Abilify makes me tired
Aripiprazole Side Effects: Common, Severe, and More
Written by Keri Wiginton
In this Article
- Muscle Movement Problems
- Metabolic Changes and Weight Gain
- Desire to Sleep
- Compulsive Behavior
- Neuroleptic Malignant Syndrome (NMS)
- Other Common Side Effects
- Less Common Side Effects
- Serious Side Effects
- After You Start Aripiprazole
- What Else You Should Know
If you have schizophrenia, your doctor may want you to take aripiprazole. That’s a prescription drug sold under the brand name Abilify.
Aripiprazole is an atypical or second-generation antipsychotic (SGA). It balances out your dopamine and serotonin levels. These are chemicals in your brain that affect how you think, feel, and act. Your thoughts may become clearer on this drug. You may stop hearing or seeing things that aren’t there. Your mood and motivation may get better.
Oral forms of the drug can also treat Tourette’s syndrome and symptoms of bipolar 1 disorder. Aripiprazole may help calm irritability in children and teens with autism. Your doctor may use it with other medicine to treat depression. You can get a shot of aripiprazole to treat agitation with schizophrenia or bipolar mania.
Aripiprazole can help your mind become more stable. But like any drug, it can cause unwanted side effects. Some are mild, but others can be serious. Talk to your doctor about what can happen if you or your child take this medicine.
Muscle Movement Problems
Restlessness. In clinical trials, about 8% of adults with schizophrenia reported akathisia. That’s a movement disorder that makes it hard to stay still. You may feel like you need to do something with your legs. You may want to pace or rock back and forth. It feels different than agitation or anxiety.
Extrapyramidal symptoms (EPS). If you’re younger than 20, you’re more likely to have muscles that move or twitch on their own. A review of 41 studies showed about 17% of young people on aripiprazole get EPS.
Symptoms of EPS include:
- Repeated muscle contractions (dystonia)
- Urge to move around (akathisia)
- Body parts that shake (tremor)
- Inability to bend (parkinsonism)
Tardive dyskinesia. This is a disorder where you can’t control the muscles in your tongue, mouth, face, and upper body. It can happen after you use antipsychotics for a long time. You’re more likely to get it if you have other medical or movement problems. But your chances may be lower on aripiprazole than older antipsychotics and some other SGAs. Tardive dyskinesia may stop once you quit your medicine. But sometimes it doesn't go away.
Metabolic Changes and Weight Gain
Atypical antipsychotics may boost your appetite or change how your body uses energy. This may lead to weight gain. Sometimes, these drugs can raise your blood sugar or cholesterol levels. That can make it more likely that you’ll have diabetes and heart disease.
But when compared to similar drugs, aripiprazole may lead to less weight gain and problems with your metabolism.
Children on SGAs are more likely to gain weight than adults, especially if they have schizophrenia or autism. But adolescents who take aripiprazole may gain less weight than kids on other antipsychotics.
Your doctor may want to keep an eye on your or your child’s weight. They may want to watch your glucose and cholesterol levels, too. In the meantime, make sure you eat a balanced diet and get plenty of exercise.
Desire to Sleep
Aripiprazole can make you tired. Somnolence, or a strong urge to sleep, is more common in children. The effects may be higher with bigger doses. But aripiprazole may cause less somnolence than similar drugs. It may go away with time.
Compulsive Behavior
It’s rare, but you may get an urge to gamble that you can’t resist. Less often, you may feel the need to have sex, shop, or eat in a way you can’t control. If your loved one acts like this, you may need to tell them. They may not know it’s not normal.
These urges usually go away when your doctor lowers your dosage or stops the medicine. But always talk to your doctor before you quit aripiprazole.
But always talk to your doctor before you quit aripiprazole.
Neuroleptic Malignant Syndrome (NMS)
Rarely, this drug can cause a possibly fatal set of symptoms. NMS can affect your heart, muscles, and kidneys. You may also get:
- A high fever
- Stiff muscles
- A change in your mental state
- Irregular heartbeat or blood pressure
- High heart rate
- A lot of sweating
If you have any of these symptoms, check with your doctor right away. They’ll want to rule out other medical conditions first. If your medicine is the problem, you’ll stop taking aripiprazole right away. You’ll get treatment for your other symptoms.
Other Common Side Effects
In clinical trials, at least 10% of all adults (including those without schizophrenia) also had:
- Nausea
- Throwing up
- Constipation
- Headache
- Dizziness
- Anxiety
- Insomnia
At least 10% of all children and young adults (including those without schizophrenia) also had:
- Headache
- Tiredness
- Increased hunger
- Insomnia
- Nausea
- Symptoms of the common cold
Less Common Side Effects
Some people may have drooling or get blurry vision, dry mouth, or a rash.
Serious Side Effects
In elderly people. Aripiprazole should not be used to treat dementia-related psychosis in older people. It may make their chances of stroke and death greater. The drug may make elderly people sleepy and lightheaded. They may not be able to swallow easily. This may raise their chances of injuries from falls or choking.
In young people. Antidepressants may raise the chances of suicidal thoughts in people younger than 24. If you care for a child or teenager on antidepressants, watch them closely for changes in their behavior. This is even more important during the first few months of treatment or if their dose changes. If you get worried, talk to your doctor.
After You Start Aripiprazole
Don’t drink alcohol or use illegal drugs when you take aripiprazole. Your medicine may not work as well if you do. You may also have worse side effects, like sleepiness.
Don’t operate machines or drive until you know how you’ll react to aripiprazole. Since it makes you drowsy, you may be more likely to have an accident. You may fall and hurt yourself if you’re tired.
Since it makes you drowsy, you may be more likely to have an accident. You may fall and hurt yourself if you’re tired.
You should tell your doctor if you exercise a lot or if you’re going to be somewhere that’s hot. That’s because the medicine may make it harder for your body to cool off. You should make sure to drink enough water.
What Else You Should Know
Your side effects may go away with time. But tell your doctor if you have any symptoms that you can’t control. They’ll help you figure out if you need to lower your dose or quit taking the drug.
Even if you feel better, don’t stop taking your medicine. You’ll need ongoing treatment for your schizophrenia. And your symptoms may come back if you miss a dose. If you want to change or stop your medicine, talk to your doctor. They’ll let you know when it’s safe to adjust your aripiprazole.
If you want to get pregnant, talk to your doctor. It may not be safe for you or your baby for you to stop your schizophrenia treatment. Your doctor can help you decide what to do about your medicine. You should also know that aripiprazole will get into your breast milk. Talk to your doctor before you start breastfeeding.
Your doctor can help you decide what to do about your medicine. You should also know that aripiprazole will get into your breast milk. Talk to your doctor before you start breastfeeding.
Abilify side effects and how to avoid them
Abilify treats conditions like depression, schizophrenia, and Tourette’s disorder but it has potential side effects, warnings, and drug interactions that you should know about
Abilify side effects | Serious side effects | How long do side effects last? | Warnings | Interactions | How to avoid side effects | Resources
Abilify is a brand-name prescription drug approved by the FDA to treat schizophrenia, major depressive disorder (in combination with other medications), and, in children, Tourette’s disorder and irritability associated with autistic disorder. Abilify can also be used alone or in combination with lithium or valproate to treat manic episodes in people diagnosed with bipolar I disorder. Abilify is also available as Abilify MyCite (which contains a sensor), or Abilify Maintena (a monthly injection).
The active ingredient in Abilify is aripiprazole, an atypical antipsychotic. The exact way Abilify works is not known, but it is thought to work by acting on dopamine and serotonin receptors in the brain. As with all antipsychotic drugs, Abilify has a number of side effects, warnings, restrictions, and drug interactions that may cause problems, so it helps to understand the downsides before starting this medicine.
RELATED: What is Abilify?
Common side effects of Abilify
The most common side effects of Abilify are:
- Headache
- Increased appetite/weight gain
- Drowsiness/sleepiness/sedation
- Agitation
- Insomnia
- High blood sugar
- Anxiety
- Stomach problems: nausea, constipation, vomiting
- Dizziness/lightheadedness
- Muscle and joint pain
- Sore throat
- Blurred vision
- Drooling/excess salivation
- Restlessness
- Compulsive behaviors
- High cholesterol
- Dry mouth
- Tremor
- Urine leakage
- Cough
- Changes in body temperature
- Fever and diarrhea (in children)
In addition to these side effects, approximately 12% of people taking Abilify MyCite in clinical trials experienced skin rashes where the MyCite patch was affixed.
Serious side effects of Abilify
The most serious side effects of Abilify include:
- Drug-induced movement problems (extrapyramidal effects) including akathisia, tardive dyskinesia, and dystonia
- Suicidal thoughts
- Worsening depression
- Stroke/mini-stroke
- Fainting and falling
- Orthostatic hypotension (sudden drop in blood pressure when standing)
- Seizures
- Diabetes
- Severe difficulty swallowing
- Body temperature dysregulation
- High blood pressure (hypertension)
- Heart rate changes
- Intestinal obstruction
- Gallbladder stones
- Swelling of the pancreas (pancreatitis)
- Blood problems
- Low white blood cell counts
- Potassium imbalance
- Muscle damage
- Neuroleptic malignant syndrome (NMS)
- Severe allergic reactions
Patients who experience a serious reaction should notify their doctor or get emergency medical help right away. Severe allergic reactions require immediate emergency medical attention. Symptoms may include hives, difficulty breathing, or swelling around the face, lips, mouth, and tongue.
Severe allergic reactions require immediate emergency medical attention. Symptoms may include hives, difficulty breathing, or swelling around the face, lips, mouth, and tongue.
How long do side effects last?
Aripiprazole has a half-life of 75 hours and its active metabolite, which works like aripiprazole, has a half-life of 94 hours. This means that many of the common side effects of aripiprazole such as headache, drowsiness, agitation, and anxiety, could take several days or even several weeks to resolve after the last dose is taken. Some side effects, such as headache and akathisia, may get better as the body adjusts to the drug.
The metabolic side effects of aripiprazole such as high blood sugar, high fats, high cholesterol, and weight gain may require treatment.
Serious side effects such as extrapyramidal symptoms, severe allergic reactions, stroke, gallbladder stones, pancreatitis, heart rate irregularities, or low white blood cell counts may require emergency medical treatment. Some, like stroke or diabetes, may have lifelong complications. Extrapyramidal symptoms can clear up within a few weeks or they may persist for years and require a medication or dosage change.
Some, like stroke or diabetes, may have lifelong complications. Extrapyramidal symptoms can clear up within a few weeks or they may persist for years and require a medication or dosage change.
Abilify contraindications & warnings
Abuse and dependence
Abilify is not a controlled substance, so healthcare professionals do not consider it an addictive drug. It also does not cause dependence, but may cause withdrawal when stopped abruptly. People taking Abilify should consult with a healthcare professional before stopping this medicine.
Overdose
Taking too much Abilify is serious but probably not lethal. If too much Abilify is taken, seek emergency medical care or call a poison helpline. There are some symptoms that may signal an oral Abilify overdose. These include:
- Vomiting
- Somnolence
- Tremor
- Aggression
- Heart rate changes
- Blood pressure changes
- Confusion
- Lethargy
- Convulsions
- Loss of consciousness
- Coma
Restrictions
Not everyone can safely take Abilify. The hazards may be too great for some people, but others may be able to take Abilify with careful monitoring for adverse reactions. Restrictions include:
The hazards may be too great for some people, but others may be able to take Abilify with careful monitoring for adverse reactions. Restrictions include:
- Hypersensitivity: People with allergies to aripiprazole or any of the inactive ingredients of Abilify can never be given this medicine.
- Older adults with dementia-related psychosis cannot be given antipsychotic drugs like Abilify because of the increased risk of death.
- Children, adolescents, and young adults are at a higher risk for worsening depression and suicide. Patients of any age require careful monitoring by both healthcare professionals and caregivers when taking Abilify.
- Cardiovascular disease: Patients with known cardiovascular problems such as heart attack, heart failure, ischemic heart disease, or heart rate problems will require close monitoring when taking Abilify.
- Cerebrovascular disease: People with a history of strokes or other cerebrovascular problems will also need careful monitoring.

- Diabetes: Antipsychotics, including Abilify, can cause high blood sugar, so regular blood sugar testing is required in people with diabetes or prediabetes.
- Low blood pressure, low blood volume, or dehydration: Because Abilify can cause blood pressure problems, any condition that raises the risk of low blood pressure will require monitoring when Abilify is prescribed.
- Seizure disorders: Abilify can cause seizures, so people with a history of seizures will be prescribed Abilify with caution.
- History of low white blood cell counts: People predisposed to problems with white blood cells will need to have regular blood tests to monitor the effects of Abilify on white blood cells.
- Aspiration pneumonia: Abilify can make swallowing difficult, raising the risk that food or drink will be aspirated and possibly cause aspiration pneumonia.
 People who are at risk for aspiration pneumonia will require close monitoring.
People who are at risk for aspiration pneumonia will require close monitoring.
Finally, aripiprazole can throw off the body’s ability to regulate body temperature, resulting in hyperthermia or hypothermia. People taking Abilify then, are vulnerable to extreme environmental temperatures. They should be cautious when temperatures get too hot or too cold, dress appropriately, and even limit going outside when the weather is extreme.
Pregnancy and nursing
Women who are pregnant or considering pregnancy should consult with a healthcare provider about the benefits and risks of taking Abilify while pregnant. There is no evidence that Abilify will harm a fetus, but when atypical antipsychotics are taken during the third trimester, there is a risk that babies will be born with withdrawal symptoms and extrapyramidal side effects (involuntary movement problems).
Women who are breastfeeding should talk to their healthcare provider. Aripiprazole is present in human breast milk and there are reports of reduced milk production in lactating women and poor weight gain in nursing infants.
Children
The U.S. Food and Drug Administration (FDA) has approved Abilify to treat schizophrenia in children as young as 13 years of age, bipolar I disorder in children as young as 10 years of age, and Tourette syndrome or autistic disorder in children as young as 6 years of age. Because of the increased risk for suicide, children and adolescents will need to be closely watched for worsening depression, thoughts of suicide, or suicidal behaviors.
Older adults
People ages 65 and older can take Abilify in the same doses as younger adults, but the starting dose may be lower. However, there is an increased risk for falls and other injuries, so other drugs that cause sleepiness or impairment may need to be adjusted. Healthcare providers are also advised not to use Abilify in seniors with dementia-related psychosis.
Abilify interactions
Like other antipsychotic medications, Abilify has several potentially harmful drug interactions.
- Antipsychotic drugs: First-generation and atypical antipsychotics produce many of the same side effects as Abilify.
 Combining more than one antipsychotic, then, increases the risk and possibly the severity of side effects.
Combining more than one antipsychotic, then, increases the risk and possibly the severity of side effects. - CNS depressants: Abilify reduces symptoms of schizophrenia and mania because it slows down the brain, that is, it is a central nervous system depressant. Many of the side effects such as fatigue, sleepiness, dizziness, and lightheadedness are due to the depressant effects of Abilify. Combining Abilify with other CNS depressants will worsen mental impairment and coordination problems caused by Abilify, and can slow or even stop breathing. These especially include sleeping pills, barbiturates, anxiety medications, opioid pain relievers, muscle relaxants, benzodiazepines, and alcohol, among others.
- Drugs that increase the side effects of aripiprazole: Some drugs block the ability of the liver to break down aripiprazole and its active metabolite, causing aripiprazole to stay in the bloodstream at higher concentrations for a longer period.
 The strongest inhibitors of aripiprazole, such as the antidepressants Prozac (fluoxetine) and Paxil (paroxetine), the antifungal drugs ketoconazole or itraconazole, or the heart rhythm drug quinidine may require the Abilify dose to be cut in half.
The strongest inhibitors of aripiprazole, such as the antidepressants Prozac (fluoxetine) and Paxil (paroxetine), the antifungal drugs ketoconazole or itraconazole, or the heart rhythm drug quinidine may require the Abilify dose to be cut in half. - Drugs that reduce the effectiveness of aripiprazole: Some drugs speed up the body’s metabolism of aripiprazole, such as carbamazepine. These drugs reduce the effectiveness of Abilify, so the Abilify dose may need to be increased.
- Blood pressure medications: Abilify can lower blood pressure, so careful blood pressure monitoring is required when it’s combined with blood pressure medications.
How to avoid Abilify side effects
Most people taking antipsychotic medications will experience side effects. Abilify is no exception, though some of the most unpleasant side effects of traditional antipsychotics are less common when taking Abilify. Still, there are many good rules of thumb for avoiding or minimizing side effects when taking Abilify.
1. Tell the healthcare provider about all medical conditions and medications
For any prescription drug, the first line of defense against side effects is to make sure that the prescribing healthcare provider has a complete medical history. For Abilify, the healthcare provider particularly needs to know about:
- Diabetes or a family history of high blood sugar
- Seizures
- High or low blood pressure
- Heart problems
- Stroke
- Low white blood cell counts
- Pregnancy or pregnancy plans
- Breastfeeding or plans to breastfeed
Side effects can also be due to drug interactions. The best way to avoid drug interactions is to keep a list of all drugs being taken including prescription or over-the-counter drugs as well as dietary supplements and herbal remedies. Always share this list with the prescribing healthcare provider.
2. Keep all appointments
Visits with the prescribing healthcare provider are another important defense against side effects. If there are side effects, keep a list and share it with the healthcare provider at each visit. The healthcare provider may be able to prescribe other drugs to help with certain side effects such as headache, constipation, or tremor—or, change the dose or the medication altogether. Sleeplessness could be solved by changing the timing of each day’s dose. Finally, tests may need to be regularly performed to spot problems before they turn into serious medical problems.
3. Watch for symptoms of potentially serious side effects
Some side effects are or can develop into severe medical conditions. Abilify, unfortunately, has many severe side effects to watch out for, but there are signs and symptoms that signal there may be a serious problem, particularly:
- Seizures
- Weakness
- High fever
- Chills
- Excessive sweating
- Slow, fast, or uneven heartbeat
- Extreme hunger or thirst
- Increased urination
- Unusual urges or compulsions
- Severe agitation
- Feeling lightheaded or dizzy when standing up
- Difficulty swallowing
- Uncontrolled muscle movement or shaking
- Hives, rash, or swelling
- Unusual bruising or bleeding
If any of these problems are noticed while taking Abilify, immediately call a healthcare professional for medical advice or seek emergency medical attention when needed.
4. Take Abilify as directed
Take Abilify exactly as instructed. Do not change the doses or stop taking Abilify without getting the medical advice of the prescribing healthcare provider.
5. Do not miss doses
Abilify doses need to be taken daily to provide maximum therapeutic benefits. If a dose is missed, take it as soon as it’s remembered. If it’s almost time for the next dose, however, skip the missed dose and take the next dose on time. Do not double up on doses. If missing doses becomes a problem, a pharmacist can provide useful tools to help remember doses such as alarms, pillboxes, smartphone apps, and even pill bottle caps that have alarms. Or, you may want to talk to your doctor about other forms of Abilify such as Abilify MyCite or Abilify Maintena.
6. Don’t drink alcohol
As a drug that slows down the brain, Abilify doesn’t mix well with alcohol. The combination will worsen mental impairment and increase the risk of falling and accidents. It can also decrease blood pressure and cause breathing to slow or even stop.
It can also decrease blood pressure and cause breathing to slow or even stop.
7. Be careful about driving and other risky activities
Abilify can cause sleepiness, blurred vision, and mental impairment. Use good judgment about driving or engaging in risky activities. Do not drive until you know how Abilify affects you. You shouldn’t drive if you experience side effects such as blurred vision.
Resources
- Abilify, Epocrates
- Abilify MyCite prescribing information, U.S. National Library of Medicine
- Abilify prescribing information, U.S. National Library of Medicine
- Aripiprazole drug summary, Prescriber’s Digital Reference
- Aripiprazole (Abilify), National Alliance on Mental Illness
- Aripiprazole withdrawal: A case report, Innovations in Clinical Neuroscience
Tieto activity a hry zabavia celú rodinu
Vianočné sviatky v spojení s lockdownom Ktoré aktivity a hry pre celú rodinu vám spríjemnia nastávajúce obdobie?
Zlepšite nalomené rodinné vzťahy vďaka spoločným aktivitám a hrám, pri ktorých sa určite nudiť nebudete. nine0007
nine0007
Escape Room u vás doma
Spoločenské únikové hry ako Escape Room, Exit alebo Únikovka sú skvelou alternatívou veľmi obľúbených, klasických Escape hier . Vyberte si jeden z pohodlia vášho domova. Hru je, pochopiteľne, možné hrať len raz, ale to isté platí aj pre jej tradičnú verziu, takže by vás to nemalo odradiť.
Skladanie papiera alebo umenie origami Na internete nájdete množstvo návodov na originálne kúsky, o ktorých by ste ani nepovedali, že sú vyrobené z papiera. nine0003 Poskladať si môžete rôzne zvieratká, vianočné ozdoby, dekorácie, ale pokojne aj postavičky z videohry Among Us.
Trending
TOP 7: Hudobné svetové rekordy, z ktorých vám padne sánka
Originálna verzia hry Hádaj kto?
Určite si spomínate na kedysi populárnu spoločenskú hru Hádaj kto? Čo ale tak namiesto kreslených postavičiek prilepiť fotografie rodinných príslušníkov či známych osobností? nine0005 Ak nemáte originálnu verziu, môžete využiť príslušenstvo z hry Scrabble alebo si hru vyrobiť.
Kreslenie a maľovanie ako balzam na dušu
Zrelaxujú, upokoja, nemusíte pri nich vôbec myslieť a ako sa hovorí, fantázii sa medze nekladú, takže máte voľnú ruku. Táto aktivita je vhodná pre celú rodinu, pričom vám úplne postačia písacie potreby a papier. Ak neviete, čo nakresliť, pokojne sa inšpirujte videom (od 2:43). nine0007
Táto aktivita je vhodná pre celú rodinu, pričom vám úplne postačia písacie potreby a papier. Ak neviete, čo nakresliť, pokojne sa inšpirujte videom (od 2:43). nine0007
Vzdelávacie hry, ktoré potrápia nejednu mozgovú bunku
Na trhu nájdete stovky vzdelávacích hier, spomedzi ktorých by sme najviac odporučili spoločenské hry Desiatka, Cortex a iKNOW . Desiatka a iKNOW patria medzi tradičné vedomostné hry s cieľom správne odpovedať alebo pre bežných smrteľníkov uhádnuť správne odpovede na otázky z rôznych oblastí. Cortex zas precvičí váš postreh, hmat a v najnovšom vydaní aj samotný čuch.
Trending
IMT Smile oslávi 30 rokov na scéne s fanúšikmi
Projekty pre šikovné ručičky
Nech ide o výrobu plyšových hračiek zo starého oblečenia, dekorácií, vlastného mydla, solí do kúpeľa či masiek na tvár , na YouTube aj Pintereste nájdete množstvo DIY projektov (z engl. Do It Yourself, teda Urob si sám – pozn. red.). Pri manuálnej práci sa odreagujete a zároveň sa zabavíte na tom, akí šikovní, prípadne menej šikovní, sú ostatní členovia rodiny.
Pátranie po vrahovi
Samozrejme, táto verzia je plne uspokojujúca, avšak o koľko zaujímavejšie by bolo preniesť hru do reality, tak ako Raj v Teórii veľkého tresku? Jedna osoba vytvorí príbeh, v ktorom sa rodinní príslušníci stanú hlavnými podozrivými a vy musíte zistiť, kto je vinný a kto nie.
Nech si vyberiete akúkoľvek aktivitu či hru pre celú rodinu0005 . Okrem toho sa nesmierne zabavíte a zblížite s rodinnými príslušníkmi, s ktorými si bežne možno príliš nerozumiete. Prípadne sa len utvrdíte v tom, prečo s nimi radšej tak často nie ste.
Trending
Filmy, z ktorých mrazí. Top 5 hororov za posledné desaťročia
Označené ako DIY escape room escaperoom lockdown origami rodina Spoločenské hry spoločné aktivity sviatky teória veľkého tresku vianoce
basics and schizophrenia / Habr 9004%
welcome, username! nine0007
This article is a logical continuation of the post on pathopsychological diagnostics. In it, I will try to tell in an accessible language about the main groups of pharmacological drugs used to treat mental illness, as well as about the mechanisms, structures and components of the human brain that are involved in this process.
In it, I will try to tell in an accessible language about the main groups of pharmacological drugs used to treat mental illness, as well as about the mechanisms, structures and components of the human brain that are involved in this process.
Disclaimer : I'm not a psychiatrist, but a psycho. I tested the drugs of all these groups on myself and observed their effects (when I was in a psychiatric hospital). In addition, I have some experience in pharmaceutical selection, but I do not have a formal education in this area. In this regard, as well as the fact that diagnosing oneself according to scientific articles is an extremely wrong thing at its core, I want to warn the reader that, before taking anything described here, it is necessary to consult a specialist. If real welders run into the post and justify the incorrectness of the stated theses, I will only be glad. nine0007
If the above does not scare you, I suggest you plunge into the fascinating world of psychopharmacology. There are a lot of letters and pictures in the post, I warn you right away.
There are a lot of letters and pictures in the post, I warn you right away.
The brain and its structure in the context of psychopharmacology
Before talking about pharmacological treatments for mental illness, it is necessary to consider some aspects of the structure and functioning of the human brain - just to make the following material clear.
Neurons and glia
Most likely, everyone present knows that the brain consists of neurons and neuroglia (special cells that perform a number of functions - trophic, structural, secretory, regulatory and protective [1, 3]) - the former are the main object of our interest, the second is not so important for this article, since most of the modern pharmacology does not have a significant effect on it (more precisely, it has only in the context of side effects).
Neurons look like this:
And glial cells - like this:
Contrary to popular belief, glial cells are quite involved in the transmission of nerve impulses [1], at least indirectly - by influencing the formation of synapses (about them - below), however, all drugs known to us affect not its cells and functions, but neurons and communication between them [4].
Consider an approximate model of the structure of a neuron:
We are interested in dendrites - processes through which the neuron receives messages from its fellows[6] (roughly speaking, the input of the neuron) and axon - the process through which the neuron transmits its message (i.e. its "output")[6 ].
Why is that? Because they are directly related to the signals that neurons transmit to each other, and in these signals the whole “spiritual life” of a person (well, almost all) is encrypted: his thoughts, memories, beliefs, preferences, etc., including, of course, what is considered a manifestation of mental illness - delusional concepts, hallucinations, and so on [4]. nine0007
Thus, the task of treating mental illness is reduced (within the biologization approach , namely, it is the basis of this article, we will talk about others separately) to the task of changing the parameters of the passage of signals between neurons and those events that occur in the neurons themselves in connection with this transfer[4]. Of course, not an arbitrary change, but directed and controlled.
Of course, not an arbitrary change, but directed and controlled.
Synapses
Next, we should consider synapse - connection of two neurons. It is important for us because it is in the synapses that the transmission of nerve impulses[6] takes place, which, as mentioned above, determines, among other things, whether a given subject will be mentally ill or not. At the conceptual level, a synapse looks like this:
First of all, it should be said that there are two types of synapses - chemical and electrical (there are also mixed ones, but they are not so interesting for us) [7]. In the first, the signal from one neuron to another is transmitted by release into the interneuronal space (so-called synaptic cleft ) of certain substances ( neurotransmitters or neurotransmitters , depending on which translation you prefer), and secondly - directly, as in the contact of wires - the current flows from one neuron to another.
We are interested in chemical synapses, because all drugs known and used in psychiatry work with them[4]. In fact, they interfere with the signal transmission process in order to change it in such a way as to reduce the manifestations of the disease. Therefore, we will have to first consider how this signal is transmitted naturally, without drugs, then determine what pathological changes in this process take place during the disease, and only then study ways to modify it. nine0007
Signal transmission between neurons
Before proceeding directly to the description of the signal transmission mechanism, we will make two important reservations: firstly, we are only considering chemical synapses here, and secondly, we give a very simplified description of this process, since the volume of the article is limited.
So, it all starts with an impulse that sends the first neuron (it is called presynaptic because it is "in front" of the synaptic cleft). An electrical impulse runs along the axon and transmits a signal that out of vesicles (special containers in which the neurotransmitter is stored) should release a certain number of molecules of the corresponding neurotransmitter into the synaptic cleft. second”, located “behind the synaptic cleft”) neuron. [4,6].
An electrical impulse runs along the axon and transmits a signal that out of vesicles (special containers in which the neurotransmitter is stored) should release a certain number of molecules of the corresponding neurotransmitter into the synaptic cleft. second”, located “behind the synaptic cleft”) neuron. [4,6].
In addition, in the postsynaptic neuron, the process of further transmission of the message is triggered by means of a second messenger, a special intracellular signaling molecule released by the postsynaptic neuron in response to the activation of the postsynaptic receptor (more on receptors below). The second messenger instructs the postsynaptic neuron to change its ion currents, propagate or inhibit neuronal electrical impulses, phosphorylate intracellular proteins, and perform many other actions [4]. nine0007
All this ultimately leads to the fact that the expression of certain genes is turned on or off in the nucleus of the postsynaptic neuron [4,8]. After a change in gene expression, a secondary cascade of events is triggered in the postsynaptic neuron. Many of them are not fully understood [4]. But for the purposes of this article, it suffices to say that this leads (or does not lead) to the generation of an impulse in this neuron and further transmission of information.
After a change in gene expression, a secondary cascade of events is triggered in the postsynaptic neuron. Many of them are not fully understood [4]. But for the purposes of this article, it suffices to say that this leads (or does not lead) to the generation of an impulse in this neuron and further transmission of information.
Receptors
Receptor is a special molecule that is located on the surface of the neuron membrane and reacts by changing the spatial configuration to the addition of a certain substance (neurotransmitter) to it [9]. The substance that activates this receptor is called its ligand .
The feature of receptors is their selectivity. For example, the serotonin receptor does not respond to dopamine and vice versa. This allows you to distinguish between the signals given by different neurons. Especially taking into account the fact that the neurotransmitter can freely “flow” from the synaptic cleft and spread over the adjacent area[4]. nine0007
nine0007
Receptors are (and this is important for us) not only postsynaptic (i.e. located on the membrane of the "second" neuron), but also presynaptic (i.e. located on the membrane of the first neuron). Why are they there? To organize feedback: the neuron itself reacts to its own neurotransmitter. This is a pretty cool feature, especially considering that the receptors of one ligand can affect the release of another (an example will be below) [4].
Neurotransmitters
Neurotransmitters (or neurotransmitters ) are the very substances by which the signal is transmitted in the chemical synapse. There are quite a few of them, the most famous and interesting to us are serotonin, norepinephrine and dopamine.
An example of an [incomplete] listing of neurotransmitters, divided into groups according to their chemical structure, is presented below [4]:
Psychonauts have a cool saying on this topic: if there is a receptor, there will be a ligand. nine0007
nine0007
What we need to remember about neurotransmitters is that they are produced by the presynaptic neuron and transmit a message to the postsynaptic neuron by binding to its receptors.
Agonists, antagonists and inverse agonists
According to the principle of action on receptors, substances can be divided into three (well, four, but those that do not affect the receptor are not of interest to us, so three) groups: agonists , antagonists and inverse agonists [4].
Agonists is the easiest thing to understand. They bind to the receptor and cause its response. In the text above, when it was said that the neurotransmitter binds to the postsynaptic receptor, it (the neurotransmitter) acted as an agonist.
The antagonist is a ligand that binds to and "deactivates" the receptor. While the receptor is occupied by the antagonist, the agonist cannot "cling" to it, and, accordingly, the message cannot get through.
An inverse agonist is a substance that, by binding to a receptor, produces physiological effects opposite to those produced by an agonist. Also, it's not hard to understand.
And then there are partial agonists and antagonists - they act in the same way as full ones, but weaker.
An important consequence: if we apply an antagonist of a certain receptor, and then increase the amount of the neurotransmitter, then in some cases the antagonism will be "cancelled". And vice versa, if we simply reduce the amount of the neurotransmitter, the effect will be the same as if we applied the appropriate antagonist. We will need this corollary later in the discussion of atypical antipsychotics. nine0007
Neurotransmitter reuptake
But that is not all. For some neurotransmitters, the mechanism of the so-called. reuptake [10]: once in the synaptic cleft and transmitting a message, the neurotransmitter returns back to the vesicle with the help of a special transporter molecule. This was done to save the neurotransmitter and control its amount in the synaptic cleft.
This was done to save the neurotransmitter and control its amount in the synaptic cleft.
Each neurotransmitter (to be more precise, each of those subject to reuptake) has its own transporter molecule: SERT for serotonin, DAT for dopamine, etc. nine0007
It should be noted the selectivity of the reuptake mechanism - the transporter cannot capture a “foreign molecule”.
Allosteric modulation
The essence of this phenomenon can be expressed as follows [4]: some receptors are able to interact not only with one ligand, but with two substances. In this case, the first is "basic" and works without the second, and the second affects the receptor only in conjunction with the first, reducing ( allosteric inhibition ) or increasing ( allosteric activation ) the intensity of the response.
- It should be noted that the work of the brain described here is greatly simplified, and in fact everything is much more complicated there.
Mental illnesses and their treatment
How psychopharma works
So, we have considered the main stages of the transmission of a nerve impulse from one neuron to another. Now we can discuss the mechanisms of work of psychopharmacological drugs in a general way [4]. nine0007
What can we do with these drugs? Lots of things, actually. Firstly, the drug can act as a direct agonist (dopaminomimetics) or an antagonist (neuroleptics) of the corresponding receptors.
Secondly, it can act as an inhibitor (SSRIs - a class of antidepressants) or an inverter (amphetamine) of the neurotransmitter reuptake process. In the first case, the neurotransmitter will not be removed from the synaptic cleft, in the second case, the reuptake system “turns 180 degrees” and, instead of dragging the neurotransmitter into the vesicles, begins to release it from them into the synaptic cleft. nine0007
Thirdly, it is possible to influence the system of secondary messengers (according to some data, some normotimics work in this way) by changing the cascade of events in the receiving (postsynaptic) neuron.
Fourthly, it is possible to act on the presynaptic receptor, block it, thus turning off the negative feedback mechanism and increasing the amount of the neurotransmitter in the synaptic cleft (some antidepressants and atypical antipsychotics).
Fifth, it is possible to activate the mechanism of allosteric modulation and enhance or weaken the action of the corresponding neurotransmitters. nine0007
And, finally, sixthly, it is possible to influence the expression of genes. Drugs in which this mechanism would be the main one are unknown to us, but, for example, valproates have this property [11].
Schizophrenia
The “default mental illness” in our psychiatric hospitals (take this opportunity to say hello to L.S. and other psychiatrists who are used to putting it on everyone without understanding), so famous that it has become a curse word (remember all these “he’s crazy” and “ you're crazy"). nine0007
A small, fairly plausible video that allows you to look inside schizophrenic perception:
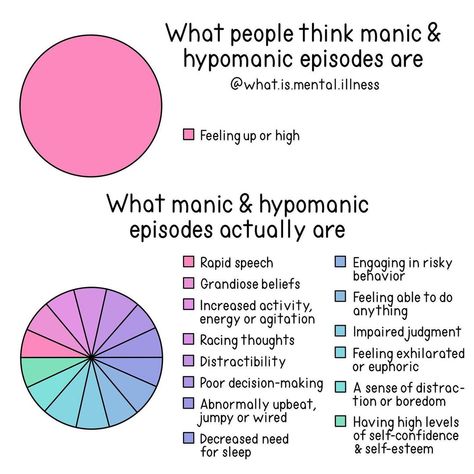
In short, it manifests itself in two aspects: in negative and productive symptoms [12]. Productive symptomatology is when the psyche begins to produce what it normally should not produce: hallucinations, ideas of relationships, delusions.
Productive symptomatology is when the psyche begins to produce what it normally should not produce: hallucinations, ideas of relationships, delusions.
Examples? The author, for example, often sees non-existent cats. One patient I worked with felt like he was being "fucked for his dreams." Another believed that only the intrigues of the FSB prevented him from receiving an award for breaking the RSA algorithm. The third thought that the treacherous Chinese were slipping heroin into his marijuana to make him an addict. There is a popular case in the literature in which the patient believed that the dogs were looking at him and laughing at his frail body [13]. nine0007
Negative symptomatology is the opposite, when the psyche does not produce what it should. These include volitional decline (the patient cannot force himself to bathe or even eat), emotional flattening (the patient is unable to express emotions, seems insensitive) and intellectual decline.
Let's make a reservation that here by schizophrenia we mean not only, in fact, F20, but the whole spectrum of schizophrenia-like disorders F2X, perhaps, with the exception of schizoaffective (F25), which in some cases is closer to affective disorders (more on them later). nine0007
nine0007
There are quite a few hypotheses regarding the causes of schizophrenia [4,13]: psychoanalysts' "misguided trajectory of life", violations of the rules of abstraction and context (Bateson's theory), the invasion of Grof's transpersonal entities, disruption of dopaminergic transmission, etc.
In the framework of this article, we will consider the latter, since most drugs widely used in psychiatry affect the dopamine system (well, the serotonin system, but these are already subtleties). nine0007
So, in our brain there is such a thing as black body (Substantia nigra) - an accumulation of bodies of dopamine (that is, those that use dopamine as a means of transmitting information) neurons. From there, the axons of these neurons stretch to various areas of the brain, forming the so-called. dopaminergic pathways: mesocortical , mesolimbic , nigrostrial and tuberoinfundibular [4].
Consider their connection with manifestations of schizophrenia. The most interesting for us will be mesolimbic dopamine pathway connecting the tegmental area of the midbrain and the substantia nigra with various structures of the limbic system. Indirectly, it is also projected to the frontal cortex and hypothalamus. Normally, it plays an important role in the process of learning, reward, memory and emotion mechanisms [4].
The most interesting for us will be mesolimbic dopamine pathway connecting the tegmental area of the midbrain and the substantia nigra with various structures of the limbic system. Indirectly, it is also projected to the frontal cortex and hypothalamus. Normally, it plays an important role in the process of learning, reward, memory and emotion mechanisms [4].
Drugs that increase dopaminergic transmission in this pathway have been found to lead to psychotic symptoms (delusions, hallucinations - positive symptoms). On the other hand, drugs that lower dopamine levels in these areas have the ability to relieve such symptoms. An interesting fact: psychosis caused by the systematic abuse of stimulants - cocaine, amphetamines, etc., can be practically indistinguishable from schizophrenic psychosis in external manifestations [4]. nine0007
In addition, an association has been established between excessive transmission activity in this pathway and aggression in psychotic patients.
The mesocortical pathway is also very interesting to us, but for a different reason. It connects the ventral tegmentum of the midbrain with the frontal lobe of the cerebral cortex, mainly with the prefrontal cortex, and plays an important role in the processes of motivation, planning, and emotional response.
It has been established[4] that a decrease in the level of dopamine in this pathway is associated with the negative symptoms of schizophrenia: flattening of affect, impoverishment of emotional life, speech disorders and, probably, a decrease in intelligence. nine0007
And here's an interesting thing: in schizophrenia, in one pathway (mesolimbic), you need to reduce the level of dopamine, and in the other (mesocortical) - increase [4]. It must be said that modern psychopharmacology has partly solved this problem, then we will explain exactly how, but for now we will briefly consider the remaining two ways in the context of the question of interest to us.
The nigrostriatal pathway , which connects the substantia nigra and ventral tegmentum with the striatum, is involved in the initiation of motor activity, being part of a system called the basal ganglia motor loop. We are interested in the fact that dopamine deficiency in this pathway causes akathisia (restlessness) - a condition in which the patient experiences a compulsive (irresistible) need to move: he is literally unable to sit still[4]. Here is a video of the process:
https://www.youtube.com/watch?v=svoDpICEnsg
By itself, akathisia is not a symptom of schizophrenia, but it is associated with it - this is a fairly common side effect of anti-schizophrenic drugs ( I think the logic is clear: drugs are trying to reduce the level of dopamine in the mesolimbic pathway, but it also decreases in the nigrostriatal one). And there is such a thing as dyskinesia induced by neuroleptics - pathological movements of arbitrary muscle groups ("twisting"). And it is on YouTube:
And it is on YouTube:
And, finally, tuberoinfundibular pathway , formed by dopaminergic neurons of the arcuate nucleus of the mediobasal hypothalamus, projecting their axons into the median eminence. The dopamine secreted by them regulates the secretion of prolactin by the anterior pituitary [4]. We are interested in it insofar as many antipsychotic drugs lead to an increase in the level of prolactin, which is especially critical for women: their menstrual cycle goes astray and lactation may begin. nine0007
Antipsychotics (aka antipsychotics)
Generally speaking, this class of drugs is not only used to treat schizophrenia, but is associated with it. Historically, they are divided into two large groups - typical and atypical .
typical antipsychotics include such well-known drugs as haloperidol, chlorpromazine (Aminazine), trifluoperazine (Triftazine). Strictly speaking, neuroleptics, ie. drugs that cause neurolepsy - a state of a significant decrease in motor and mental activity, emotional flatness and indifference to what is happening, are only drugs in this group. The newer, atypical, "neuroleptics" are more properly called antipsychotics, but no one really bothers with this.
The newer, atypical, "neuroleptics" are more properly called antipsychotics, but no one really bothers with this.
The main mechanism of action of these drugs is to block postsynaptic dopamine receptors (mainly D2) [4,14]. From the mechanism of schizophrenia described above, it is clear what the therapeutic effect of these drugs is based on: they block receptors in the mesolimbic pathway (remember that receptor antagonists make these very receptors inactive, as a result of which the signal ceases to be transmitted from one neuron to another). nine0007
The only bad thing is that typical neuroleptics are not limited to mesolimbic pathways, also blocking D2 receptors in the mesocortical pathway, which leads to worsening of negative symptoms (remember that they appear precisely because of insufficient dopaminergic transmission in this pathway) [four]. That is, in fact, they work according to the well-known principle among the people: "we treat one thing, we cripple another. "
"
And if we take into account that the combination of productive and negative symptoms in schizophrenia is not at all uncommon, then everything becomes quite sad (negative symptoms, other things being equal, mean a less favorable long-term prognosis than productive ones). To reduce the undesirable consequences of taking antipsychotics, special preparations are used - correctors , the most famous of which is trihexyphenidyl ("Cyclodol").
In general, in our experience, it is difficult to distinguish between a person who has severe negative symptoms of schizophrenia and a patient drugged with antipsychotics.
Differences are not visible not only visually or during communication, but also in tests. It often happens that replacing a typical neuroleptic with a more modern drug greatly reduces the severity of intellectual deficit, volitional decline, emotional flattening and other negative symptoms. nine0007
But that's not all bad that can be said about these drugs.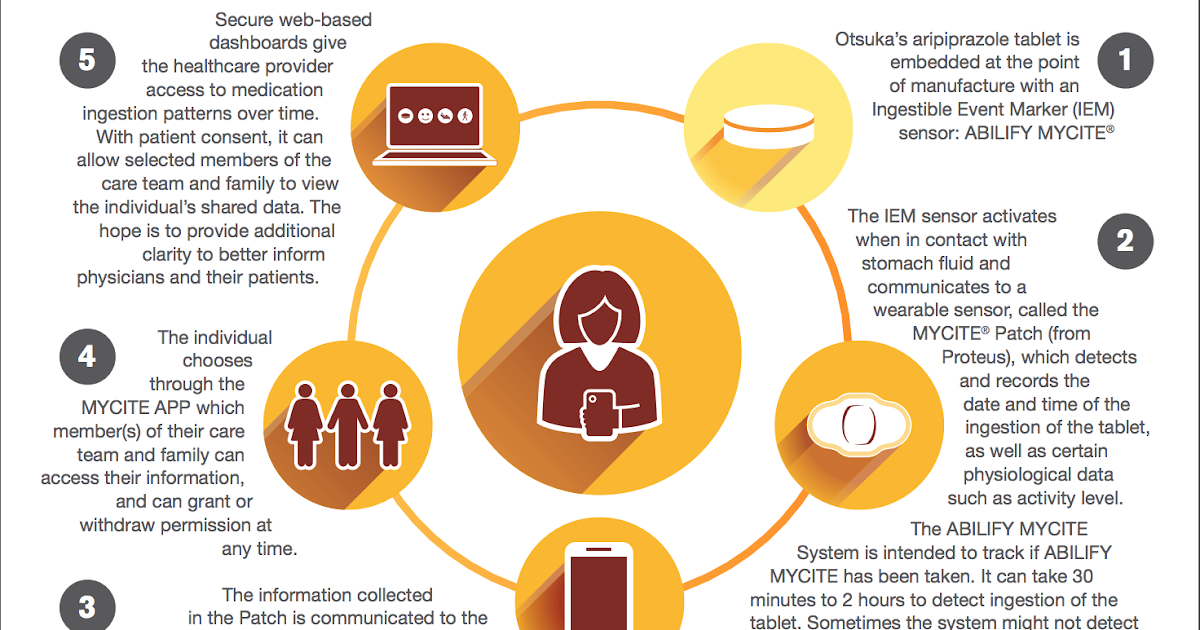 Since they block D2 receptors absolutely everywhere, incl. in the nigrostrial pathway, they are the cause of such phenomena as akathisia ("restlessness") and dyskinesia ("twisting") [4].
Since they block D2 receptors absolutely everywhere, incl. in the nigrostrial pathway, they are the cause of such phenomena as akathisia ("restlessness") and dyskinesia ("twisting") [4].
And almost all drugs in this group lead to an increase in prolactin levels with all the ensuing (gee-gee, Beavis, pun) consequences.
These are the pills. At the same time, they are the most popular drugs of choice in psychiatric hospitals, at least in our region. Why? There are two reasons for this. nine0007
The first is quite rational: they perfectly allow to remove the state of acute psychosis[4]. If the patient is aggressive, in agitation, sees voices and hears aliens, runs after household members with an ax, etc., then an injection of life-giving haloperidol (or another drug of this group) can bring him into a state suitable, if not for conversation, then for transportation to the appropriate institution, much faster than more modern preparations. Not always, but that's the trend.
The second reason is a banal lack of funding. It often happens that a psychiatrist would be happy to prescribe some kind of aripiprazole, but it simply is not and will never be in the medicine cabinet because it is quite expensive.
Well, and I must say separately: if your psychiatrist has prescribed you a typical antipsychotic, do not rush to quarter it - sometimes they can really be the best choice. But consideration of such subtleties is already beyond the scope of this article.
Now let's talk about atypical antipsychotics (they are simply “ atypicals ”). Typical representatives of the group of atypical antipsychotics are quetiapine, olanzapine, risperidone, etc.
we need to block it only in one, in one - on the contrary, strengthen it, and the other two, if possible, do not touch. nine0007
Atypicals partially solve this problem[4]. From the point of view of pharmacology, they are antagonists of dopamine and serotonin receptors. As you can see, serotonin was added here, which was not in the description of schizophrenia itself (the reader with an asterisk knows about the role of 5-HT-2A receptors, but we decided not to complicate the picture).
As you can see, serotonin was added here, which was not in the description of schizophrenia itself (the reader with an asterisk knows about the role of 5-HT-2A receptors, but we decided not to complicate the picture).
The fact is that serotonin inhibits the release of dopamine, and the nature of this inhibition differs in all four dopamine pathways. Thus, by affecting serotonin, we can influence dopamine (indirectly). Let's try to figure it out. nine0007
Dopamine (that is, those that transmit information through dopamine) have a postsynaptic serotonin receptor, by activating which we can reduce the release of dopamine. In fact, it works like a switch: by stimulating the serotonin receptor (5-HT-2A), we inhibit the release of dopamine into the synaptic cleft. The reverse is also true: by blocking the serotonin receptor (5-HT-2A), we increase the release of dopamine. Those. counteract its antagonism.
It is important to understand here: atypicals simultaneously act in opposite directions: they reduce dopaminergic transmission due to antagonism of D2-dopamine receptors and increase it due to blocking of 5-HT-2A-serotonin receptors. Which action "wins" depends on the number of 5-HT-2ª receptors [4]. nine0007
Which action "wins" depends on the number of 5-HT-2ª receptors [4]. nine0007
Fortunately, the mesolimbic pathway is the least of them. This means that D2 receptor antagonism “wins” there and dopaminergic transmission is reduced, which is what we want, since this leads to a decrease in productive symptoms.
In the nigrostriatal pathway (which is responsible for dyskinesia and akathisia), additional dopamine release by blocking 5-HT-2A serotonin receptors compensates for the effect of atypicals as D2 receptor agonists.
B mesocortical pathway serotonin receptors are located at a higher density than dopamine receptors, so atypicals here work to increase dopaminergic transmission, which is what we need, since this allows us to deal with negative symptoms. Again, nature itself seems to play along with us.
An interesting fact about atypicals is that in fact the victory of one action over another (increasing dopaminergic transmission over its decrease or vice versa) depends not only on which pathway is in question, but also on the dose of the drug. Therefore, they (atypicals) have a very strong dependence of the clinical effect on the dose of the drug [4]. nine0007
Therefore, they (atypicals) have a very strong dependence of the clinical effect on the dose of the drug [4]. nine0007
Finally, the third generation of atypicals, aripiprazole and bifenprux, are the most interesting.
They are interesting in that they simultaneously have the properties of partial agonists and antagonists of dopamine (D2) and serotonin (5-HT-1A) receptors [15]. Which properties of the drug will appear depends on the dose and on the presence and amount of the neurotransmitter.
This makes the pharmacological profile of these drugs unique: if dopamine is low, they work as an activator of dopaminergic transmission, and if it is high, then as its inhibitor. nine0007
Personal experience. Instead of a conclusion
A review of antipsychotics would be incomplete without a description of personal experience with this group of drugs. Next, I will briefly describe how it was. Please do not take it as a guide to action, since the selection of psychopharma is an individual process and should be carried out under the guidance of a specialist.
Quetiapine - taken for the relief of manic episodes. He copes with this task perfectly, but he didn’t like it on an ongoing basis: emotional flattening is too pronounced and I really want to sleep. I use it from time to time in order to escape from reality during emotionally significant events that I am unable to endure and as a safety net when taking% ROSCOMNADZOR%. nine0007
Chlorpromazine (Aminazin) - I didn't like it at all. It doesn’t completely eliminate mental disorders, it sedates very strongly, shortens associative chains, and makes it difficult to think. It doesn't help, it only makes it worse.
Amisulpride . The effect is dose dependent. At 400 mg / day. sensations - as if you live in a basin of glycerin: movements are slow, you physically feel air resistance, reality is clouded. It is impossible to think, to express emotions too. At 50 mg - you are activated, it is easy to think, violations of thinking are much less pronounced. nine0007
nine0007
Aripiprazole . Now I am writing this article on it (in combination with some other drugs), which I could not even dream of before.
- The article turned out to be quite large anyway, so we will talk about the treatment of affective disorders (depression, mania), OCD, GAD and other things in the next article, if this topic is of interest to the community at all.
Literature
1. Douglas Fields. Glial cells (neuroglia).
scisne.net/a-1101
2. Konorev, M. R. A course of lectures on pharmacology: a manual for students of 3 and 4 courses pharmacist. fak. honey. universities: in 2 volumes. Vol. 1: / M. R. Konorev, I. I. Krapivko, D. A. Rozhdestvensky; Ministry of Health of the Republic of Belarus, Vitebsk State. honey. un-t. - Vitebsk: [VSMU], 2013. - 243 p.Yo
3. F. Huho. Neurochemistry. Fundamentals and principles. Moscow: Mir, 1990. ISBN 5-003-001030-0
4. Stahl, S. M. Essential psychopharmacology: neuroscientific basis and practical application / Stephen M. Stahl; with illustrations by Nancy Muntner.—2nd ed. p.; cm. ISBN 0-521-64154-3 (hardback)—ISBN 0-521-64615-4 (pbk.)
Stahl; with illustrations by Nancy Muntner.—2nd ed. p.; cm. ISBN 0-521-64154-3 (hardback)—ISBN 0-521-64615-4 (pbk.)
5. Neurochemistry: a textbook for biological and medical universities. Ed. acad. RAMS I.P. Ashmarin and prof. P.V. Stukalova. M.: Ed. Institute of Biomedical Chemistry RAMS, 1996. ISBN: 5-0-02-2
6. Shostak V.I., Lytaev S.A., Berezantseva M.S. Psychophysiology. Tutorial. - St. Petersburg, 2007. ISBN 978-5-93979-186-1
7. Eccles D.K. Physiology of synapses. — M.: Mir, 1966. — 397 p.
8. Anne E. West, Wen G. Chen, Matthew B. Dalva, Ricardo E. Dolmetsch, Jon M. Kornhauser, Adam J. Shaywitz, Mari A. Takasu, Xu Tao, and Michael E. Greenberg. Calcium regulation of neuronal gene expression PNAS 2001 98 (20) 11024-11031; doi:10.1073/pnas.191352298
9. John E. Hall PhD. Guyton and Hall Textbook of Medical Physiology, 13e (Guyton Physiology). ISBN-13: 978-1455770052
10. Neurotransmitter Transporters in the Central Nervous System J. Masson, C.