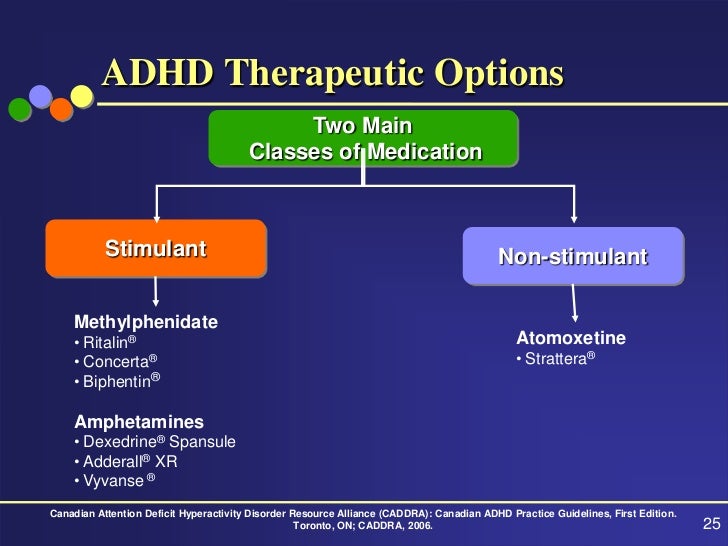 The child moves according to the conditions of the game, he can be explosive, impulsive. This may help him win. But the game is about attention. This function is being trained. Then the restraint function is trained. However, he can be distracted. Each task is solved as it arrives. This improves each feature individually.
The child moves according to the conditions of the game, he can be explosive, impulsive. This may help him win. But the game is about attention. This function is being trained. Then the restraint function is trained. However, he can be distracted. Each task is solved as it arrives. This improves each feature individually.
But no medicine teaches how to behave, so two more directions are added:
- Behavioral or Behavioral Therapy focuses on certain behavioral patterns, either shaping or extinguishing them through reward, punishment, coercion and inspiration.
- Work on personality. Family therapy , which forms the personality and which determines where to direct these qualities (disinhibition, aggressiveness, increased activity).
All this complex of methods of psychocorrection and drug treatment with timely diagnosis will help hyperactive children to compensate for violations in time and fully realize themselves in life.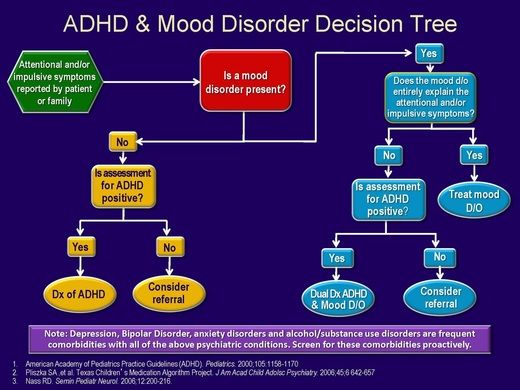 nine0017
nine0017
Pharmacocorrection
Drugs are used as an adjunct in the treatment of ADHD. The best known of these are psychostimulants such as methylphenidate, dextroamphetamine with amphetamine, and dextroamphetamine. One of the disadvantages of these drugs is the need to take them several times a day (the duration of action is about 4 hours). Now there are methylphenidate and dextroamphetamine with long-acting amphetamine (up to 12 hours). Other groups of drugs are also used, for example, atomoxetine. nine0017
Drug therapy is given on an individual basis when the cognitive and behavioral problems in a child with ADHD cannot be managed by non-drug interventions alone.
The United Nations Committee on the Rights of the Child has issued recommendations stating: “The Committee is concerned about reports that Attention Deficit Hyperactivity Disorder (ADHD) and Attention Deficit Disorder (ADD) are being misdiagnosed and that psychostimulants are being over-prescribed as a result despite increasing evidence of the harmful effects of these drugs. The Committee recommends further research into the diagnosis and treatment of ADHD and ADD, including the possible negative effects of psychostimulants on the physical and psychological well-being of children, and the maximum use of other forms of management and treatment when addressing behavioral disorders.” nine0009 [15]
The Committee recommends further research into the diagnosis and treatment of ADHD and ADD, including the possible negative effects of psychostimulants on the physical and psychological well-being of children, and the maximum use of other forms of management and treatment when addressing behavioral disorders.” nine0009 [15]
The approach common in the CIS is nootropic drugs, substances that improve brain function, metabolism, energy, increase the tone of the cortex. Also prescribed drugs, consisting of amino acids, which improve the metabolism of the brain. There is no evidence that such treatment is effective.
- Psychostimulants
- Pemoline
- Methylphenidate
- Dextroamphetamine
- Antidepressants nine0037
- Venlafaxine
- Nortriptyline
- Atomoxetine
Causes of ADHD
The exact cause of ADHD is not known [16] , but there are several theories. The causes of organic disorders can be:
The causes of organic disorders can be:
- General deterioration of the environmental situation.
- Infections of the mother during pregnancy and the effects of drugs, alcohol, drugs, smoking during this period.
- Immunological incompatibility (by Rh factor). nine0039
- Threats of miscarriage.
- Chronic diseases of the mother.
- Premature, transient or prolonged labor, induction of labor, anesthesia poisoning, caesarean section.
- Birth complications (improper presentation of the fetus, entanglement of the umbilical cord) lead to injuries of the fetal spine, asphyxia, internal cerebral hemorrhage.
- Any illness in infants with high fever and strong medications.
- Asthma, pneumonia, heart failure, diabetes, kidney disease can all interfere with normal brain function [17] .
Genetic factors
Specialists of the Medical Genetic Research Center of the Russian Academy of Medical Sciences and the Faculty of Psychology of Moscow State University found that “most researchers agree that a single cause of the disease cannot be identified and, it seems, will never be possible” [18] . Scientists from the United States, Holland, Colombia and Germany have suggested that 80% of the occurrence of ADHD depends on genetic factors. Out of more than thirty candidate genes, three were selected - the dopamine transporter gene, as well as two dopamine receptor genes. However, the genetic prerequisites for the development of ADHD are manifested in interaction with the environment, which can strengthen or weaken these prerequisites [18] .
Scientists from the United States, Holland, Colombia and Germany have suggested that 80% of the occurrence of ADHD depends on genetic factors. Out of more than thirty candidate genes, three were selected - the dopamine transporter gene, as well as two dopamine receptor genes. However, the genetic prerequisites for the development of ADHD are manifested in interaction with the environment, which can strengthen or weaken these prerequisites [18] .
Other common comorbidities
- Asperger's Syndrome
- Bipolar affective disorder
- Dyslexia
- Tourette syndrome
Forecast
Individuals with this disease have to put up with a number of restrictions.
Criticism
ADHD is one of the most questionable and controversial mental disorders [19] [20] ADHD and its treatment have been questioned since at least 1970s. [6] [21] [22] Many doctors, teachers, high-ranking politicians, parents and the media doubt the existence of ADHD. The range of opinions about ADHD is quite wide - from those who do not believe that ADHD exists, to those who believe that there are genetic or physiological prerequisites for this condition. [6]
The range of opinions about ADHD is quite wide - from those who do not believe that ADHD exists, to those who believe that there are genetic or physiological prerequisites for this condition. [6]
Researchers at Canada's McMaster University have identified five main points on which the debate is evolving:
- Clinical diagnosis for which there are no laboratory or radiological diagnostic tests or physical features of the body.
- Criteria for diagnosis changed frequently.
- There is no effective treatment. Existing methods of treatment are very long.
- In the treatment, drugs are used, some of which contain narcotic substances (methylphenidate, dextroamphetamine). nine0038 The number of diagnoses varies considerably across countries. [23]
In 1998, the National Institutes of Health hosted a conference on ADHD. By the end of the conference, they came to the following conclusion:
".
..We do not have an independent, reliable test for ADHD and there is no evidence that ADHD is caused by a brain disorder."
Original text
"...We do not have an independent, valid test for ADD/ADHD and there are no data to indicate that ADD/ADHD is due to a brain malfunction." [24]
Lack of clarity about what could be classified as ADHD and changes in criteria for diagnosis led to confusion. [25] Ethical and legal issues regarding treatment have been major areas of controversy, especially the use of psychostimulants in treatment, and the advertising of stimulants for the treatment of ADHD by groups and individuals who receive money from pharmaceutical companies. nine0009 [20]
Medical professionals and news agencies have argued that the diagnosis and treatment of this disorder deserves more thorough investigation. [26]
Alternative theories [27] such as Hunter vs. farmer theory, Neurodiversity and Social construct theory of ADHD have been proposed to explain the symptoms of ADHD.
farmer theory, Neurodiversity and Social construct theory of ADHD have been proposed to explain the symptoms of ADHD.
Some individuals and groups completely deny the existence of ADHD. These include Thomas Szasz, Michel Foucault, and groups such as the Citizens' Commission on Human Rights (CCHR). nine0009 [28] However, most US medical authorities and courts consider ADHD diagnoses to be legitimate. (See Ritalin class action lawsuits)
Literature
In Russian
- Altherr P., Berg L., Wölfl A., Passolt M. Hyperactive children. Correction of psychomotor development. - M: Publishing Center "Academy", 2004
- Bryazgunov I.P., Kasatikova E.V. Restless child or all about hyperactive children. - M.: Publishing House of the Institute of Psychotherapy, 2002
- Bryazgunov I.P., Kasatikova E.V. Attention deficit hyperactivity disorder in children. - M.: Medpraktika-M, 2002
- Zavadenko N.N. Hyperactivity and attention deficit in childhood.
 - M.: Publishing center "Academy", 2005.
- M.: Publishing center "Academy", 2005. - Zavadenko N.N. How to understand a child: children with hyperactivity and attention deficit. - School-Press, 2001
- Zavadenko N.N., Suvorinova N.Yu., Rumyantseva M.V. Attention deficit hyperactivity disorder: risk factors, age dynamics, diagnostic features. - Defectology, 2003, No. 6
- Monina G.B., Lyutova-Roberts E.K., Chutko L.S. hyperactive children. Psychological and pedagogical correction. - St. Petersburg: Speech, 2007
- Murashova E.V. Children are “mattresses” and children are “catastrophes”. Hypodynamic and hyperdynamic syndrome" - Yekaterinburg: U-Factoria, 2004.
- Russell A. Barclay, Christina M. Benton. Your naughty child. - St. Petersburg: Peter, 2004
- Chutko L.S., Pal'chik A.B., Kropotov Yu.D. Attention deficit hyperactivity disorder in children and adolescents. - St. Petersburg: SPbMAPO Publishing House, 2004
- Chutko L.S. Attention deficit hyperactivity disorder and concomitant disorders.
 - St. Petersburg: Hoka, 2007
- St. Petersburg: Hoka, 2007
In foreign languages
- Hartmann, Thom "Attention Deficit Disorder, A Different Perception" subtitled "A Hunter in a Farmers World".
- Barkley, Russell A. Take Charge of ADHD: The Complete Authoritative Guide for Parents (2005) New York: Guilford Publications.
- Bellak L, Kay SR, Opler LA. (1987) "Attention deficit disorder psychosis as a diagnostic category". nine0005 Psychiatric Developments , 5(3), 239-63. PMID 3454965
- Conrad, Peter Identifying Hyperactive Children (Ashgate, 2006).
- Crawford, Teresa I'm Not Stupid! I'm ADHD!
- Green, Christopher, Kit Chee, Understanding ADD ; Doubleday 1994; ISBN 0-86824-587-9
- Hanna, Mohab. (2006) Making the Connection: A Parent's Guide to Medication in AD/HD , Washington D.C.: Ladner-Drysdale.
- Joseph, J. (2000). "Not in Their Genes: A Critical View of the Genetics of Attention-Deficit Hyperactivity Disorder", Developmental Review 20, 539-567.
- Kelly, Kate, Peggy Ramundo. (1993) You Mean I'm Not Lazy, Stupid or Crazy?! A Self-Help Book for Adults with Attention deficit Disorder . ISBN 0-684-81531-1
- Matlen, Terry. (2005) "Survival Tips for Women with AD/HD". ISBN 1886941599
- Ninivaggi, F.J. "Attention-Deficit/Hyperactivity Disorder in Children and Adolescents: Rethinking Diagnosis and Treatment Implications for Complicated Cases", Connecticut Medicine . September 1999; Vol. 63, no. 9, 515-521. PMID 10531701
Notes
- ↑ LONI: Laboratory of Neuro Imaging
- ↑ NINDS Attention Deficit-Hyperactivity Disorder Information Page. National Institute of Neurological Disorders and Stroke (NINDS/NIH) February 9, 2007. Accessed 2007-08-13.
- ↑ Russell A. Barkley Official Site, Authority ADHD, Attention Deficit Hyperactivity Disorder
- ↑ Attention-Deficit/Hyperactivity Disorder (ADHD). Data from Behavenet.
 com . Information collected on December 11, 2006.
com . Information collected on December 11, 2006. - ↑ Vincent Parrillo Encyclopedia of Social Problems. - SAGE, 2008. - P. 63. - ISBN 9781412941655
- ↑ 1 2 3 4 Treatment of Attention-Deficit/Hyperactivity Disorder. US department of health and human services (December 1999). Retrieved October 2, 2008.
- ↑ Mayes R, Bagwell C, Erkulwater J (2008). "ADHD and the rise in stimulant use among children". Harv Rev Psychiatry 16 (3): 151–66. DOI:10.1080/10673220802167782. PMID 18569037.
- ↑ Developmental psychopathology. - Chichester: John Wiley & Sons, 2006. - ISBN 0-471-23737-X
- ↑ ADD/ADHD Health Center. Information from WebMD.com . Data collected December 11, 2006.
- ↑ Attention deficit/hyperactivity disorder.
 E.D. Belousova, M.Yu. Nikanorov. Department of Psychoneurology and Epileptology, Moscow Research Institute of Pediatrics and Pediatric Surgery, Ministry of Health of the Russian Federation
E.D. Belousova, M.Yu. Nikanorov. Department of Psychoneurology and Epileptology, Moscow Research Institute of Pediatrics and Pediatric Surgery, Ministry of Health of the Russian Federation - ↑ Attention deficit hyperactivity disorder in children: modern approaches to pharmacotherapy N.N. Zavadenko, N.Yu. Suvorinova, N.V. Grigoriev. Department of Nervous Diseases, Faculty of Pediatrics, Russian State Medical University, Moscow
- ↑ RIA Novosti
- ↑ Belgian tragedy: is the "American Syndrome" to blame?
- ↑ Ritalin addiction help
- ↑ http://www.cchr.ru/press1.html Child psychiatrists in Australia, Finland and Denmark received
- ↑ Stimulant medication for the treatment of attention-deficit hyperactivity disorder: evidence-b(i)ased practice? -- Bailly 29 (8): 284 -- Psychiatric Bulletin. nine0038 ↑ Article about ADHD on the website of the Faculty of Psychological and Pedagogical Management of the Higher School of Social and Management Consulting
- ↑ 1 2 Genetics of Hyperactivity and Attention Deficit//Chemistry and Life.
 2008. No. 1., p. 5
2008. No. 1., p. 5 - ↑ Mayes R, Bagwell C, Erkulwater J (2008). "ADHD and the rise in stimulant use among children". Harv Rev Psychiatry 16 (3): 151–66. DOI:10.1080/10673220802167782. PMID 18569037. Foreman, D. M. (2006). "Attention deficit hyperactivity disorder: legal and ethical aspects" (REVIEW, full text). Archives of Disease in Childhood 91 (2): 192-94. DOI:10.1136/adc.2004.064576. PMID 16428370.
- ↑ Vincent Parrillo Encyclopedia of Social Problems. - SAGE, 2008. - ISBN 9781412941655
- ↑ Developmental psychopathology. - Chichester: John Wiley & Sons, 2006. - ISBN 0-471-23737-X
- ↑ Jadad AR, Booker L, Gauld M, et al (December 1999). "The treatment of attention-deficit hyperactivity disorder: an annotated bibliography and critical appraisal of published systematic reviews and metaanalyses".
 Canadian journal of psychiatry. Revue canadienne de psychiatrie 44 (10): 1025–35. PMID 10637682.
Canadian journal of psychiatry. Revue canadienne de psychiatrie 44 (10): 1025–35. PMID 10637682. - ↑ www.adhdtesting.org A real look inside the issue
- ↑ PBS - frontline: medicating kids: adhd: american academy of pediatrics' guidelines.
- ↑ BBC NEWS.
- ↑ Rethinking ADHD >> Palgrave.com: Title Page.
- ↑ Citizens Commission On Human Rights - Australia (CCHR Australia).
External links
In Russian
- Attention deficit hyperactivity disorder. (ADHD)
- Attention deficit hyperactivity disorder in children: modern approaches to pharmacotherapy
- Attention Fund
- Attention Deficit Hyperactivity Disorder in Children (ADHD)
- Articles on ADHD
- About Attention Deficit Hyperactivity Disorder (ADHD-ADHD)
- Physician reports on ADHD
- Psychiatry Chapter 18 Attention Disorder with Hyperactivity Disorder P.
 Wander, R. Scheider
Wander, R. Scheider - Attention deficit hyperactivity disorder in children: modern approaches to pharmacotherapy
Critical
- Citizens Commission on Human Rights. ADHD and "learning disorder"
- Dangerous psychiatric diagnosis
- Pseudoscience
- Invented "diseases" are the product of fraud
- Fred Baughman, excerpt from The ADHD Fraud: How Psychiatry Makes Patients Out of Normal Children
- "Mirror of the Week", No. 36 (360) September 15 - 21, 2001, "TABLET" PEDAGOGY
- Blog "Psychology versus psychiatry - the fight of the century!"
- The Truth about ADHD from their mouth! (video)
- Psychiatrist Thomas Szas about psychiatry [1] (video)
English
- Live with Dr. Fred Baughman: ADHD fraud and the chemical holocaust against a generation of children. — Taichung: Truth Publishing International, Ltd., 2005.
- adhd
- Attention-Deficit / Hyperactivity Disorder (ADHD) at the Center for Disease Control
- Diagnosis and Treatment of Attention Deficit Hyperactivity Disorder at NIH
- National Institute of Mental Health on ADHD
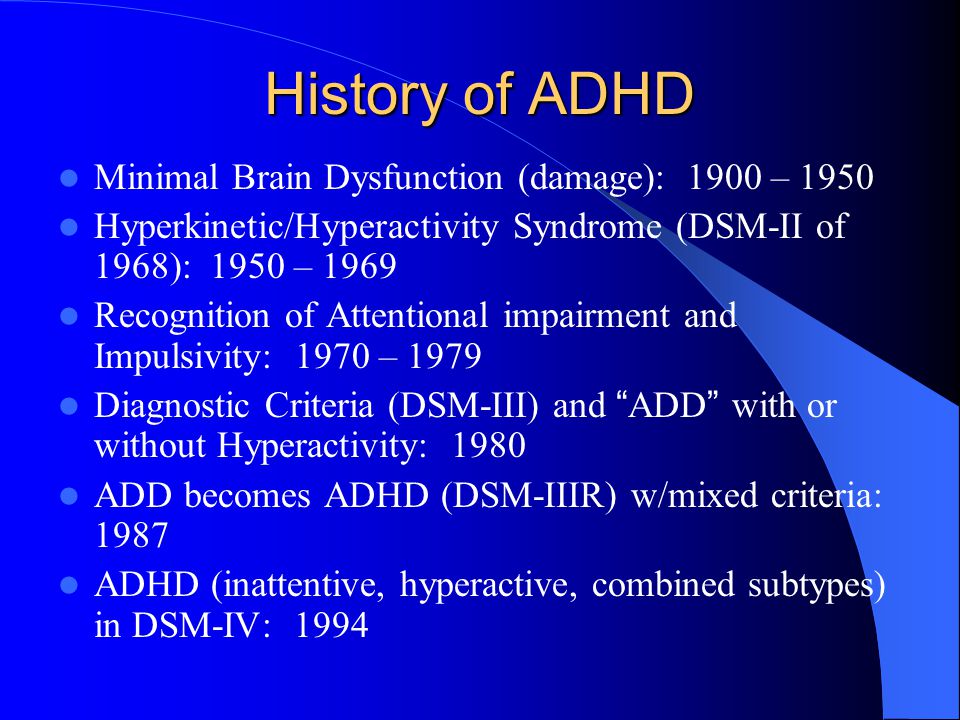
- The History of ADHD: 1798, Alexander Crichton, with pictures of the original works and sources.
 ADHD Uppmärksammas Koncentrerat Digest
ADHD Uppmärksammas Koncentrerat Digest - The History of ADHD: 1902 with some original pictures of Sir George Frederick Still and his work. ADHD Uppmärksammas Koncentrerat Digest
- About.com: ADD/ADHD
See also
- Sluggish schizophrenia
- Drapetomania
- Psychiatric abuse
DSM-IV Diagnostic Criteria for ADHD
Attention-Deficit/Hyperactivity Disorder (ADHD) age. nine0009 [1] [2] [3] . Manifested by symptoms such as difficulty concentrating, hyperactivity and poorly controlled impulsivity. [4]
ADHD and its treatment have been controversial since the 1970s. [5] [6] [7] [8] The existence of ADHD is questioned by a number of health professionals, teachers, politicians, parents and the media. Some believe that ADHD does not exist at all, others believe that there are genetic and physiological causes of this condition. Many people disagree with the use of stimulant drugs for the treatment of ADHD. nine0009 [6]
Many people disagree with the use of stimulant drugs for the treatment of ADHD. nine0009 [6]
|
Contents
|
General information
From a neurological point of view, ADHD is regarded as a persistent and chronic syndrome for which no cure has been found. According to the population of the United States, this disorder is present in 3-5% of people, including both children and adults. [9]
According to the population of the United States, this disorder is present in 3-5% of people, including both children and adults. [9]
According to the current (early 2007) diagnostic criteria, ADHD can be diagnosed starting in late preschool or school age, as assessment of the child's behavior in at least two settings (e.g., home and school) is required to fulfill the diagnosis requirements. The presence of learning disabilities and social functioning is a necessary criterion for establishing a diagnosis of ADHD. nine0009 [10] The question of the objectivity of the diagnosis of ADHD and sufficient grounds for prescribing drug treatment remains debatable, due to the lack of uniform diagnostic criteria and methods for assessing the symptoms of the disease.
Prevalence
ADHD is more common in boys. The relative prevalence among boys and girls ranges from 3:1 to 9:1, depending on the criteria for diagnosis, study methods, and study groups (children who were referred to a doctor; schoolchildren; the general population). The estimates of the prevalence of ADHD also depend on these factors (from 1-2% to 25-30%). According to some data, the prevalence of the syndrome among younger schoolchildren is about 10-15%, in boys it occurred 2.8-3 times more often than in girls. nine0017
The estimates of the prevalence of ADHD also depend on these factors (from 1-2% to 25-30%). According to some data, the prevalence of the syndrome among younger schoolchildren is about 10-15%, in boys it occurred 2.8-3 times more often than in girls. nine0017
Definition and criteria for diagnosis
Currently, the basis for establishing a diagnosis is a phenomenological psychological characteristic. Many of the signs of ADHD appear only occasionally.
Impulsivity
One of the main signs of ADHD, along with attention disorders, is impulsivity - lack of control of behavior in response to specific demands. Clinically, these children are often characterized as reacting quickly to situations, not waiting for directions and instructions to complete the task, and inadequately assessing the requirements of the task. As a result, they are very careless, inattentive, careless and frivolous. These children often fail to consider the potentially negative, harmful, or destructive (and even dangerous) consequences that may be associated with certain situations or their actions.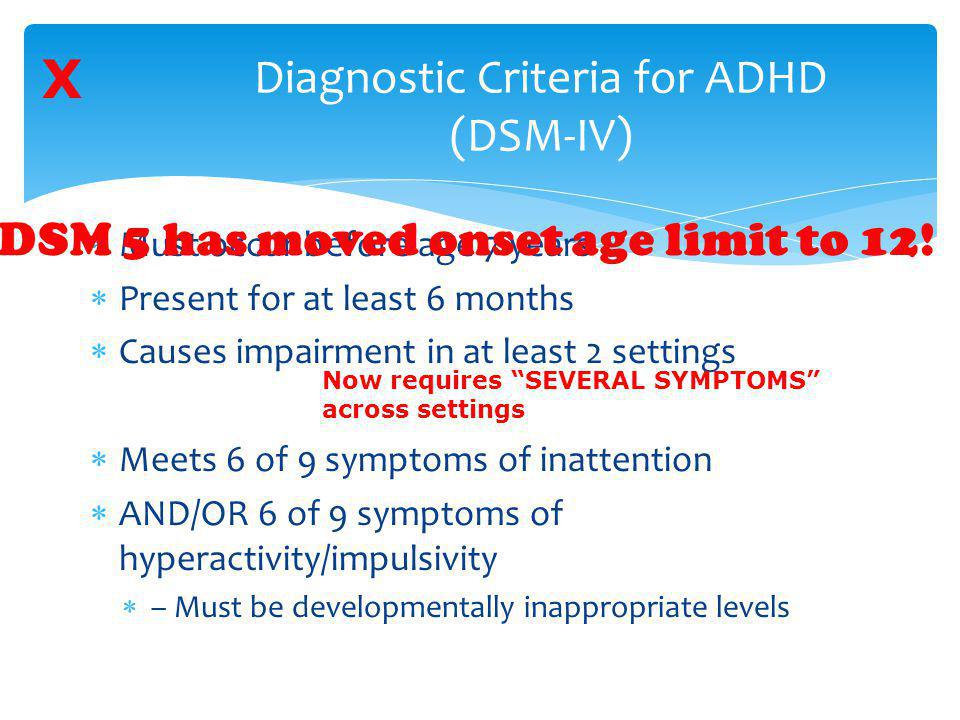 Often they expose themselves to unreasonable, unnecessary risks in order to show their courage, whims and quirks, especially in front of their peers. As a result, accidents with poisoning and injuries are not uncommon. Children with ADHD may carelessly damage or destroy someone's property much more often than children without signs of ADHD. nine0017
Often they expose themselves to unreasonable, unnecessary risks in order to show their courage, whims and quirks, especially in front of their peers. As a result, accidents with poisoning and injuries are not uncommon. Children with ADHD may carelessly damage or destroy someone's property much more often than children without signs of ADHD. nine0017
One of the difficulties in diagnosing ADHD is that it is often accompanied by other problems. A small group of people with ADHD suffer from a rare disorder called Tourette's syndrome.
DSM-IV Diagnostic Criteria for ADHD
I. Choice of option A or B:
A. INATTENTION Diagnosis requires six or more of the following symptoms of inattention that persist for at least six months and are severe enough to indicate a lack of adjustment and inconsistency with normal age characteristics:
- Often unable to pay attention to details; due to negligence, frivolity, makes mistakes in school assignments, in work performed and other activities.
- Usually has difficulty maintaining attention when performing tasks or playing games.
- It often seems that the child does not listen to the speech addressed to him.
- Often fails to follow the instructions given and to complete the lessons, homework or duties at the workplace (which has nothing to do with negative or protest behavior, inability to understand the task). nine0039
- Often has difficulty organizing tasks and other activities independently.
- Usually avoids involvement in tasks that require sustained mental effort (eg, schoolwork, homework).
- Frequently loses things needed at school and at home (eg toys, school supplies, pencils, books, work tools).
- Easily distracted by extraneous stimuli. nine0038 Often shows forgetfulness in everyday situations.
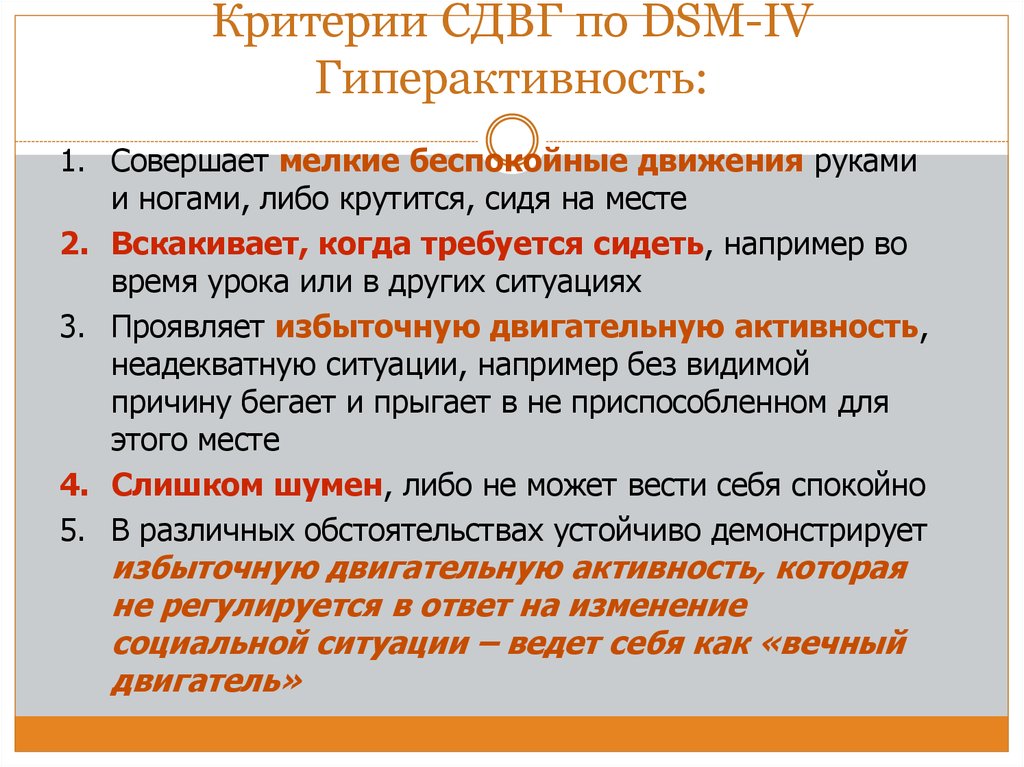
B. HYPERACTIVITY . The presence of six or more of the following symptoms of hyperactivity and impulsivity that persist for at least six months and are so pronounced that they indicate a lack of adaptation and inconsistency with normal age characteristics:
- Restless movements in the hands and feet are often observed; sitting on a chair, spinning, spinning.
 nine0039
nine0039 - Often gets up from his seat in class during lessons or other situations where he needs to stay put.
- Often shows aimless motor activity: runs, spins, tries to climb somewhere, and in such situations when it is unacceptable.
- Usually unable to play quietly, calmly, or engage in leisure activities.
- Is often in constant motion and behaves "as if a motor were attached to it".
- Often talkative. nine0039
IMPULSITY
- Often answers questions without thinking, without listening to the end.
- Usually has difficulty waiting for his turn in various situations.
- Often interferes with others, sticks to others (for example, interferes in conversations or games).
II. ( B. ) Some of the symptoms of impulsivity, hyperactivity, and inattention begin to disturb others before the age of seven. nine0017
III. ( C. ) Problems associated with the above symptoms occur in two or more settings (eg, school and home).
IV. ( D. ) There is strong evidence of clinically significant impairments in social contacts or schooling.
Adult ADHD
It turns out that more than half of the children suffering from this disorder continue to suffer from it into adulthood. In 30-70% of cases, ADHD symptoms continue into adulthood. Many adults who did not have this problem in childhood do not realize that this is precisely the reason for their inability to maintain attention, difficulties in learning new material, in organizing the space around them and in interpersonal relationships. nine0017
Treatments for ADHD
Approaches to the treatment and management of ADHD and the methods available may differ from country to country. However, despite these differences, most experts consider the most effective integrated approach, which combines several methods, individually selected in each case. Methods of behavior modification, psychotherapy, pedagogical and neuropsychological correction are used. "Drug therapy is indicated on an individual basis when the cognitive and behavioral problems in a child with ADHD cannot be managed by non-drug methods alone." nine0009 [11] In the USA, addictive [12] [13] [14] Ritalin is used for treatment.
"Drug therapy is indicated on an individual basis when the cognitive and behavioral problems in a child with ADHD cannot be managed by non-drug methods alone." nine0009 [11] In the USA, addictive [12] [13] [14] Ritalin is used for treatment.
Currently, there are several approaches to the treatment of ADHD
- Neuropsychological . When, with the help of various exercises, we return to the previous stages of ontogenesis and rebuild those functions that were formed archaically incorrectly and have already been fixed. To do this, they need, like any other ineffective pathological skill, to purposefully reveal, disinhibit, destroy and create a new skill that is more consistent with effective work. And this is carried out on all three floors of mental activity. This is a laborious, multi-month job. The child is born 9months. And neuropsychological correction is designed for this period. And then the brain begins to work more efficiently, with less energy costs.
 Old archaic connections, relations between the hemispheres are normalizing. Energy, management, active attention are built.
Old archaic connections, relations between the hemispheres are normalizing. Energy, management, active attention are built.
- Syndromic . Let's imagine that a personally mature child wants to behave in accordance with the norms, wants to learn, to perceive knowledge. His parents raised him well. He must sit quietly in class. Must be attentive and listen, control yourself. Three difficult tasks at the same time. Not a single adult person is able to perform three tasks that are difficult for him. Therefore, syndromic work is that the child is given an interesting activity (voluntary). But in this activity there is post-voluntary attention (when we become interested in something and delved into it, we already strain without additional costs). Therefore, when they say that children with ADHD are able to sit at the computer for a very long time, then this is a completely different attention. nine0039
There are outdoor games that require only the effort of attention.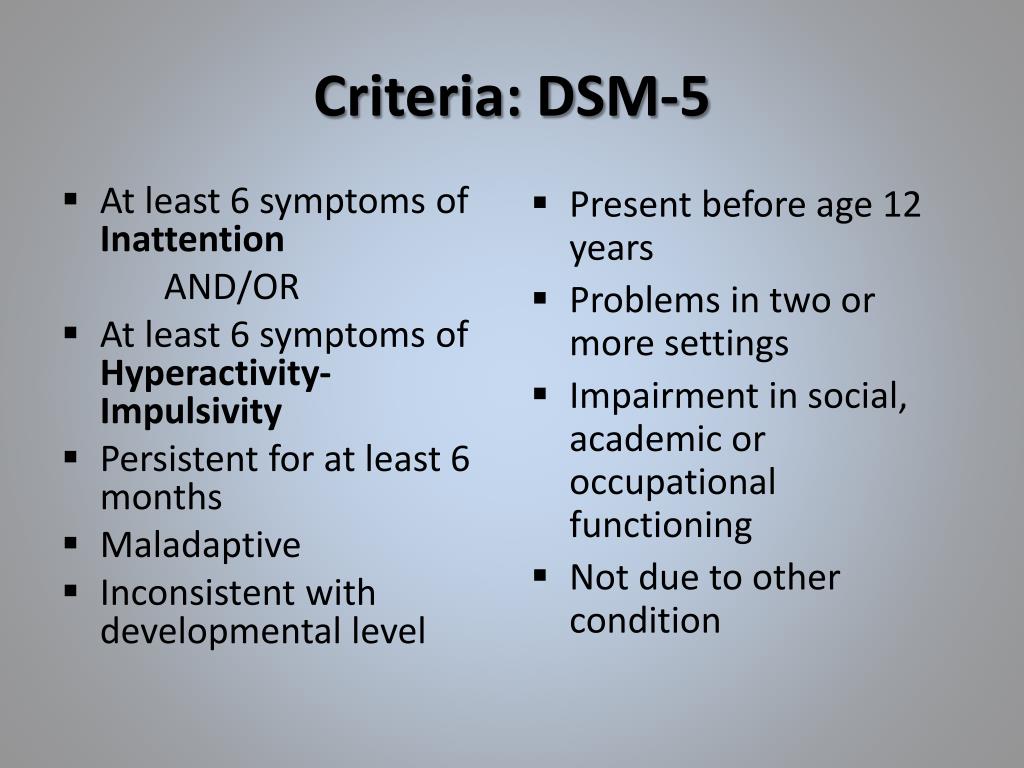 The child moves according to the conditions of the game, he can be explosive, impulsive. This may help him win. But the game is about attention. This function is being trained. Then the restraint function is trained. However, he can be distracted. Each task is solved as it arrives. This improves each feature individually.
The child moves according to the conditions of the game, he can be explosive, impulsive. This may help him win. But the game is about attention. This function is being trained. Then the restraint function is trained. However, he can be distracted. Each task is solved as it arrives. This improves each feature individually.
But no medicine teaches how to behave, so two more directions are added:
- Behavioral or Behavioral Therapy focuses on certain behavioral patterns, either shaping or extinguishing them through reward, punishment, coercion and inspiration.
- Work on personality. Family therapy , which forms the personality and which determines where to direct these qualities (disinhibition, aggressiveness, increased activity).
All this complex of methods of psychocorrection and drug treatment with timely diagnosis will help hyperactive children to compensate for violations in time and fully realize themselves in life. nine0017
nine0017
Pharmacocorrection
Drugs are used as an adjunct in the treatment of ADHD. The best known of these are psychostimulants such as methylphenidate, dextroamphetamine with amphetamine, and dextroamphetamine. One of the disadvantages of these drugs is the need to take them several times a day (the duration of action is about 4 hours). Now there are methylphenidate and dextroamphetamine with long-acting amphetamine (up to 12 hours). Other groups of drugs are also used, for example, atomoxetine. nine0017
Drug therapy is given on an individual basis when the cognitive and behavioral problems in a child with ADHD cannot be managed by non-drug interventions alone.
The United Nations Committee on the Rights of the Child has issued recommendations stating: “The Committee is concerned about reports that Attention Deficit Hyperactivity Disorder (ADHD) and Attention Deficit Disorder (ADD) are being misdiagnosed and that psychostimulants are being over-prescribed as a result despite increasing evidence of the harmful effects of these drugs.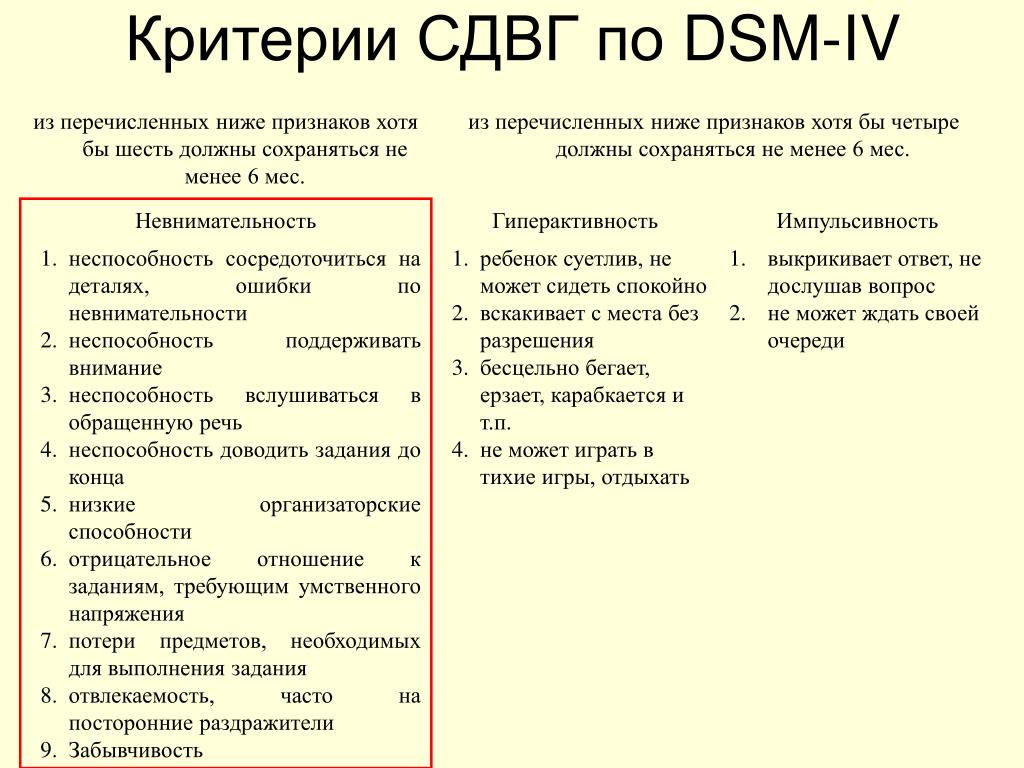 The Committee recommends further research into the diagnosis and treatment of ADHD and ADD, including the possible negative effects of psychostimulants on the physical and psychological well-being of children, and the maximum use of other forms of management and treatment when addressing behavioral disorders.” nine0009 [15]
The Committee recommends further research into the diagnosis and treatment of ADHD and ADD, including the possible negative effects of psychostimulants on the physical and psychological well-being of children, and the maximum use of other forms of management and treatment when addressing behavioral disorders.” nine0009 [15]
The approach common in the CIS is nootropic drugs, substances that improve brain function, metabolism, energy, increase the tone of the cortex. Also prescribed drugs, consisting of amino acids, which improve the metabolism of the brain. There is no evidence that such treatment is effective.
- Psychostimulants
- Pemoline
- Methylphenidate
- Dextroamphetamine
- Antidepressants nine0037
- Venlafaxine
- Nortriptyline
- Atomoxetine
Causes of ADHD
The exact cause of ADHD is not known [16] , but there are several theories. The causes of organic disorders can be:
The causes of organic disorders can be:
- General deterioration of the environmental situation.
- Infections of the mother during pregnancy and the effects of drugs, alcohol, drugs, smoking during this period.
- Immunological incompatibility (by Rh factor). nine0039
- Threats of miscarriage.
- Chronic diseases of the mother.
- Premature, transient or prolonged labor, induction of labor, anesthesia poisoning, caesarean section.
- Birth complications (improper presentation of the fetus, entanglement of the umbilical cord) lead to injuries of the fetal spine, asphyxia, internal cerebral hemorrhage.
- Any illness in infants with high fever and strong medications.
- Asthma, pneumonia, heart failure, diabetes, kidney disease can all interfere with normal brain function [17] .
Genetic factors
Specialists of the Medical Genetic Research Center of the Russian Academy of Medical Sciences and the Faculty of Psychology of Moscow State University found that “most researchers agree that a single cause of the disease cannot be identified and, it seems, will never be possible” [18] . Scientists from the United States, Holland, Colombia and Germany have suggested that 80% of the occurrence of ADHD depends on genetic factors. Out of more than thirty candidate genes, three were selected - the dopamine transporter gene, as well as two dopamine receptor genes. However, the genetic prerequisites for the development of ADHD are manifested in interaction with the environment, which can strengthen or weaken these prerequisites [18] .
Scientists from the United States, Holland, Colombia and Germany have suggested that 80% of the occurrence of ADHD depends on genetic factors. Out of more than thirty candidate genes, three were selected - the dopamine transporter gene, as well as two dopamine receptor genes. However, the genetic prerequisites for the development of ADHD are manifested in interaction with the environment, which can strengthen or weaken these prerequisites [18] .
Other common comorbidities
- Asperger's Syndrome
- Bipolar affective disorder
- Dyslexia
- Tourette syndrome
Forecast
Individuals with this disease have to put up with a number of restrictions.
Criticism
ADHD is one of the most questionable and controversial mental disorders [19] [20] ADHD and its treatment have been questioned since at least 1970s. [6] [21] [22] Many doctors, teachers, high-ranking politicians, parents and the media doubt the existence of ADHD. The range of opinions about ADHD is quite wide - from those who do not believe that ADHD exists, to those who believe that there are genetic or physiological prerequisites for this condition. [6]
The range of opinions about ADHD is quite wide - from those who do not believe that ADHD exists, to those who believe that there are genetic or physiological prerequisites for this condition. [6]
Researchers at Canada's McMaster University have identified five main points on which the debate is evolving:
- Clinical diagnosis for which there are no laboratory or radiological diagnostic tests or physical features of the body.
- Criteria for diagnosis changed frequently.
- There is no effective treatment. Existing methods of treatment are very long.
- In the treatment, drugs are used, some of which contain narcotic substances (methylphenidate, dextroamphetamine). nine0038 The number of diagnoses varies considerably across countries. [23]
In 1998, the National Institutes of Health hosted a conference on ADHD. By the end of the conference, they came to the following conclusion:
".
..We do not have an independent, reliable test for ADHD and there is no evidence that ADHD is caused by a brain disorder."
Original text
"...We do not have an independent, valid test for ADD/ADHD and there are no data to indicate that ADD/ADHD is due to a brain malfunction." [24]
Lack of clarity about what could be classified as ADHD and changes in criteria for diagnosis led to confusion. [25] Ethical and legal issues regarding treatment have been major areas of controversy, especially the use of psychostimulants in treatment, and the advertising of stimulants for the treatment of ADHD by groups and individuals who receive money from pharmaceutical companies. nine0009 [20]
Medical professionals and news agencies have argued that the diagnosis and treatment of this disorder deserves more thorough investigation. [26]
Alternative theories [27] such as Hunter vs. farmer theory, Neurodiversity and Social construct theory of ADHD have been proposed to explain the symptoms of ADHD.
farmer theory, Neurodiversity and Social construct theory of ADHD have been proposed to explain the symptoms of ADHD.
Some individuals and groups completely deny the existence of ADHD. These include Thomas Szasz, Michel Foucault, and groups such as the Citizens' Commission on Human Rights (CCHR). nine0009 [28] However, most US medical authorities and courts consider ADHD diagnoses to be legitimate. (See Ritalin class action lawsuits)
Literature
In Russian
- Altherr P., Berg L., Wölfl A., Passolt M. Hyperactive children. Correction of psychomotor development. - M: Publishing Center "Academy", 2004
- Bryazgunov I.P., Kasatikova E.V. Restless child or all about hyperactive children. - M.: Publishing House of the Institute of Psychotherapy, 2002
- Bryazgunov I.P., Kasatikova E.V. Attention deficit hyperactivity disorder in children. - M.: Medpraktika-M, 2002
- Zavadenko N.N. Hyperactivity and attention deficit in childhood.
 - M.: Publishing center "Academy", 2005.
- M.: Publishing center "Academy", 2005. - Zavadenko N.N. How to understand a child: children with hyperactivity and attention deficit. - School-Press, 2001
- Zavadenko N.N., Suvorinova N.Yu., Rumyantseva M.V. Attention deficit hyperactivity disorder: risk factors, age dynamics, diagnostic features. - Defectology, 2003, No. 6
- Monina G.B., Lyutova-Roberts E.K., Chutko L.S. hyperactive children. Psychological and pedagogical correction. - St. Petersburg: Speech, 2007
- Murashova E.V. Children are “mattresses” and children are “catastrophes”. Hypodynamic and hyperdynamic syndrome" - Yekaterinburg: U-Factoria, 2004.
- Russell A. Barclay, Christina M. Benton. Your naughty child. - St. Petersburg: Peter, 2004
- Chutko L.S., Pal'chik A.B., Kropotov Yu.D. Attention deficit hyperactivity disorder in children and adolescents. - St. Petersburg: SPbMAPO Publishing House, 2004
- Chutko L.S. Attention deficit hyperactivity disorder and concomitant disorders.
 - St. Petersburg: Hoka, 2007
- St. Petersburg: Hoka, 2007
In foreign languages
- Hartmann, Thom "Attention Deficit Disorder, A Different Perception" subtitled "A Hunter in a Farmers World".
- Barkley, Russell A. Take Charge of ADHD: The Complete Authoritative Guide for Parents (2005) New York: Guilford Publications.
- Bellak L, Kay SR, Opler LA. (1987) "Attention deficit disorder psychosis as a diagnostic category". nine0005 Psychiatric Developments , 5(3), 239-63. PMID 3454965
- Conrad, Peter Identifying Hyperactive Children (Ashgate, 2006).
- Crawford, Teresa I'm Not Stupid! I'm ADHD!
- Green, Christopher, Kit Chee, Understanding ADD ; Doubleday 1994; ISBN 0-86824-587-9
- Hanna, Mohab. (2006) Making the Connection: A Parent's Guide to Medication in AD/HD , Washington D.C.: Ladner-Drysdale.
- Joseph, J. (2000). "Not in Their Genes: A Critical View of the Genetics of Attention-Deficit Hyperactivity Disorder", Developmental Review 20, 539-567.
- Kelly, Kate, Peggy Ramundo. (1993) You Mean I'm Not Lazy, Stupid or Crazy?! A Self-Help Book for Adults with Attention deficit Disorder . ISBN 0-684-81531-1
- Matlen, Terry. (2005) "Survival Tips for Women with AD/HD". ISBN 1886941599
- Ninivaggi, F.J. "Attention-Deficit/Hyperactivity Disorder in Children and Adolescents: Rethinking Diagnosis and Treatment Implications for Complicated Cases", Connecticut Medicine . September 1999; Vol. 63, no. 9, 515-521. PMID 10531701
Notes
- ↑ LONI: Laboratory of Neuro Imaging
- ↑ NINDS Attention Deficit-Hyperactivity Disorder Information Page. National Institute of Neurological Disorders and Stroke (NINDS/NIH) February 9, 2007. Accessed 2007-08-13.
- ↑ Russell A. Barkley Official Site, Authority ADHD, Attention Deficit Hyperactivity Disorder
- ↑ Attention-Deficit/Hyperactivity Disorder (ADHD). Data from Behavenet.
 com . Information collected on December 11, 2006.
com . Information collected on December 11, 2006. - ↑ Vincent Parrillo Encyclopedia of Social Problems. - SAGE, 2008. - P. 63. - ISBN 9781412941655
- ↑ 1 2 3 4 Treatment of Attention-Deficit/Hyperactivity Disorder. US department of health and human services (December 1999). Retrieved October 2, 2008.
- ↑ Mayes R, Bagwell C, Erkulwater J (2008). "ADHD and the rise in stimulant use among children". Harv Rev Psychiatry 16 (3): 151–66. DOI:10.1080/10673220802167782. PMID 18569037.
- ↑ Developmental psychopathology. - Chichester: John Wiley & Sons, 2006. - ISBN 0-471-23737-X
- ↑ ADD/ADHD Health Center. Information from WebMD.com . Data collected December 11, 2006.
- ↑ Attention deficit/hyperactivity disorder.
 E.D. Belousova, M.Yu. Nikanorov. Department of Psychoneurology and Epileptology, Moscow Research Institute of Pediatrics and Pediatric Surgery, Ministry of Health of the Russian Federation
E.D. Belousova, M.Yu. Nikanorov. Department of Psychoneurology and Epileptology, Moscow Research Institute of Pediatrics and Pediatric Surgery, Ministry of Health of the Russian Federation - ↑ Attention deficit hyperactivity disorder in children: modern approaches to pharmacotherapy N.N. Zavadenko, N.Yu. Suvorinova, N.V. Grigoriev. Department of Nervous Diseases, Faculty of Pediatrics, Russian State Medical University, Moscow
- ↑ RIA Novosti
- ↑ Belgian tragedy: is the "American Syndrome" to blame?
- ↑ Ritalin addiction help
- ↑ http://www.cchr.ru/press1.html Child psychiatrists in Australia, Finland and Denmark received
- ↑ Stimulant medication for the treatment of attention-deficit hyperactivity disorder: evidence-b(i)ased practice? -- Bailly 29 (8): 284 -- Psychiatric Bulletin. nine0038 ↑ Article about ADHD on the website of the Faculty of Psychological and Pedagogical Management of the Higher School of Social and Management Consulting
- ↑ 1 2 Genetics of Hyperactivity and Attention Deficit//Chemistry and Life.
 2008. No. 1., p. 5
2008. No. 1., p. 5 - ↑ Mayes R, Bagwell C, Erkulwater J (2008). "ADHD and the rise in stimulant use among children". Harv Rev Psychiatry 16 (3): 151–66. DOI:10.1080/10673220802167782. PMID 18569037. Foreman, D. M. (2006). "Attention deficit hyperactivity disorder: legal and ethical aspects" (REVIEW, full text). Archives of Disease in Childhood 91 (2): 192-94. DOI:10.1136/adc.2004.064576. PMID 16428370.
- ↑ Vincent Parrillo Encyclopedia of Social Problems. - SAGE, 2008. - ISBN 9781412941655
- ↑ Developmental psychopathology. - Chichester: John Wiley & Sons, 2006. - ISBN 0-471-23737-X
- ↑ Jadad AR, Booker L, Gauld M, et al (December 1999). "The treatment of attention-deficit hyperactivity disorder: an annotated bibliography and critical appraisal of published systematic reviews and metaanalyses".
 Canadian journal of psychiatry. Revue canadienne de psychiatrie 44 (10): 1025–35. PMID 10637682.
Canadian journal of psychiatry. Revue canadienne de psychiatrie 44 (10): 1025–35. PMID 10637682. - ↑ www.adhdtesting.org A real look inside the issue
- ↑ PBS - frontline: medicating kids: adhd: american academy of pediatrics' guidelines.
- ↑ BBC NEWS.
- ↑ Rethinking ADHD >> Palgrave.com: Title Page.
- ↑ Citizens Commission On Human Rights - Australia (CCHR Australia).
External links
In Russian
- Attention deficit hyperactivity disorder. (ADHD)
- Attention deficit hyperactivity disorder in children: modern approaches to pharmacotherapy
- Attention Fund
- Attention Deficit Hyperactivity Disorder in Children (ADHD)
- Articles on ADHD
- About Attention Deficit Hyperactivity Disorder (ADHD-ADHD)
- Physician reports on ADHD
- Psychiatry Chapter 18 Attention Disorder with Hyperactivity Disorder P.
 Wander, R. Scheider
Wander, R. Scheider - Attention deficit hyperactivity disorder in children: modern approaches to pharmacotherapy
Critical
- Citizens Commission on Human Rights. ADHD and "learning disorder"
- Dangerous psychiatric diagnosis
- Pseudoscience
- Invented "diseases" are the product of fraud
- Fred Baughman, excerpt from The ADHD Fraud: How Psychiatry Makes Patients Out of Normal Children
- "Mirror of the Week", No. 36 (360) September 15 - 21, 2001, "TABLET" PEDAGOGY
- Blog "Psychology versus psychiatry - the fight of the century!"
- The Truth about ADHD from their mouth! (video)
- Psychiatrist Thomas Szas about psychiatry [1] (video)
English
- Live with Dr. Fred Baughman: ADHD fraud and the chemical holocaust against a generation of children. — Taichung: Truth Publishing International, Ltd., 2005.
- adhd
- Attention-Deficit / Hyperactivity Disorder (ADHD) at the Center for Disease Control
- Diagnosis and Treatment of Attention Deficit Hyperactivity Disorder at NIH
- National Institute of Mental Health on ADHD
- The History of ADHD: 1798, Alexander Crichton, with pictures of the original works and sources.