Moderate autism spectrum disorder
The Difference Between Moderate To Severe Autism
Posted on March 20, 2019 by SDCAadmin
Every person with autism will face social, communication, and behavior challenges, and they will need ongoing assistance and support.
However, autism is a developmental disorder that’s a spectrum, meaning children with autism may experience mild, moderate, or severe symptoms and impairments.
As the parent of a child with autism, identifying the differences between moderate to severe autism assists you in understanding your child and helping him or her achieve a quality of life and the highest possible level of independence possible.
Here are some of the differences in moderate to severe autism.
Behavior For Moderate To Severe Autism
Communication and intellectual challenges cause children with moderate autism to exhibit many unusual behaviors. They may flap their arms, rock, hit, bite, scratch, or become obsessed with an object when they’re bored, upset, happy, frustrated, overwhelmed, or unable to share their thoughts or feelings.
While these and other behaviors are a way of communicating, they can be scary and dangerous to family members, onlookers, and the child. Certain behaviors will remain quirks for life, but therapy, communication strategies, and other tools can help children learn to cope and communicate better so they remain safe.
The behaviors of children with severe autism are similar to those exhibited by children with moderate autism to a greater degree. Typically difficult to manage, these behaviors can include a variety of self-soothing, stimulating, or communicative behaviors like rocking, flapping and jumping as well as aggression toward others and self-abuse.
Beneficial therapy can help children with severe autism cope and communicate, but they may continue to exhibit these behaviors on some level throughout their lives.
Communication & Language For Moderate To Severe Autism
Communication and language capabilities are generally limited in children with moderate autism. They may acquire language skills later than normal and speak below their age level. In some cases, children with moderate autism are nonverbal and unable to speak words.
They may acquire language skills later than normal and speak below their age level. In some cases, children with moderate autism are nonverbal and unable to speak words.
Depending on intellectual abilities, children with moderate autism may learn to communicate through pictures, typing, or via other communication devices.
Many children with severe autism have very limited communication and language abilities. If they can speak, they repeat words and phrases they hear others say or say only a few words that do not fit the context.
Despite serious limitations, though, children with severe autism can communicate through sounds, groans, and behaviors. Parents use observation, interaction, and speech therapy to understand their child and discover ways to improve communication and language.
Children with moderate autism may or may not interact with peers. They generally struggle to make eye contact, interpret body language and emotions, and understand figures of speech, and they may simply walk away from conversations that don’t involve their favorite topics or interests.
However, children with moderate autism can play near or with peers unless their repetitive behaviors like arm flapping or rocking, limited speech capabilities, and aggression scare peers who don’t understand the disorder.
The limitations of children with severe autism greatly reduce social interactions. These children often cannot control their repetitive behaviors and may express their discomfort, thoughts, and emotions through violent meltdowns that hinder community involvement.
Limited speech also hinders conversations, an essential part of socializing, unless they learn to communicate via alternative methods.
Sensory Concerns For Moderate To Severe Autism
Sensitivity to textures, tastes, sights, sounds, and aromas can be a challenge for children with moderate autism.
When faced with overwhelming sensory input, they may meltdown and display behaviors like rocking, moaning, or aggression. Parents must know their child’s sensory concerns and take steps to create a non-threatening environment with limitations on sensory triggers. They can turn down the lights, serve preferred foods, and reduce household noise.
They can turn down the lights, serve preferred foods, and reduce household noise.
Additionally, they can use behavior therapy and other strategies to help their child develop coping skills and become more comfortable in less-than-ideal environments.
Because of sensory concerns, children with severe autism must often live in a very structured and predictable environment. They may be unable to tolerate loud noises, certain aromas, or any touching.
To prevent meltdowns or self-injurious behavior, parents must create a non-threatening environment and limit their child’s exposure to sensory triggers. In cases, therapy can help children with severe autism manage sensory concerns to a degree over time.
Education For Moderate To Severe Autism
Although children with moderate autism may have some intellectual or learning disabilities, they can often attend school. Because a mainstream classroom is usually overwhelming, children with moderate autism may enroll in an autism support classroom in a traditional school setting or attend a school specifically designed for students with autism.
Special accommodations in the Individualized Education Program (IEP) provide beneficial supports that help the children maximize strengths, improve weaknesses, and gain valuable academic, social, emotional, and life skills.
Some children with severe autism have intellectual challenges that make learning difficult. A traditional school setting is impossible to navigate and even an autistic support classroom may be overwhelming.
However, small, therapeutic settings in a traditional or autism specific school can provide an environment that helps children with severe autism learn and grow. Here, educators follow a specialized and individualized plan for each child. With these supports, children with severe autism learn valuable skills.
Level Of Care For Moderate To Severe Autism
With behavior and occupational therapies, children with moderate autism can achieve a level of independence.
Often, they can learn to dress, bathe, and feed themselves, and they may even be able to hold a job eventually. Intellectual and other challenges may hinder complete independence, though. They will always need someone to ensure their safety, provide for daily needs, and manage their treatment plan, including therapy and medical care.
Intellectual and other challenges may hinder complete independence, though. They will always need someone to ensure their safety, provide for daily needs, and manage their treatment plan, including therapy and medical care.
Children with severe autism typically need 24/7 care and supervision. Thanks to therapy, they can learn basic self-care. However, they will need assistance performing many activities of daily living, managing health care, and functioning in daily life.
Parents must carefully choose caregivers and respite workers who understand autism and can meet their child’s specific needs in a safe and effective manner.
Children with moderate to severe autism face similar yet different challenges.
Understand what type of autism your child has as you create a plan that nurtures and equips your loved one to reach his or her full potential and live a life of safety, comfort, and dignity.
You may also be interested in these related articles:
- Benefits of Choosing an Autism School
- Resource Guide For Autism Information And Education
- Teaching Students With All Levels of Autism
« Oldest
Newest »
Autism spectrum disorder - Symptoms and causes
Overview
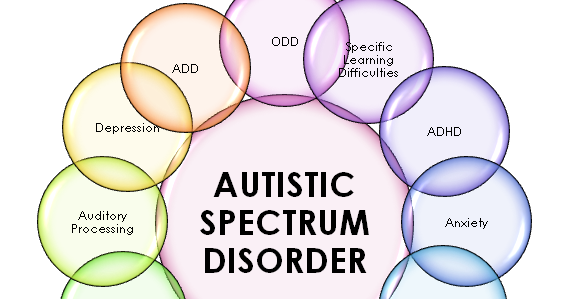
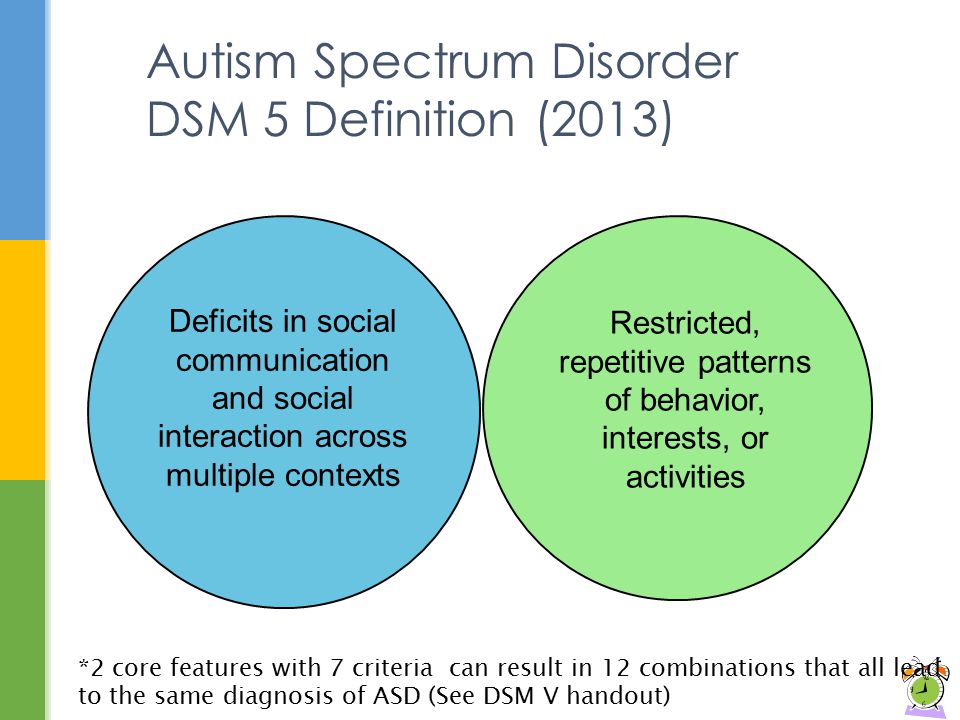
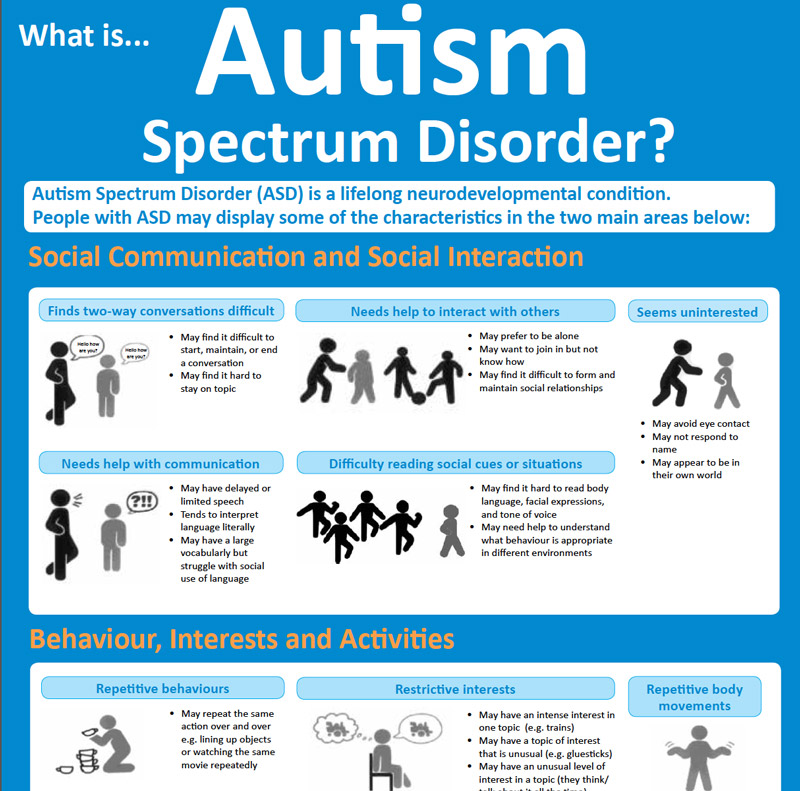
Autism spectrum disorder is a condition related to brain development that impacts how a person perceives and socializes with others, causing problems in social interaction and communication. The disorder also includes limited and repetitive patterns of behavior. The term "spectrum" in autism spectrum disorder refers to the wide range of symptoms and severity.
The disorder also includes limited and repetitive patterns of behavior. The term "spectrum" in autism spectrum disorder refers to the wide range of symptoms and severity.
Autism spectrum disorder includes conditions that were previously considered separate — autism, Asperger's syndrome, childhood disintegrative disorder and an unspecified form of pervasive developmental disorder. Some people still use the term "Asperger's syndrome," which is generally thought to be at the mild end of autism spectrum disorder.
Autism spectrum disorder begins in early childhood and eventually causes problems functioning in society — socially, in school and at work, for example. Often children show symptoms of autism within the first year. A small number of children appear to develop normally in the first year, and then go through a period of regression between 18 and 24 months of age when they develop autism symptoms.
While there is no cure for autism spectrum disorder, intensive, early treatment can make a big difference in the lives of many children.
Products & Services
Symptoms
Some children show signs of autism spectrum disorder in early infancy, such as reduced eye contact, lack of response to their name or indifference to caregivers. Other children may develop normally for the first few months or years of life, but then suddenly become withdrawn or aggressive or lose language skills they've already acquired. Signs usually are seen by age 2 years.
Each child with autism spectrum disorder is likely to have a unique pattern of behavior and level of severity — from low functioning to high functioning.
Some children with autism spectrum disorder have difficulty learning, and some have signs of lower than normal intelligence. Other children with the disorder have normal to high intelligence — they learn quickly, yet have trouble communicating and applying what they know in everyday life and adjusting to social situations.
Because of the unique mixture of symptoms in each child, severity can sometimes be difficult to determine. It's generally based on the level of impairments and how they impact the ability to function.
It's generally based on the level of impairments and how they impact the ability to function.
Below are some common signs shown by people who have autism spectrum disorder.
Social communication and interaction
A child or adult with autism spectrum disorder may have problems with social interaction and communication skills, including any of these signs:
- Fails to respond to his or her name or appears not to hear you at times
- Resists cuddling and holding, and seems to prefer playing alone, retreating into his or her own world
- Has poor eye contact and lacks facial expression
- Doesn't speak or has delayed speech, or loses previous ability to say words or sentences
- Can't start a conversation or keep one going, or only starts one to make requests or label items
- Speaks with an abnormal tone or rhythm and may use a singsong voice or robot-like speech
- Repeats words or phrases verbatim, but doesn't understand how to use them
- Doesn't appear to understand simple questions or directions
- Doesn't express emotions or feelings and appears unaware of others' feelings
- Doesn't point at or bring objects to share interest
- Inappropriately approaches a social interaction by being passive, aggressive or disruptive
- Has difficulty recognizing nonverbal cues, such as interpreting other people's facial expressions, body postures or tone of voice
Patterns of behavior
A child or adult with autism spectrum disorder may have limited, repetitive patterns of behavior, interests or activities, including any of these signs:
- Performs repetitive movements, such as rocking, spinning or hand flapping
- Performs activities that could cause self-harm, such as biting or head-banging
- Develops specific routines or rituals and becomes disturbed at the slightest change
- Has problems with coordination or has odd movement patterns, such as clumsiness or walking on toes, and has odd, stiff or exaggerated body language
- Is fascinated by details of an object, such as the spinning wheels of a toy car, but doesn't understand the overall purpose or function of the object
- Is unusually sensitive to light, sound or touch, yet may be indifferent to pain or temperature
- Doesn't engage in imitative or make-believe play
- Fixates on an object or activity with abnormal intensity or focus
- Has specific food preferences, such as eating only a few foods, or refusing foods with a certain texture
As they mature, some children with autism spectrum disorder become more engaged with others and show fewer disturbances in behavior. Some, usually those with the least severe problems, eventually may lead normal or near-normal lives. Others, however, continue to have difficulty with language or social skills, and the teen years can bring worse behavioral and emotional problems.
Some, usually those with the least severe problems, eventually may lead normal or near-normal lives. Others, however, continue to have difficulty with language or social skills, and the teen years can bring worse behavioral and emotional problems.
When to see a doctor
Babies develop at their own pace, and many don't follow exact timelines found in some parenting books. But children with autism spectrum disorder usually show some signs of delayed development before age 2 years.
If you're concerned about your child's development or you suspect that your child may have autism spectrum disorder, discuss your concerns with your doctor. The symptoms associated with the disorder can also be linked with other developmental disorders.
Signs of autism spectrum disorder often appear early in development when there are obvious delays in language skills and social interactions. Your doctor may recommend developmental tests to identify if your child has delays in cognitive, language and social skills, if your child:
- Doesn't respond with a smile or happy expression by 6 months
- Doesn't mimic sounds or facial expressions by 9 months
- Doesn't babble or coo by 12 months
- Doesn't gesture — such as point or wave — by 14 months
- Doesn't say single words by 16 months
- Doesn't play "make-believe" or pretend by 18 months
- Doesn't say two-word phrases by 24 months
- Loses language skills or social skills at any age
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Causes
Autism spectrum disorder has no single known cause. Given the complexity of the disorder, and the fact that symptoms and severity vary, there are probably many causes. Both genetics and environment may play a role.
Both genetics and environment may play a role.
- Genetics. Several different genes appear to be involved in autism spectrum disorder. For some children, autism spectrum disorder can be associated with a genetic disorder, such as Rett syndrome or fragile X syndrome. For other children, genetic changes (mutations) may increase the risk of autism spectrum disorder. Still other genes may affect brain development or the way that brain cells communicate, or they may determine the severity of symptoms. Some genetic mutations seem to be inherited, while others occur spontaneously.
- Environmental factors. Researchers are currently exploring whether factors such as viral infections, medications or complications during pregnancy, or air pollutants play a role in triggering autism spectrum disorder.
No link between vaccines and autism spectrum disorder
One of the greatest controversies in autism spectrum disorder centers on whether a link exists between the disorder and childhood vaccines. Despite extensive research, no reliable study has shown a link between autism spectrum disorder and any vaccines. In fact, the original study that ignited the debate years ago has been retracted due to poor design and questionable research methods.
Despite extensive research, no reliable study has shown a link between autism spectrum disorder and any vaccines. In fact, the original study that ignited the debate years ago has been retracted due to poor design and questionable research methods.
Avoiding childhood vaccinations can place your child and others in danger of catching and spreading serious diseases, including whooping cough (pertussis), measles or mumps.
Risk factors
The number of children diagnosed with autism spectrum disorder is rising. It's not clear whether this is due to better detection and reporting or a real increase in the number of cases, or both.
Autism spectrum disorder affects children of all races and nationalities, but certain factors increase a child's risk. These may include:
- Your child's sex. Boys are about four times more likely to develop autism spectrum disorder than girls are.
- Family history. Families who have one child with autism spectrum disorder have an increased risk of having another child with the disorder.
 It's also not uncommon for parents or relatives of a child with autism spectrum disorder to have minor problems with social or communication skills themselves or to engage in certain behaviors typical of the disorder.
It's also not uncommon for parents or relatives of a child with autism spectrum disorder to have minor problems with social or communication skills themselves or to engage in certain behaviors typical of the disorder. - Other disorders. Children with certain medical conditions have a higher than normal risk of autism spectrum disorder or autism-like symptoms. Examples include fragile X syndrome, an inherited disorder that causes intellectual problems; tuberous sclerosis, a condition in which benign tumors develop in the brain; and Rett syndrome, a genetic condition occurring almost exclusively in girls, which causes slowing of head growth, intellectual disability and loss of purposeful hand use.
- Extremely preterm babies. Babies born before 26 weeks of gestation may have a greater risk of autism spectrum disorder.
- Parents' ages. There may be a connection between children born to older parents and autism spectrum disorder, but more research is necessary to establish this link.
Complications
Problems with social interactions, communication and behavior can lead to:
- Problems in school and with successful learning
- Employment problems
- Inability to live independently
- Social isolation
- Stress within the family
- Victimization and being bullied
Prevention
There's no way to prevent autism spectrum disorder, but there are treatment options. Early diagnosis and intervention is most helpful and can improve behavior, skills and language development. However, intervention is helpful at any age. Though children usually don't outgrow autism spectrum disorder symptoms, they may learn to function well.
By Mayo Clinic Staff
Related
Associated Procedures
News from Mayo Clinic
Products & Services
Mental retardation and autism spectrum disorders
1000
children
suffer from
mental retardation
Up to 50% of people with autism spectrum disorders have an IQ level <70.
The first signs can be diagnosed up to 2 years.
Contribution of genetic factors ~ 80%.
20 out of every 10,000 children
have an autism spectrum disorder
.
The mortality rate in people under the age of 20 years with moderate and deep remaining is 3 times higher than the general population
Mild ca.
85%
patients
Moderate ca.
mental retardation, intellectual disability or brain function.
Autism Spectrum Disorders
include a wide range of symptoms, primarily impaired social interaction and social communication, combined with limited interests and rigid and repetitive behavior patterns. Mental development can range from profound retardation to a high level of intelligence.
What does genetic research give?
End of diagnostic search
Accurate molecular genetic analysis makes it possible not to conduct further diagnostic studies and to predict the patient's rehabilitation potential.
Selection of the correct treatment
Some diseases from this group have pathogenetic treatment, which allows to avoid or significantly slow down the progression of neurological symptoms.
Identification of the risk of transmission of the disease by inheritance
Thanks to genetic diagnosis, the risk of the disease in subsequent generations can be calculated and repeated cases in the family can be avoided.
About disease: causes
1. Environmental factors:
environmental exposure can cause profound changes in brain development, particularly in neuronal differentiation, synaptogenesis and axonal myelination
- tobacco smoking and exposure to alcohol or drugs during pregnancy
- Positive family history
- Congenital defects of the central nervous system
- intrauterine fetal injury (e.
 g. infectious or chemical)
g. infectious or chemical) - Prematurity (gestational age less than 35 weeks)
- Schizophrenia-like psychosis or mental illness in parents
- Use of sodium valproate during pregnancy
- asphyxia/birth trauma
- infections involving the central nervous system
2. Genetic factors:
include a wide range of symptoms, primarily impaired social interaction and social communication, combined with limited interests and rigid and repetitive behavior patterns.
Mental development in this case can vary from profound backwardness to a high level of intelligence.
- fragile X syndrome
- monogenic syndromes (eg, Angelman syndrome)
- chromosomal pathology (Down syndrome), microdeletions/microduplications
- monogenic diseases: tuberous sclerosis, neurofibromatosis, epileptic encephalopathies, muscular dystrophy, phenylketonuria, etc.
Mental Retardation and Autism Spectrum Disorders Panel
The study is performed using the high-throughput sequencing (NGS) method on the Illumina NextSeq 500 sequencer with an average coverage of at least 70-100x.
60 working days
Developmental delay, mental retardation and autism spectrum disorders panel
35000 RUB
Read more
Sign up for genetic testing To get the consultation
Test indication:
Combination of 3 key factors: low IQ, severe impairment of social communication and interaction, and onset in childhood.
In the case of autism spectrum disorders, about half of the parents notice unusual behavior of the child by the age of 18 months, and by 24 months already 80% of parents pay attention to deviations.
Because delaying treatment can affect long-term outcome, the child should be seen by a specialist immediately if any of the following are present:
- By 12 months of age, the baby is not babbling yet.
- Does not gesticulate by 12 months (does not point at objects, does not wave goodbye, etc.).
- Does not pronounce words by 16 months.
- Does not spontaneously speak two-word phrases by 24 months (except for echolalia).
- If any part of language or social skills is lost at any age.
When non-genetic causes of mental retardation and/or autism spectrum disorders are ruled out, the clinician should suspect a hereditary disorder.
As recommended by the American Academy of Neurology and Pediatric Neurology, the following tests are of diagnostic value for finding the causes of MR/ASD:
1
Genetic testing including high resolution karyotype, fragile X DNA analysis, chromosomal microarray analysis and high throughput exome sequencing
2
Selective metabolic tests in the combination of MR/RAS with cyclic vomiting, lethargy, early seizures
3
EEG with sleep recording against the background of sleep deprivation
Benefits of genetic disease research
Genetic testing can detect mutations in known genes associated with MR and/or ASD. Over time, already existing panels of genes are supplemented and expanded taking into account world databases.
Over time, already existing panels of genes are supplemented and expanded taking into account world databases.
Precise molecular genetic analysis makes it possible not to conduct further diagnostic studies and more accurately predict the course of the disease.
The procedure is strictly confidential.
The patient receives accurate results, on the basis of which specialists can prescribe the most effective treatment.
The analysis is quick and painless. All that is required for analysis is a blood sample. Specialists compare the results with a special panel that allows you to identify the possible cause of the disease.
Treatment
Mental retardation at present, for the most part, is not subject to medical correction, and is reduced to symptomatic and pathogenetic therapy, and for the most part to psychotherapeutic and pedagogical studies.
What else?
Molecular screening
More details
Screening for hereditary diseases of the unborn child
More details
Non-invasive paternity test
Read more
Miscarriage
Read more
Evaluation of the severity of autism spectrum disorders in children with general developmental disorders
Supervisor - Candidate of Medical Sciences, Associate Professor Karpyuk V. A.
A.
Grodno State Medical University, Belarus, 230009, Grodno, st. Gorkogo, 80
[email protected] - Bizyukevich Svetlana Viktorovna
CV. Autism spectrum disorders are a topical issue in child psychiatry. There is an acute problem of the earliest diagnosis of autism spectrum disorders, differential diagnosis, dynamic monitoring of children with autism spectrum disorders (ASD). The purpose of this article is to quantify the severity of autism spectrum disorders using the Childhood Autism Rating Scale (CARS). The results of applying the rating scale to assess the severity of ASD are presented. The scale showed high efficiency for quantitative assessment of the severity of autism spectrum disorders, which may allow individualizing the approach to the use of treatment and correction measures in children with ASD.
Keywords: autism spectrum disorders, diagnostics, rating scale, children.
ASSESSMENT OF THE SEVERITY OF AUTISM SPECTRUM DISORDERS IN CHILDREN WITH GENERAL DEVELOPMENTAL DISORDERS Biziukevich S.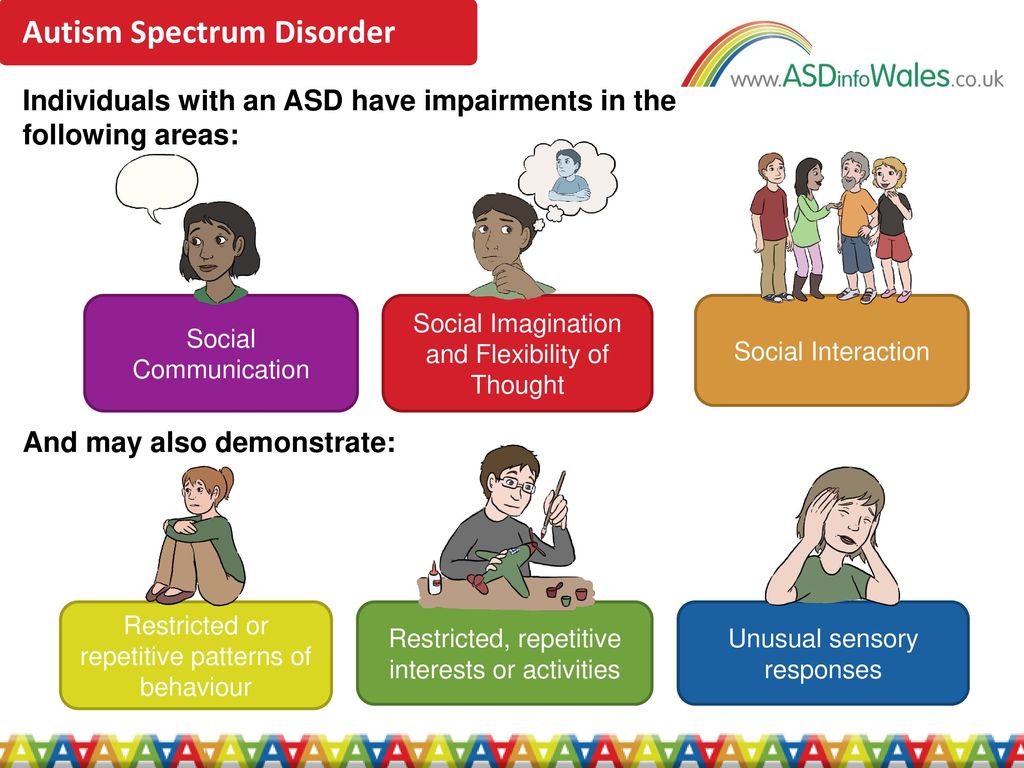 V.
V.
Scientific advisor — associate professor Karpiuk V.A., Candidate of Medicine
Grodno state medical university, Belarus, 230009, Grodno, Gorkogo St., 80.
Summary. Autism spectrum disorder is a challenging problem in pediatric psychiatry. An urgent task is the earliest diagnosis of autism spectrum disorders, differential diagnosis, dynamic monitoring of children with autism spectrum disorders (ASD). The aim of this study is to quantify the severity of autism spectrum disorders using the rating scale for the assessment of childhood autism (CARS). The results of the application of the rating scale to assess the severity of the ASD are presented. The scale revealed a high efficiency of the severity of autism spectrum disorders for the quantitative assessment, which make it possible to individualize the approach to the application of therapeutic and rehabilitative measures in children with ASD. Key words: autism spectrum disorders, diagnosis, rating scale, children.
Introduction. The problem of autism spectrum disorders is one of the most urgent in modern psychiatry, due to the steady increase in the number of children with autism spectrum disorders. Due to ambiguous approaches to the assessment of autistic disorders in different countries, the prevalence of autism is different and ranges from 4 to 26 cases per 10,000 children. The average male to female ratio in autism spectrum disorders (ASD) is 4.3:1 [3].
In the Republic of Belarus, from 2005 to 2012, the total number of children under the supervision of psychiatrists due to general developmental disorders, including autism spectrum disorders (ASD), increased by 2.8 times (from 251 to 699 cases) [1].
Autism Spectrum Disorders are developmental disorders characterized by marked and pervasive deficits in social interaction and communication, as well as limited interests and repetitive activities. The etiology and pathogenesis of ASD is not fully understood. Have
place various hypotheses on the etiology of autism spectrum disorders. It should be borne in mind that the existing hypotheses are not mutually exclusive and rather describe violations in different systems. In addition, the cause or causes of ASD may lie in the simultaneous influence of various etiological factors at a certain stage of intrauterine development [2].
It should be borne in mind that the existing hypotheses are not mutually exclusive and rather describe violations in different systems. In addition, the cause or causes of ASD may lie in the simultaneous influence of various etiological factors at a certain stage of intrauterine development [2].
Severe polymorphism
of clinical manifestations of autism spectrum disorders makes it difficult to accurately diagnose certain types of ASD. Based on diagnostic criteria,
presented in the International Classification of Diseases of the Tenth Revision (ICD-10): qualitative deviations in social
interactions, in terms of
sociability, as well as
limited stereotypical interests and behavioral reactions, the severity of signs of autism spectrum disorders is reduced to a subjective interpretation which often leads to overdiagnosis.
The subjectivism of such assessments is especially pronounced in the differential diagnosis of autism spectrum disorders with other mental disorders accompanied by hyperactivity, stereotypical
movements, limited interests, intellectual decline.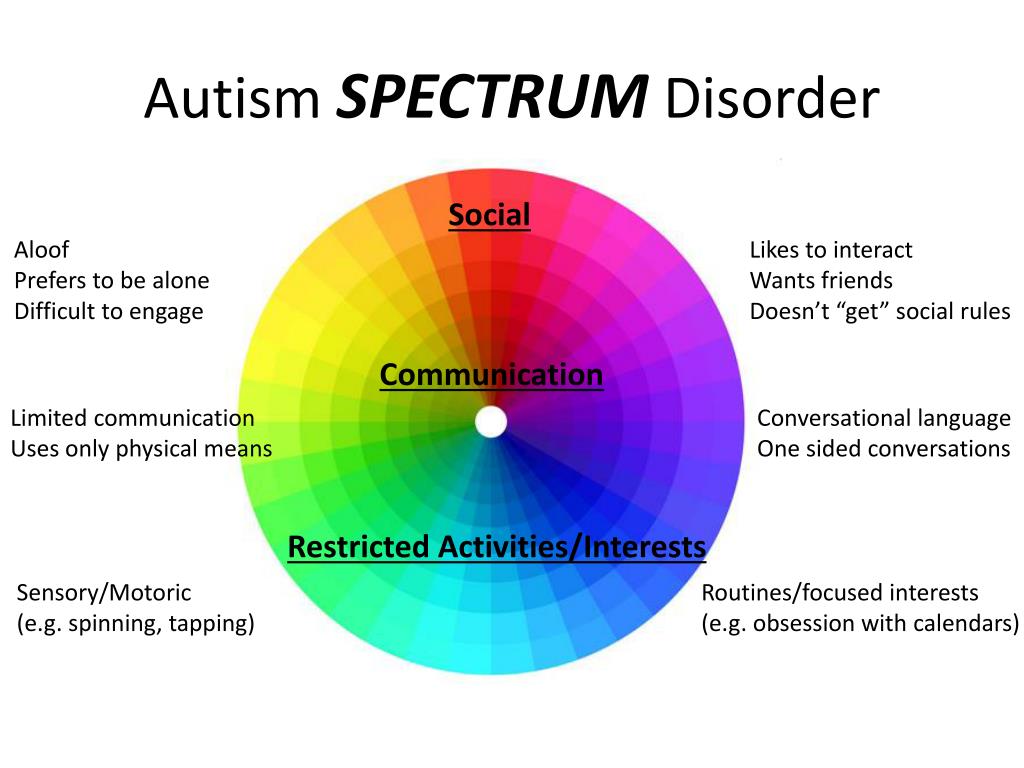
In Russian-speaking countries, including the Republic of Belarus, isolated cases of using diagnostic tools to quantify the severity of signs of autism spectrum disorders are described. This suggests that the diagnosis of the severity of signs of autism spectrum disorders is not accurate enough.
Thus, in order to develop individual programs of treatment and correction measures for children with autism spectrum disorders, it is important to establish the severity of autism spectrum disorders.
The purpose of this work is to assess the severity of autistic manifestations in children using the Childhood Autism Rating Scale (CARS).
Method. The study was carried out with the participation of 37 children who underwent inpatient examination and treatment in the children's department of the GOCC "Psychiatry-Narcology" for the period from January to December 2016. Of these, boys accounted for - 62.2% (23 people), girls - 37.8 % (14 people), aged 3 to 8 years. The study group included patients who, in accordance with the ICD-10 research diagnostic criteria, were diagnosed with "autism spectrum disorders".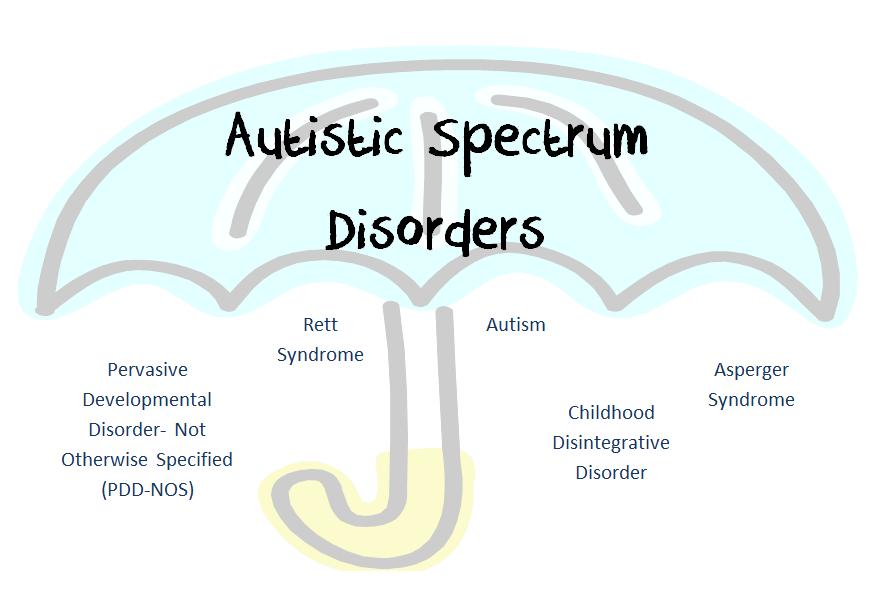
To quantify the severity of ASD, an adapted (translation and adaptation of Morozova T.Yu., Dovbnya S.V., 2011) rating scale for assessing childhood autism (CARS) was used. The scale is a standardized tool for assessing the severity of autistic behavior based on clinical observations of the child's behavior. It consists of 15 functional areas. The assessment of individual areas includes 4 degrees - from signs corresponding to age to signs that are very "deviating from the usual".
Results of the study and their discussion: The distribution of the examined children by gender and depending on the diagnosis is presented in Table 1.
Table 1. Distribution of children by sex and diagnosis
Diagnosis General Boys Girls
number (F 84.0) 16 11 5
Atypical autism (F 84.1) 4 3 1
Asperger's syndrome (B 84.5) 4 3 1
Rett syndrome (B 84.2) 1 0 1
90.3 6 3 3 Hyperactive disorder associated with mental retardation and stereotyped movements (B 84.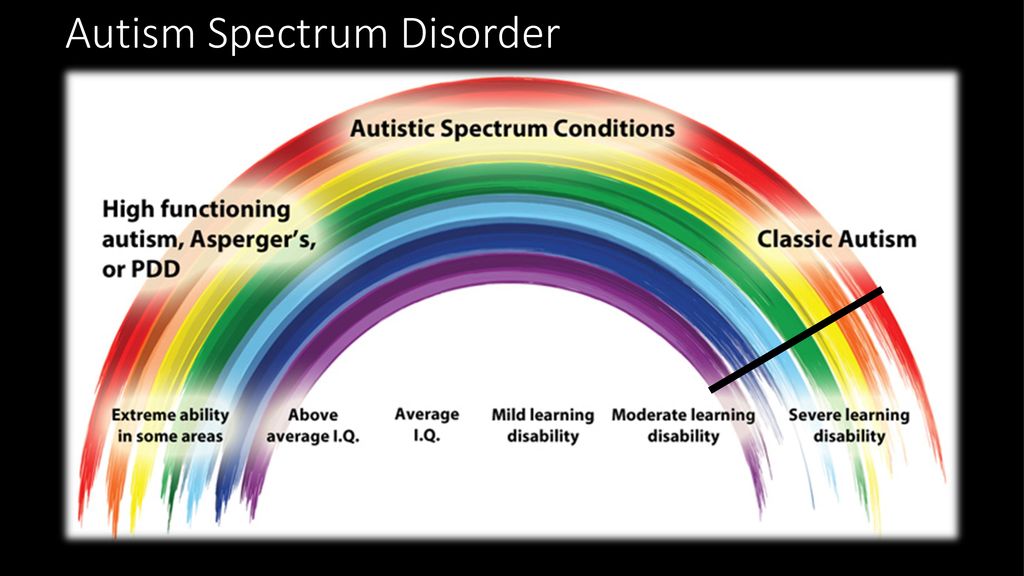 4) 6 3 3
4) 6 3 3
Total: 37 23 14
%. Atypical autism was detected in 10.8% of cases. Of the total number of children, 10.8% have Asperger's syndrome, 1 child (2.7%) has Rett's syndrome.
another disintegrative disorder of childhood, as well as a hyperactive disorder, combined with mental retardation and stereotypical
movements.
The largest number of children with autism spectrum disorders at the age of 5 years - 10 people (27%),
the smallest - at the age of 3 years - 4 people (11%). At the age of 4 years - 9 children (24%), at 6 years old - (22%), 7 years old - 13%, at 8 years old - 3%. The average age of the examined children is 5 years. The peak of the number of surveyed falls on the primary school age - 5-7 years, which reflects the rather late detection of ASD.
The Childhood Autism Rating Scale (CARS) was used to quantify the severity of autism spectrum disorders. The distribution of children depending on the severity of ASD on a scale (CARS) is presented in Table 3.
Table 3. Distribution of children depending on the severity of ASD on a scale _(CARS)_
Diagnosis Total number of children 15-29.5 points - no signs of ASD 30-36.6 points - mild - moderate signs of ASD 37-60 points - severe signs of ASD
Childhood autism (B 84.0) 16 0 4 12
Atypical autism (B 84.1) 4 1 1 2
Asperger's syndrome (B 84.5) 4 2 2 0 Rett syndrome (B0
84.2) 1 0 0 1Disintegrative disorder of childhood (B 84.3) 6 2 2 2
Hyperactive disorder associated with mental retardation and stereotyped movements (B 84.4) 6 0 3 3
Total: 37 5 12 20
severe features of autism spectrum disorder. Children diagnosed with childhood autism, atypical
autism, Rett syndrome in most cases showed severe signs of ASD. In the group of children with hyperactive disorder,
combined with mental retardation and stereotyped movements, severe and moderate signs of autism spectrum disorders were detected to the same extent. Severe signs of autism spectrum disorders in children diagnosed with childhood disintegrative disorder were found only in half of the cases. With Asperger's syndrome, half of the subjects had mild signs of ASD. Moderately pronounced signs of autism spectrum disorders were found in 12 people (29.7%) among all examined children. In 13.5% (5 people) of cases, signs of autism spectrum disorders were not detected or did not reach the value of mild severity.
Severe signs of autism spectrum disorders in children diagnosed with childhood disintegrative disorder were found only in half of the cases. With Asperger's syndrome, half of the subjects had mild signs of ASD. Moderately pronounced signs of autism spectrum disorders were found in 12 people (29.7%) among all examined children. In 13.5% (5 people) of cases, signs of autism spectrum disorders were not detected or did not reach the value of mild severity.
Conclusion. An analysis of the results obtained and their correlation with individual groups of general developmental disorders allows us to draw a number of conclusions. Severe signs of autism spectrum disorders in the vast majority of cases are detected in children diagnosed with "Children's autism", "Atypical autism", but among the examined, in 5 children, significant severity of autistic manifestations was not found, which may indicate the absence of ASD.
Thus, the use of the rating scale (CARS) to assess the severity of autistic manifestations improves the quality of diagnosis verification and differential diagnosis of
ASD with other mental disorders, and also provides an opportunity to develop individual programs for the medical, psychological and pedagogical rehabilitation of patients with ASD.