Symptoms and signs of ocd
Obsessive-compulsive disorder (OCD) - Symptoms and causes
Overview
Obsessive-compulsive disorder (OCD) features a pattern of unwanted thoughts and fears (obsessions) that lead you to do repetitive behaviors (compulsions). These obsessions and compulsions interfere with daily activities and cause significant distress.
You may try to ignore or stop your obsessions, but that only increases your distress and anxiety. Ultimately, you feel driven to perform compulsive acts to try to ease your stress. Despite efforts to ignore or get rid of bothersome thoughts or urges, they keep coming back. This leads to more ritualistic behavior — the vicious cycle of OCD.
OCD often centers around certain themes — for example, an excessive fear of getting contaminated by germs. To ease your contamination fears, you may compulsively wash your hands until they're sore and chapped.
If you have OCD, you may be ashamed and embarrassed about the condition, but treatment can be effective.
Symptoms
Obsessive-compulsive disorder usually includes both obsessions and compulsions. But it's also possible to have only obsession symptoms or only compulsion symptoms. You may or may not realize that your obsessions and compulsions are excessive or unreasonable, but they take up a great deal of time and interfere with your daily routine and social, school or work functioning.
Obsession symptoms
OCD obsessions are repeated, persistent and unwanted thoughts, urges or images that are intrusive and cause distress or anxiety. You might try to ignore them or get rid of them by performing a compulsive behavior or ritual. These obsessions typically intrude when you're trying to think of or do other things.
Obsessions often have themes to them, such as:
- Fear of contamination or dirt
- Doubting and having difficulty tolerating uncertainty
- Needing things orderly and symmetrical
- Aggressive or horrific thoughts about losing control and harming yourself or others
- Unwanted thoughts, including aggression, or sexual or religious subjects
Examples of obsession signs and symptoms include:
- Fear of being contaminated by touching objects others have touched
- Doubts that you've locked the door or turned off the stove
- Intense stress when objects aren't orderly or facing a certain way
- Images of driving your car into a crowd of people
- Thoughts about shouting obscenities or acting inappropriately in public
- Unpleasant sexual images
- Avoidance of situations that can trigger obsessions, such as shaking hands
Compulsion symptoms
OCD compulsions are repetitive behaviors that you feel driven to perform.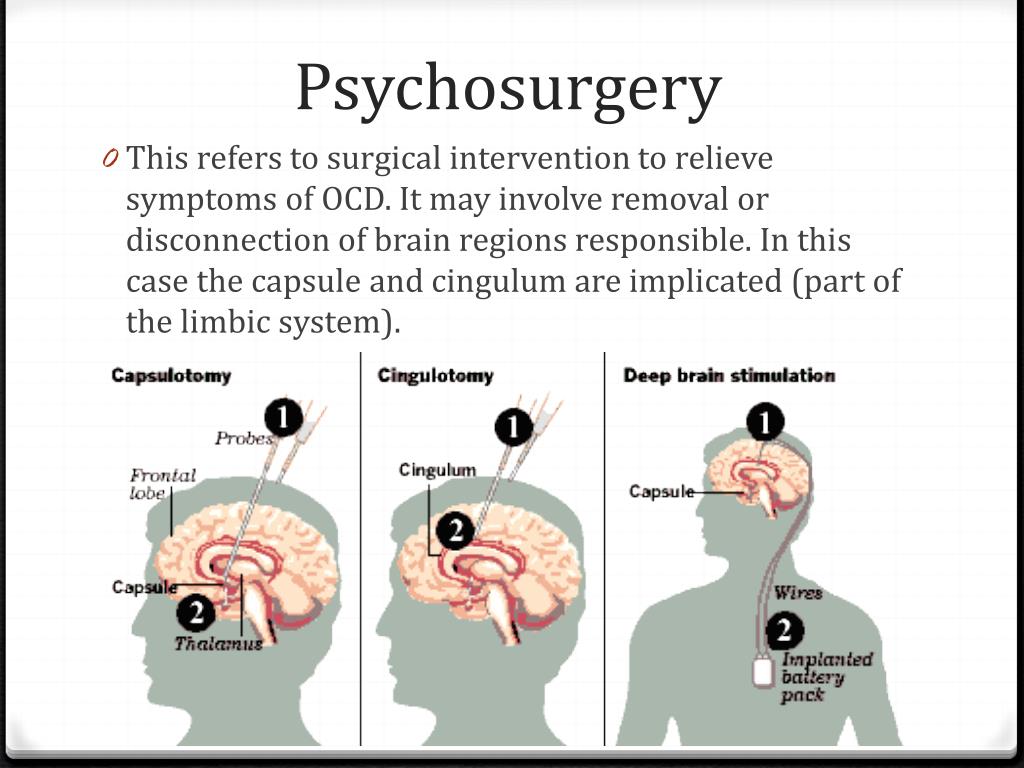 These repetitive behaviors or mental acts are meant to reduce anxiety related to your obsessions or prevent something bad from happening. However, engaging in the compulsions brings no pleasure and may offer only a temporary relief from anxiety.
These repetitive behaviors or mental acts are meant to reduce anxiety related to your obsessions or prevent something bad from happening. However, engaging in the compulsions brings no pleasure and may offer only a temporary relief from anxiety.
You may make up rules or rituals to follow that help control your anxiety when you're having obsessive thoughts. These compulsions are excessive and often are not realistically related to the problem they're intended to fix.
As with obsessions, compulsions typically have themes, such as:
- Washing and cleaning
- Checking
- Counting
- Orderliness
- Following a strict routine
- Demanding reassurance
Examples of compulsion signs and symptoms include:
- Hand-washing until your skin becomes raw
- Checking doors repeatedly to make sure they're locked
- Checking the stove repeatedly to make sure it's off
- Counting in certain patterns
- Silently repeating a prayer, word or phrase
- Arranging your canned goods to face the same way
Severity varies
OCD usually begins in the teen or young adult years, but it can start in childhood. Symptoms usually begin gradually and tend to vary in severity throughout life. The types of obsessions and compulsions you experience can also change over time. Symptoms generally worsen when you experience greater stress. OCD, usually considered a lifelong disorder, can have mild to moderate symptoms or be so severe and time-consuming that it becomes disabling.
Symptoms usually begin gradually and tend to vary in severity throughout life. The types of obsessions and compulsions you experience can also change over time. Symptoms generally worsen when you experience greater stress. OCD, usually considered a lifelong disorder, can have mild to moderate symptoms or be so severe and time-consuming that it becomes disabling.
When to see a doctor
There's a difference between being a perfectionist — someone who requires flawless results or performance, for example — and having OCD. OCD thoughts aren't simply excessive worries about real problems in your life or liking to have things clean or arranged in a specific way.
If your obsessions and compulsions are affecting your quality of life, see your doctor or mental health professional.
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Causes
The cause of obsessive-compulsive disorder isn't fully understood. Main theories include:
- Biology.
 OCD may be a result of changes in your body's own natural chemistry or brain functions.
OCD may be a result of changes in your body's own natural chemistry or brain functions. - Genetics. OCD may have a genetic component, but specific genes have yet to be identified.
- Learning. Obsessive fears and compulsive behaviors can be learned from watching family members or gradually learned over time.
Risk factors
Factors that may increase the risk of developing or triggering obsessive-compulsive disorder include:
- Family history. Having parents or other family members with the disorder can increase your risk of developing OCD.
- Stressful life events. If you've experienced traumatic or stressful events, your risk may increase. This reaction may, for some reason, trigger the intrusive thoughts, rituals and emotional distress characteristic of OCD.

- Other mental health disorders. OCD may be related to other mental health disorders, such as anxiety disorders, depression, substance abuse or tic disorders.
Complications
Problems resulting from obsessive-compulsive disorder may include, among others:
- Excessive time spent engaging in ritualistic behaviors
- Health issues, such as contact dermatitis from frequent hand-washing
- Difficulty attending work, school or social activities
- Troubled relationships
- Overall poor quality of life
- Suicidal thoughts and behavior
Prevention
There's no sure way to prevent obsessive-compulsive disorder. However, getting treatment as soon as possible may help prevent OCD from worsening and disrupting activities and your daily routine.
By Mayo Clinic Staff
Related
Associated Procedures
NIMH » Obsessive-Compulsive Disorder
Overview
Obsessive-compulsive disorder (OCD) is a common, chronic, and long-lasting disorder in which a person has uncontrollable, reoccurring thoughts ("obsessions") and/or behaviors ("compulsions") that he or she feels the urge to repeat over and over.
Signs and Symptoms
People with OCD may have symptoms of obsessions, compulsions, or both. These symptoms can interfere with all aspects of life, such as work, school, and personal relationships.
Obsessions are repeated thoughts, urges, or mental images that cause anxiety. Common symptoms include:
- Fear of germs or contamination
- Unwanted forbidden or taboo thoughts involving sex, religion, or harm
- Aggressive thoughts towards others or self
- Having things symmetrical or in a perfect order
Compulsions are repetitive behaviors that a person with OCD feels the urge to do in response to an obsessive thought. Common compulsions include:
- Excessive cleaning and/or handwashing
- Ordering and arranging things in a particular, precise way
- Repeatedly checking on things, such as repeatedly checking to see if the door is locked or that the oven is off
- Compulsive counting
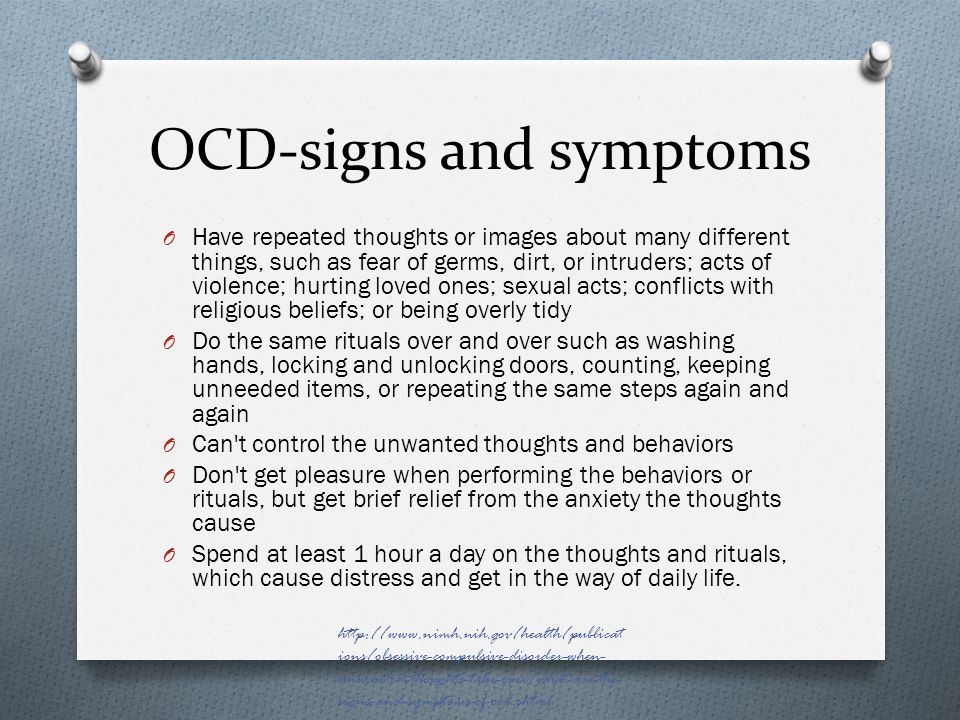
Not all rituals or habits are compulsions.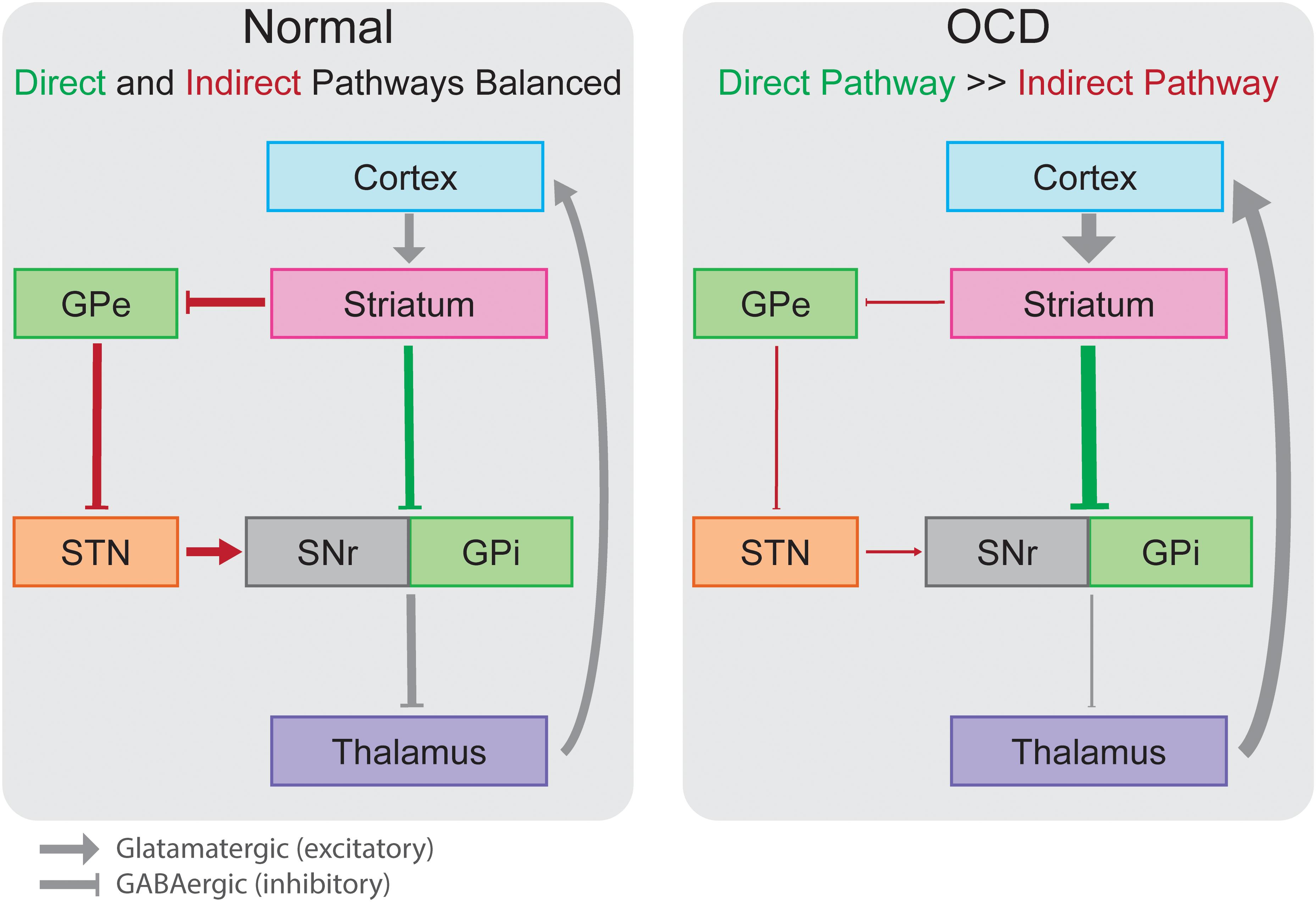 Everyone double checks things sometimes. But a person with OCD generally:
Everyone double checks things sometimes. But a person with OCD generally:
- Can't control his or her thoughts or behaviors, even when those thoughts or behaviors are recognized as excessive
- Spends at least 1 hour a day on these thoughts or behaviors
- Doesn’t get pleasure when performing the behaviors or rituals, but may feel brief relief from the anxiety the thoughts cause
- Experiences significant problems in their daily life due to these thoughts or behaviors
Some individuals with OCD also have a tic disorder. Motor tics are sudden, brief, repetitive movements, such as eye blinking and other eye movements, facial grimacing, shoulder shrugging, and head or shoulder jerking. Common vocal tics include repetitive throat-clearing, sniffing, or grunting sounds.
Symptoms may come and go, ease over time, or worsen. People with OCD may try to help themselves by avoiding situations that trigger their obsessions, or they may use alcohol or drugs to calm themselves. Although most adults with OCD recognize that what they are doing doesn’t make sense, some adults and most children may not realize that their behavior is out of the ordinary. Parents or teachers typically recognize OCD symptoms in children.
Although most adults with OCD recognize that what they are doing doesn’t make sense, some adults and most children may not realize that their behavior is out of the ordinary. Parents or teachers typically recognize OCD symptoms in children.
If you think you have OCD, talk to your health care provider about your symptoms. If left untreated, OCD can interfere in all aspects of life.
Risk Factors
OCD is a common disorder that affects adults, adolescents, and children all over the world. Most people are diagnosed by about age 19, typically with an earlier age of onset in boys than in girls, but onset after age 35 does happen. For statistics on OCD in adults, please see the NIMH Obsessive-Compulsive Disorder webpage.
The causes of OCD are unknown, but risk factors include:
Genetics
Twin and family studies have shown that people with first-degree relatives (such as a parent, sibling, or child) who have OCD are at a higher risk for developing OCD themselves. The risk is higher if the first-degree relative developed OCD as a child or teen. Ongoing research continues to explore the connection between genetics and OCD and may help improve OCD diagnosis and treatment.
The risk is higher if the first-degree relative developed OCD as a child or teen. Ongoing research continues to explore the connection between genetics and OCD and may help improve OCD diagnosis and treatment.
Brain Structure and Functioning
Imaging studies have shown differences in the frontal cortex and subcortical structures of the brain in patients with OCD. There appears to be a connection between the OCD symptoms and abnormalities in certain areas of the brain, but that connection is not clear. Research is still underway. Understanding the causes will help determine specific, personalized treatments to treat OCD.
Environment
An association between childhood trauma and obsessive-compulsive symptoms has been reported in some studies. More research is needed to understand this relationship better.
In some cases, children may develop OCD or OCD symptoms following a streptococcal infection—this is called Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS). For more information, please read NIMH's fact sheet on PANDAS.
For more information, please read NIMH's fact sheet on PANDAS.
Treatments and Therapies
OCD is typically treated with medication, psychotherapy, or a combination of the two. Although most patients with OCD respond to treatment, some patients continue to experience symptoms.
Sometimes people with OCD also have other mental disorders, such as anxiety, depression, and body dysmorphic disorder, a disorder in which someone mistakenly believes that a part of their body is abnormal. It is important to consider these other disorders when making decisions about treatment.
Medication
Serotonin reuptake inhibitors (SRIs), which include selective serotonin reuptake inhibitors (SSRIs) are used to help reduce OCD symptoms.
SRIs often require higher daily doses in the treatment of OCD than of depression and may take 8 to 12 weeks to start working, but some patients experience more rapid improvement.
If symptoms do not improve with these types of medications, research shows that some patients may respond well to an antipsychotic medication. Although research shows that an antipsychotic medication may help manage symptoms for people who have both OCD and a tic disorder, research on the effectiveness of antipsychotics to treat OCD is mixed.
Although research shows that an antipsychotic medication may help manage symptoms for people who have both OCD and a tic disorder, research on the effectiveness of antipsychotics to treat OCD is mixed.
If you are prescribed a medication, be sure you:
- Talk with your health care provider or a pharmacist to make sure you understand the risks and benefits of the medications you're taking.
- Do not stop taking a medication without talking to your health care provider first. Suddenly stopping a medication may lead to "rebound" or worsening of OCD symptoms. Other uncomfortable or potentially dangerous withdrawal effects are also possible.
- Report any concerns about side effects to your health care provider right away. You may need a change in the dose or a different medication.
- Report serious side effects to the U.S. Food and Drug Administration (FDA) MedWatch Adverse Event Reporting program online or by phone at 1-800-332-1088. You or your health care provider may send a report.

Other medications have been used to treat OCD, but more research is needed to show the benefit of these options. For basic information about these medications, you can visit the NIMH Mental Health Medications webpage. For the most up-to-date information on medications, side effects, and warnings, visit the FDA website.
Psychotherapy
Psychotherapy can be an effective treatment for adults and children with OCD. Research shows that certain types of psychotherapy, including cognitive behavior therapy (CBT) and other related therapies (e.g., habit reversal training) can be as effective as medication for many individuals. Research also shows that a type of CBT called Exposure and Response Prevention (EX/RP)—spending time in the very situation that triggers compulsions (e.g. touching dirty objects) but then being prevented from undertaking the usual resulting compulsion (e.g. handwashing)—is effective in reducing compulsive behaviors in OCD, even in people who did not respond well to SRI medication.
As with most mental disorders, treatment is usually personalized and might begin with either medication or psychotherapy, or with a combination of both. For many patients, EX/RP is the add-on treatment of choice when SRIs or SSRIs medication does not effectively treat OCD symptoms or vice versa for individuals who begin treatment with psychotherapy.
Other Treatment Options
In 2018, the FDA approved Transcranial Magnetic Stimulation (TMS) as an adjunct in the treatment of OCD in adults.
NIMH is supporting research into other new treatment approaches for people whose OCD does not respond well to the usual therapies. These new approaches include combination and add-on (augmentation) treatments, as well as novel techniques such as deep brain stimulation. You can learn more about brain stimulation therapies on the NIMH website.
Finding Treatment
For general information on mental health and to locate treatment services in your area, call the Substance Abuse and Mental Health Services Administration (SAMHSA) Treatment Referral Helpline at 1-800-662-HELP (4357). SAMHSA also has a Behavioral Health Treatment Locator on its website that can be searched by location. You can also visit the NIMH’s Help for Mental Illnesses page for more information and resources.
SAMHSA also has a Behavioral Health Treatment Locator on its website that can be searched by location. You can also visit the NIMH’s Help for Mental Illnesses page for more information and resources.
Join a Study
Clinical trials are research studies that look at new ways to prevent, detect, or treat diseases and conditions. The goal of clinical trials is to determine if a new test or treatment works and is safe. Although individuals may benefit from being part of a clinical trial, participants should be aware that the primary purpose of a clinical trial is to gain new scientific knowledge so that others may be better helped in the future.
Researchers at NIMH and around the country conduct many studies with patients and healthy volunteers. We have new and better treatment options today because of what clinical trials uncovered years ago. Be part of tomorrow’s medical breakthroughs. Talk to your health care provider about clinical trials, their benefits and risks, and whether one is right for you.
To learn more or find a study, visit:
- NIMH’s Clinical Trials webpage: Information about participating in clinical trials
- Clinicaltrials.gov: Current Studies on OCD: List of clinical trials funded by the National Institutes of Health (NIH) being conducted across the country
Learn More
Free Booklets and Brochures
- Obsessive-Compulsive Disorder: When Unwanted Thoughts Take Over: This brochure provides information on OCD including signs and symptoms, causes, and treatment options such as psychotherapy and medication. Also available en español.
Federal Resources
- Obsessive-Compulsive Disorder (MedlinePlus – also en español)
Research and Statistics
- Journal Articles: This webpage provides information on references and abstracts from MEDLINE/PubMed (National Library of Medicine).
- OCD Statistics: Adults: This webpage lists information on the prevalence of OCD among adults.
Last Reviewed: September 2022
Unless otherwise specified, NIMH information and publications are in the public domain and available for use free of charge. Citation of NIMH is appreciated. Please see our Citing NIMH Information and Publications page for more information.
Obsessive Compulsive Disorder Treatment
Great Thought is an obsessive compulsive disorder treatment program. We will relieve you of obsessive thoughts, movements and rituals. Let's get back to life!
Symptoms of obsessive-compulsive disorder
- Frightening images and drives
- Compulsive acts (rituals)
- Intrusive check of one's own actions
- Fear of trouble, pollution or infection
- Inexplicable desire to count something
- Excessive organization and pedantry
- Perfectionism in relationships, work and even leisure
- "Stuck", "looping" on one's thoughts
You feel that over time your mood becomes worse: apathy, depression, obsessions increase, and rituals begin to fill all your free time or harm your physical health.
You may have had more than one meeting with psychologists, psychotherapists and psychiatrists. You are not given the "scary" psychiatric diagnoses of Schizophrenia or Bipolar Disorder, but are prescribed medication and psychotherapy nonetheless. However, such treatment cannot be called effective - the symptoms persist and only aggressive pharmacotherapy temporarily reduces anxiety.
What is obsessive-compulsive disorder?
Obsessive-compulsive disorder is a syndrome characterized by the presence of obsessive thoughts (obsessions) to which a person reacts with certain actions (compulsions). The causes of the disorder are rarely superficial. The syndrome is also accompanied by the development of obsessive memories and various pathological phobias. May be chronic, episodic or progressive.
Obsession - obsessive thought, persistent desire for something, uncontrollable and accompanied by anxiety and intense anxiety. In an attempt to cope with such thoughts, a person resorts to committing compulsions.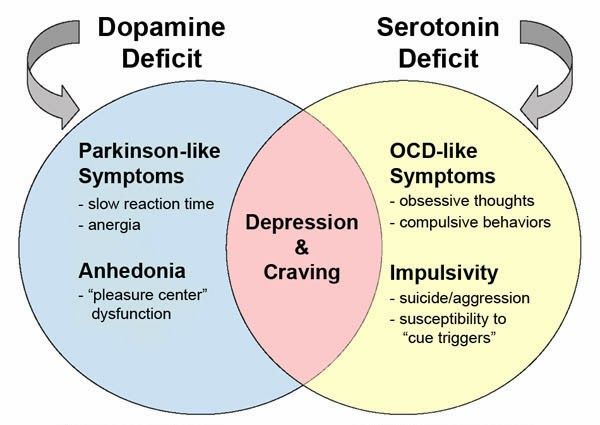
Compulsion - an irresistible need to perform certain actions (rituals), which can be assessed by the person himself as irrational or meaningless, and the internal need to perform them is forced and is the result of obsessive ideas.
Common examples of OCD manifestations
- An exaggerated sense of danger. Fear of the materiality of thoughts:
- "now I will lose control and hurt my loved ones"
- "something terrible is about to happen, I can feel it"
- "I shouldn't think like that, all this will come true because of me"
- Pathological fear of pollution. Thirst for Purity
- Excessive perfectionism, exaggerated responsibility - "everything must be done perfectly", "everything depends on me, mistakes are unacceptable"
How does this painful algorithm work?
Most people have unwanted or obsessive thoughts quite often, but all sufferers of the disorder greatly exaggerate their importance. Fear of one's own thoughts leads to attempts to neutralize the negative feelings that arise from obsessions, for example by avoiding thought-provoking situations or by engaging in "rituals" of excessive self-cleansing or prayer.
Fear of one's own thoughts leads to attempts to neutralize the negative feelings that arise from obsessions, for example by avoiding thought-provoking situations or by engaging in "rituals" of excessive self-cleansing or prayer.
As we noted earlier, repetitive avoidance behavior can "get stuck", "loop", that is, have a tendency to repeat. The cause of obsessive-compulsive disorder is the interpretation of intrusive thoughts as catastrophic and true.
If you periodically experience over the years:
- Constant or fluctuating anxiety
- The need to perform certain ritualized actions
- A persistent decline in the quality of life due to the need to avoid certain thoughts and actions, places and events
And you are also persecuted:
- Significant problems in studies and career
- Failure to establish a serious relationship
- Constant criticism and pressure from relatives
- Many senseless activities
- Excessive involvement in computer games and the Internet, alcohol
- Loneliness and isolation
We strongly recommend that you do not delay seeking help and that you complete a remedial program.
Consultations and psychotherapeutic sessions according to the program are held several times a week, until the relief of severe symptoms, then the frequency of meetings with specialists is reduced to 2–3 per month. Count on the fact that in the end we will deal with your problem together.
Treatment of obsessive-compulsive disorder in Neuro-Psi
Every day, the specialists of the NEURO-PSI clinic analyze the world practice in the field of psychiatry and psychotherapy. The goal is the impartial selection and implementation of those methods of treatment and psychological assistance, the effectiveness of which has been convincingly proven in independent studies.
We are guided by the principles of evidence-based medicine and use as a basic method of treatment a psychotherapeutic paradigm, the effectiveness of which has been widely recognized by the professional community.
1. What is the essence of the obsessive-compulsive disorder treatment program
Since obsessive thoughts, rituals and conditions are only symptoms of mental dysfunction, the root cause must be treated in order to achieve a stable result. A comprehensive work is carried out with the client, taking into account the main factors that create well-being.
A comprehensive work is carried out with the client, taking into account the main factors that create well-being.
The main emphasis is on teaching the client how to properly respond to his thoughts, emotions, inner feelings and interpretation of external events.
All types of psychotherapeutic and drug treatments serve the same goal: to achieve the best result in the shortest possible time. At the same time, by coordinating the efforts of specialists in various fields, the most complete coverage of all types of mental illnesses, disorders and disorders is possible.
2. What treatments are used
- Priority:
- Cognitive-Behavioral Therapy.
- Schema Therapy.
- Reality Therapy.
- Choice Theory.
- Rational pharmacotherapy.
- Psychopharmacotherapy (if indicated)
- Biofeedback Therapy
- Rational psychocorrection of stress
- Jacobson progressive muscle relaxation.
- Traditional and modern gymnastic systems, relaxation techniques.
- Breathing techniques .
- Stress exposure.
- Self-control training.
- Jacobson progressive muscle relaxation.
- Lifestyle modification
- Work with bad habits.
- Diet correction.
- Professional and social adaptation.
3. How is the treatment under the program
Each treatment program at the NEURO-PSI clinic consists of four stages:
- diagnostics,
- work with disease symptoms,
- work with the causes of the disease,
- consolidation of the achieved results.
Work efficiency is increased by dividing the treatment process into a predetermined number of sessions, at convenient times and without hospitalization. This means that each program is adapted to the problem that the client has addressed.
The program method of treatment is predictable, time-limited, productive, and, most importantly, understandable for the client.
Of course, the treatment takes place in a comfortable mode without interruption from work, study or family. Specialists of various profiles will work with you (team method). This is necessary to minimize the risk of diagnostic errors that could lead to the adoption of a suboptimal treatment plan.
Improvements in well-being and mood (healing) occur in stages: after the decrease in emotional problems, bodily symptoms decrease. Working with the causes (etiology) of obsessive-compulsive disorder helps to avoid relapses in the future.
4. What are the results and prognosis?
Upon completion of the program, you get rid of obsessive thoughts and rituals, fear of pollution, unmotivated fears, panic attacks and multiple vegetative symptoms (sudden jumps in blood pressure, heart palpitations, dizziness, nausea).
According to statistics, the effectiveness of the methods used approaches 100% if all recommendations of specialists are followed.
Skills you acquire during the program:
- self-control and self-regulation
- constructive analysis of the state of the body
- understanding one's own mental and emotional sphere
- ability to control one's attention
- ability to act consciously in stressful situations
Significantly improves the emotional and physical condition, gains self-confidence, in the future. Emotional stress is removed, sleep and appetite are restored. The efficiency is greatly increased.
5. Where to start taking the course
In order for you to know the treatment plan, we recommend signing up for a diagnostic (first) consultation.
Obsessive-Compulsive Disorder (OCD) - key facts in English
Obsessive-Compulsive Disorder (OCD)
See our disclaimer that applies to all translations available on this site.
What is obsessive-compulsive disorder?
At times, we can all get hung up on some things, but if:
You obsessively have terrible thoughts even when you try to get rid of them,
You have to count or touch things over and over again, or repeat actions, such as washing your hands,
maybe you have obsessive-compulsive disorder (OCD).
Who gets OCD?
About 1 in 50 people will experience OCD at some point in their lives. Equally, it can be men and women. In the UK, their number is about 1 million people. OCD usually begins in adolescence or early adulthood. Symptoms of OCD may get worse or worse over time, but often people don't seek help for many years.
OCD usually begins in adolescence or early adulthood. Symptoms of OCD may get worse or worse over time, but often people don't seek help for many years.
What are the signs and symptoms of obsessive-compulsive disorder?
- Recurring thoughts that make you feel anxious - "obsessions" or "obsessions". It can be unpleasant words or phrases, mental pictures or doubts.
- The things you do over and over again that help you feel less anxious are 'compulsions'. You can try to correct or "neutralize" thoughts by counting over and over again, saying a special word, or performing certain rituals.
What are the causes of OCD?
Many factors can play a role in the occurrence of OCD. One or more of the following could explain why you or someone you know has OCD.
- In some cases, OCD is inherited, so sometimes the disorder can run in the family.
- Stressful life events cause OCD in about a third of cases.
- Life changes in which you have to take on more responsibility, such as puberty, the birth of a child, or a new job.
- If you have OCD and it lasts for some time, you may develop an imbalance of serotonin (also known as 5HT), a brain neurotransmitter.
- You are a neat, pedantic, methodical person - but you take it too far.
- If you have extremely high standards of morality and responsibility, you may feel especially bad about having unpleasant thoughts. To the point where you start to be wary and keep a close eye on them, which makes them even more likely to appear.
How to help yourself
- If you regularly force yourself to think the thoughts that are bothering you, you will be able to control them better. You can write them down - on a recorder or on paper, and then listen to or reread. You should do this regularly, for about half an hour every day. At the same time, try to resist compulsive behavior.
- Do not use alcohol to control your anxiety.
- If your intrusive thoughts are about your faith or religion, discuss them with your religious leader to help you understand if OCD is a problem.
- Try using a self-help book.
Professional help Various types of psychotherapy
Exposure and response prevention
Helps to stop the mutual reinforcing of compulsive behavior and anxiety.
We know that if you stay in a stressful situation long enough, you will gradually get used to it and the anxiety will go away. In this way, you gradually face the situation that you fear (exposure), but stop yourself from doing your usual compulsive rituals of checking or clearing (avoiding a response) and wait for your anxiety to go away.
Cognitive therapy
Instead of getting rid of your thoughts, cognitive therapy helps you change how you react to them. It specifically targets unrealistic self-critical thoughts. Useful if you have intrusive thoughts but are not performing any rituals or activities to reduce your anxiety. Can be used with Exposure and Response Prevention.
Antidepressant treatment
Even if you are not depressed, SSRI (Selective Serotonin Reuptake Inhibitor) antidepressants can help. They may be used alone or with cognitive behavioral therapy for moderate to severe OCD. If the medicine doesn't help at all after three months of taking it, you can change it to another SSRI antidepressant or a medicine called Clomipramine (Anafranil).
They may be used alone or with cognitive behavioral therapy for moderate to severe OCD. If the medicine doesn't help at all after three months of taking it, you can change it to another SSRI antidepressant or a medicine called Clomipramine (Anafranil).
How effective is the treatment?
Exposure and prevention of response
About three out of four people who completed this psychotherapy did well, but one in four will return symptoms and require additional treatment. Approximately one in four people refuse to try this type of cognitive-behavioral therapy or do not complete it - they find it too hard for them.
Medications
About six people in 10 feel better with medication and their symptoms lessen by about half. Medications do help prevent OCD from returning for as long as they are taken, even years later. Unfortunately, about half of those who stop taking the drug return symptoms within a few months afterward. This is less likely when drug treatment is combined with cognitive behavioral therapy.
Which approach is best for me?
Mild OCD
Exposure and response prevention can be done without professional help. This method is effective and has no side effects, but you will feel more anxious for a while. You must be motivated and ready for hard work. Cognitive therapy and drug treatment are equally effective.
Moderate or severe OCD
- Initially, you can choose either CBT (up to 10 hours in contact with a therapist) or medication (within 12 weeks). If you do not get better, you should try both treatments together.
- If you have severe OCD, it is best to use medication and CBT together from the start.
- Taking medication alone will help you if you don't feel able to face the anxiety that Exposure and response prevention will cause, but the chances of OCD coming back are higher - about one in two compared to one in four with psychotherapy treatment. The medicine must be taken for about a year and is obviously not ideal during pregnancy or breastfeeding.