Mental health cpt codes list 2016
Mental Health CPT Codes: The Definitive Guide [2022]
CPT (Current Procedural Terminology) is a standardized medical codeset maintained by the AMA. CPT codes are five digit numeric codes describing everything from surgery to radiology to psychotherapy.
CPT Codes are different from Diagnosis Codes or ICD10 F-Codes for billing and coding your insurance claims. Here’s our mental health diagnosis code list if you need to look one up.
For therapists that are on managed care panels or provide superbills to their clients, knowing your CPT codes is paramount to getting paid in full and avoiding insurance audits.
The amount insurance companies will reimburse depends on a number of different factors (professional credentials, geographic location, etc.), but using the correct CPT Code and add-on code(s) to express the exact service is an important part to the whole process and in ultimately determining your payment!
Errors, accidental or otherwise, will directly impact insurance company’s payment of services. If you need help with making sure your billing and coding is error-free, our mental health billing service can help.
Think about reaching out if the rest of this article hurts your feelings.
Article Index:
- Most Common Mental Health CPT Codes
- Add-On CPT Codes for Mental Health Billing
- Mental Health CPT Code Cheat Sheet [PDF]
- Testing & Evaluation CPT Codes
- Psych and Evaluation and Management (E/M) Codes
- Sample Reimbursement Rates by License Type
- Sample Reimbursement Rates by CPT Code
The most common CPT Codes used by therapists and behavioral health professionals:
Outpatient Mental Health Therapist Diagnostics, Evaluation, Intake CPT Code:- 90791 – Psychiatric Diagnostic Evaluation (usually just one/client is covered)
- 90832 – Psychotherapy, 30 minutes (16-37 minutes).
- 90834 – Psychotherapy, 45 minutes (38-52 minutes).
- 90837 – Psychotherapy, 60 minutes (53 minutes and over).
- 90846 – Family or couples psychotherapy, without patient present.
- 90847 – Family or couples psychotherapy, with patient present.
- 90853 – Group Psychotherapy (not family).
- 98968 – Telephone therapy (non-psychiatrist) – limit 3 units/hours per application.
- 90839 – Psychotherapy for crisis, 60 minutes (30-74 minutes).
- +90840 – Add-on code for an additional 30 minutes (75 minutes and over). Used in conjunction with 90839.
- +90785 – Interactive Complexity add-on code. Covered below.
- 90404 – Cigna / MHN EAP CPT Code. These two companies use a unique CPT code for EAP sessions.

- 96101 – Psychological testing, interpretation and reporting by a psychologist (per Hour)
- 90880 – Hypnotherapy – limit 10 units/hours per application
- 90876 – Biofeedback
- 90849 – Multiple family group psychotherapy
- 90845 – Psychoanalysis
Mental Health Add-On CPT Codes
Here is a short list of the most common Add-On codes for routine outpatient mental health billing.
- Add-On CPT Code 90785 – Interactive complexity. Example: play therapy using dolls or other toys. This is an interactive complexity add-on code that is not a payable expense. This code only indicates that the treatment is complex in nature.
- Add-On CPT Code 90863 – Pharmacologic Management after therapy.
- Add-On CPT Code 99050 – Services provided in the office at times other than regularly scheduled office hours, or days when the office is normally closed.
- Add-On CPT Code 99051 – Services provided in the office during regularly scheduled evening, weekend, or holiday office hours.
- Add-On CPT Code 99354 – Additional time after the additional time of 74 minutes. Adding another 30 minutes. (Only use if the duration of your session is at least 90 minutes for 90837 or 80 minutes for 90847).
- Add-On CPT Code 99355 – Additional time after first 60 minutes. First additional 30 to 74 minutes.
- Add-On CPT Code 90840 – 30 additional minutes of psychotherapy for crisis. Used only in conjunction with CPT 90839.
- Add-On CPT Code 90833 – 30 minute psychotherapy add-on. Example: Psychiatrist evaluates medication response, then has 30 minute session.
- Add-On CPT Code 90836 – 45 minute psychotherapy add-on. Example: Clinical Nurse Specialist evaluates medication response, then has 45 minute session.
If you’re wondering how to handle billing add-on codes, we can help make this process simple and automatic. Learn how we can help by inquiring about our billing service.
- 90792 – Psychiatric Diagnostic Evaluation with medical services (usually just one/client is covered)
- 99201 – E/M – New Patient Office Visit – 10 Minutes
- 99202 – E/M – New Patient Office Visit – 20 Minutes
- 99203 – E/M – New Patient Office Visit – 30 Minutes
- 99204 – E/M – New Patient Office Visit – 45 Minutes
- 99205 – E/M – New Patient Office Visit – 60 Minutes
- 99211 – E/M – Established Patients – 5 Minutes
- 99212 – E/M – Established Patients – 10 Minutes
- 99213 – E/M – Established Patients – 15 Minutes
- 99214 – E/M – Established Patients – 25 Minutes
- 99215 – E/M – Established Patients – 40 Minutes
- 99443 – Telephone therapy (psychiatrist), – limit 3 units/hours per application
Mental Health CPT Code Cheat Sheet
Download a copy of our PDF Behavioral Health CPT Code Cheat Sheet!
CPT Coding for TherapyCPT coding for psychotherapy doesn’t have to be difficult! There are an overwhelming amount of total CPT Codes (~8,000), however only 24 are specifically designated for psychotherapy and other mental health services.
To make matters even simpler, nearly all therapists will regularly use an even smaller subset of these 24.
CPT is a large and dynamic code set that changes year to year, but the psychotherapy codes seldom change.
The most recent change for psychotherapy codes took place in 2019, then 2013, and previously 1998.
To ensure your coding is current and up to date, consider using a billing service instead of having to remember all the codes.
Behavioral Health CPT Add-On Codes
A CPT Add-on Code is a code describing a service performed in in conjunction with a primary service. Many of these add-on codes are associated with a specific CPT Code or a small set of CPT Codes and cannot be used otherwise.
For instance, the behavioral health CPT Code for interactive complexity (+90785) can be used for a diagnostic (90791, 90792) or a normal psychotherapy session (90832, 90834, 90837) but not a crisis psychotherapy session (90839).
Add-on Codes are identified by a + sign in front of the number, i. e. +90840 is an add-on code for extra time in the case of crisis psychotherapy.
e. +90840 is an add-on code for extra time in the case of crisis psychotherapy.
On CMS 1500 forms CPT Add-on codes are simply added on a new line.
Add-on codes are extremely important to use in order to most accurately describe the services being rendered and to ensure your services are maximized per session.
We help the mental health providers that work with us in our billing service do all of this for every appointment.
Mental Health Testing CPT Codes [2020]
These codes are only effective January 1st, 2019.
Assessment of Aphasia and Cognitive Performance Testing CPT Codes
CPT Code 96105
Assessment of aphasia (includes assessment of expressive and receptive speech and language function, language comprehension, speech production ability, reading, spelling, writing, e.g., by Boston Diagnostic Aphasia Examination) with interpretation and report, per hour
CPT Code 96125
Standardized cognitive performance testing (e. g., Ross Information Processing Assessment) per hour of a qualified health care professional’s time, both face-to-face time administering tests to the patient and time interpreting these test results and preparing the report
g., Ross Information Processing Assessment) per hour of a qualified health care professional’s time, both face-to-face time administering tests to the patient and time interpreting these test results and preparing the report
Developmental/Behavioral Screening and Testing
CPT Code 96110
Developmental screening (e.g., developmental milestone survey, speech and language delay screen), with scoring and documentation, per standardized instrument
CPT Code 96112
Developmental test administration (including assessment of fine and/or gross motor, language, cognitive level, social, memory, and/ or executive functions by standardized developmental instruments when performed), by physician or other qualified health care professional, with interpretation and report; first hour
Add-on CPT Code + 96113 – Each additional 30 minutes (List separately in addition to code for primary procedure)
CPT Code 96127
Brief emotional/behavioral assessment (e.g. , depression inventory, attention-deficit/hyperactivity disorder [ADHD] scale), with scoring and documentation, per standardized instrument
, depression inventory, attention-deficit/hyperactivity disorder [ADHD] scale), with scoring and documentation, per standardized instrument
Psychological/Neuropsychological Testing CPT Codes
These codes have changed in 2019.
Neurobehavioral Status Exam CPT Codes
CPT Code 96116
Neurobehavioral status exam (clinical assessment of thinking, reasoning and judgement, e.g., acquired knowledge, attention, language, memory, planning and problem solving, and visual spatial abilities), by physician or other qualified health care professional, both faceto-face time with the patient and time interpreting test results and preparing the report; first hour
Add-on CPT Code +96121 – Each additional hour (List separately in addition to code for primary procedure)
Test Evaluation Services CPT Codes
CPT Code 96130
Psychological testing evaluation services by physician or other qualified health care professional, including integration of patient data, interpretation of standardized test results and clinical data, clinical decision making, treatment planning and report and interactive feedback to the patient, family member(s) or caregiver(s), when performed; first hour
Add-on CPT Code +96131 – Each additional hour (List separately in addition to code for primary procedure)
CPT Code 96132
Neuropsychological testing evaluation services by physician or other qualified health care professional, including integration of patient data, interpretation of standardized test results and clinical data, clinical decision making, treatment planning and report and interactive feedback to the patient, family member(s) or caregiver(s), when performed; first hour
Add-on CPT Code +96133 – Each additional hour (List separately in addition to code for primary procedure)
Test Administration and Scoring CPT Codes
CPT Code 96136
Psychological or neuropsychological test administration and scoring by physician or other qualified health care professional, two or more tests, any method, first 30 minutes
Add-on CPT Code +96137 – Each additional 30 minutes (List separately in addition to code for primary procedure)
CPT Code 96138
Psychological or neuropsychological test administration and scoring by technician, two or more tests, any method; first 30 minutes
Add-on CPT Code +96139 – Each additional 30 minutes (List separately in addition to code for primary procedure)
Automated Testing and Result CPT Codes
96146 – Psychological or neuropsychological test administration, with single automated instrument via electronic platform, with automated result only
Mental Health Evaluation & Management (E/M) Codes
There are also E/M (evaluation & management) in conjunction with psychotherapy, used by authorized prescribers, psychiatrists, and MDs.
Coding E/M is trickier, harder to document and more vulnerable to audit but usually results in greater reimbursement.
There’s also a series of E/M codes that are used without the psychotherapy component.
For more in-depth coverage on E/M coding for psychotherapy there are some good free webinars released by AACAP on E/M CPT Codes.
- Add-on CPT Code +90833 – E/M code for 30 minutes of psychiatry (used with 90832).
- Add-on CPT Code +90836 – E/M code for 45 minutes of psychiatry (used with 90834).
- Add-on CPT Code +90838 – E/M code for 60 minutes of psychotherapy (used with 90837).
- Psychotherapy must be at least 16 minutes.
- Time is very important and should be rounded to the nearest CPT Code.
- Outpatient vs. Inpatient is not important.
- E/M codes can only be used by prescribers (MD, DO, APN, PA).
Medicare 2022 Reimbursement Rates by CPT Code
| CPT Code | Description | Medicare Reimbursement Rate 2020 | Medicare Reimbursement Rate 2021 | Medicare Reimbursement Rate 2022 |
|---|---|---|---|---|
| 90791 | Psychological Diagnostic Evaluation | $140. 19 19 | $180.75 | $195.46 |
| 90792 | Psychological Diagnostic Evaluation with Medication Management | $157.49 | $201.68 | $218.90 |
| 90832 | Individual Psychotherapy, 30 Minutes | $68.47 | $77.81 | $85.07 |
| 90833 | Individual Psychotherapy with Evaluation and Management Services, 30 minutes | $71.00 | $71.18 | $77.88 |
| 90834 | Individual Psychotherapy, 45 Minutes | $91.18 | $103.28 | $112.29 |
| 90836 | Individual Psychotherapy with Evaluation and Management Services, 45 minutes | $89.74 | $90.02 | $98.30 |
| 90837 | Individual Psychotherapy, 60 Minutes | $136.95 | $152.48 | $164.84 |
| 90838 | Individual Psychotherapy with Evaluation and Management Services, 60 minutes | $118.57 | $119.33 | $129.30 |
| 90839 | Individual Crisis Psychotherapy initial 60 min | $157. 66 66 | ||
| 90840 | Individual Crisis Psychotherapy initial 60 min, each additional 30 min | $78.64 | ||
| 99201 | Evaluation and Management Services, Outpatient, New Patient | $46.49 | Not Covered | Not covered |
| 99202 | Evaluation and Management Services, Outpatient, New Patient | $77.48 | $73.97 | $80.91 |
| 99203 | Evaluation and Management Services, Outpatient, New Patient | $109.92 | $113.75 | $124.39 |
| 99204 | Evaluation and Management Services, Outpatient, New Patient | $166.86 | $169.93 | $185.26 |
| 99205 | Evaluation and Management Services, Outpatient, New Patient | $209.75 | $224.36 | $244.99 |
| 99211 | Evaluation and Management Services, Outpatient, Established Patient | $23.07 | $23.03 | $25.71 |
| 99212 | Evaluation and Management Services, Outpatient, Established Patient | $45. 77 77 | $56.88 | $62.76 |
| 99213 | Evaluation and Management Services, Outpatient, Established Patient | $75.32 | $92.47 | $100.57 |
| 99214 | Evaluation and Management Services, Outpatient, Established Patient | $110.28 | $131.20 | $141.78 |
| 99215 | Evaluation and Management Services, Outpatient, Established Patient | $147.76 | $183.19 | $200.00 |
| 99354 | Prolonged Services | $132.26 | $132.09 | $140.26 |
| 99355 | Prolong Services with E/M | $100.91 | $100.33 | $101.32 |
| 90846 | Family psychotherapy without patient, 50 minutes | $103.58 | $99.10 | $107.37 |
| 90847 | Family psychotherapy with patient, 50 minutes | $107.19 | $102.59 | $111.15 |
| 96105 | Assessment of aphasia and cognitive performance | $101. 54 54 | $109.26 | |
| 96112 | Developmental testing administration by a physician or qualified health care professional, 1st hr | $131.55 | $141.02 | |
| 96113 | Developmental testing administration by a physician or qualified health care professional, each additional hour | $58.62 | $66.54 | |
| 96116 | Neurobehavioral status exam performed by a physician or qualified health professional, first hour | $97.00 | $104.73 | |
| 96121 | Neurobehavioral status exam performed by a physician or qualified health professional, additional hour | $82.35 | $87.34 | |
| 96125 | Standardized cognitive performance test administered by health care professional | $107.12 | $115.69 | |
| 96127 | Brief emotional and behavioral assessment | $4.89 | $5.29 | |
| 96130 | Psychological testing and evaluation by a physician or qualified health care professional, first hour | $120. 73 73 | $132.70 | |
| 96131 | Psychological testing and evaluation by a physician or qualified health care professional, each additional hour | $91.42 | $98.68 | |
| 96132 | Neuropsychological testing and evaluation by a physician or qualified health care professional, first hour | $133.29 | $144.80 | |
| 96133 | Neuropsychological testing and evaluation by a physician or qualified health care professional, each additional hour | $103.98 | $112.29 | |
| 96136 | Neuropsychological or psychological test administration and scoring by a physician or qualified health care professional, first hour | $46.76 | $49.15 | |
| 96137 | Neuropsychological or psychological test administration and scoring by a physician or qualified health care professional, each additional hour | $41.87 | $44.24 | |
| 96138 | Neuropsychological or psychological test administration and scoring by a technician, first hour | $37. 34 34 | $38.56 | |
| 96139 | Neuropsychological or psychological test administration and scoring by a technician, each additional hour | $37.34 | $$39.32 |
(Source)
Interactive Complexity (+90785): Criteria and How to Bill+90785 is one of the new add-on codes in the most recent CPT update in 2013.
This code is used as an umbrella add-on code and can be used for four different criteria. The most common scenarios usually involve children, although this is not necessarily always the case.
Common Examples of Interactive Complexity:
- The use of play equipment with young children.
- Interpreters/translators.
- Involvement of parents with discordant views that complicate the treatment plan.
- Report of abuse/neglect.
Interactive complexity can be used in conjunction with the primary CPT Codes for diagnostics, psychotherapy, or group therapy and cannot be used for couple/family therapy or crisis codes.
+90785, can be used with: 90791, 90792, 90832, 90833, 90834, 90836, 90837, 90838, 90853.
Unsure when to use the interactive complexity code? Need help asking if it will be approved? Our billing service exclusively for mental health providers is here to help.
Am I Being Underpaid? Was I Paid the Right Amount?Here’s typical rates depending on the therapist’s credentials:
Typical Reimbursements by Type of Therapist| Type of Therapist | Reimbursement/Session |
| Social Workers | ~$55-60 |
| Marriage Family Therapists | ~$60-65 |
| Counselors | ~$60-65 |
| Psychologists | ~$70-80 |
These rates can vary significantly therapist to therapist but are good benchmarks for comparison.
How about CPT Codes? How do they affect the rate of reimbursement? This is a difficult and complex calculation, depending on the level of education, location, and license. The AMA has created a code search feature on their website that shows payment based off CPT Code and location.
The AMA has created a code search feature on their website that shows payment based off CPT Code and location.
This information is somewhat incomplete and is based off medicare payments and does not specify a number of other important factors. However, this tool is still very useful to compare the relative value CPT Codes against one another.
Private insurance will be correlated with some deviation from these numbers.
Reimbursement by CPT Code (Three Different Geographies)Reimbursement (Rest of CA)Reimbursement (Los Angeles)Reimbursement (WA)
| Code | California | Los Angeles | Washington |
| 90791 | $137.10 | $141.17 | $132.98 |
| 90792 | $147.84 | $152.16 | $143.39 |
| 90832 | $66.14 | $68.03 | $64.25 |
| +90833 | $67.69 | $69.69 | $65.70 |
| 90834 | $87.66 | $90. 15 15 | $85.18 |
| +90836 | $85.71 | $88.21 | $83.18 |
| 90837 | $131.28 | $134.95 | $127.54 |
| +90838 | $113.07 | $116.42 | $109.75 |
| 90846 | $106.46 | $109.51 | $103.38 |
| 90847 | $109.75 | $112.82 | $106.60 |
| 90853 | $26.99 | $27.83 | $26.21 |
| 90839 | $137.22 | $141.04 | $133.28 |
| +90840 | $65.75 | $67.61 | $63.89 |
| +90785 | $14.67 | $15.08 | $14.24 |
Data from AMA Codemanager. These numbers are useful for relative comparison of individual CPT Codes and geography.
Therapist Reimbursement Rates for 2022
Read our definitive guide with 2022 reimbursement rates for mental health CPT codes.
Downcoding Claims
Downcoding (including less services on the claim than actually provided) will usually mean you get paid less, while upcoding (including more services on the claim than actually provided) can get you in trouble with your managed care panels.
It’s also important to note that it might be tempting to maximize your CPT codes to earn higher reimbursements.
This is highly recommended against and can get you flagged, audited and removed from insurance panels. Even if this is your biller’s error, the therapist is the one who ultimately bears the responsibility and will be the one penalized.
Here’s a video guide we did of this article!
Distilled Guide to Mental Health CPT Codes
If you are just starting out or just beginning to deal with managed care, keep it simple.
CPT Codes appear far more complex from the outside looking in. Make a quick cheatsheet.
Don’t worry about memorizing all the CPT Codes (there’s alot!) or even all of the mental health ones. You will likely just use just a few individual codes.
Memorize the relevant codes and use google or other references to find the correct CPT codes for more unique scenarios.
Call to verify eligibility and benefits and make sure those codes will be approved with that client’s coverage.
And if all of that sounds like too much trouble, offload the work to us. You won’t have to know one CPT code from another to get your billing paid in full.
Additional Resources- Medicare Reimbursement by CPT Code & Area
- CPT Reimbursement Lookup & RVU (Relative Value Unit) Overview
- Crosswalk of 2012 to 2013 CPT Codes
- CPT 2013 Standard Edition [Probably Unnecessary]
- Insurance Reimbursement Comparison Tool
Consider Outsourcing Your Billing
Don’t want to learn any of this stuff? We are your team of billing experts here to translate all of this gibberish into English! Reach out about our billing service if you are a licensed mental health provider (we only work with licensed mental health providers).
202020212022behavioral health cpt codesmental health billing guidemental health cpt codesmental health cpt codes guidemost common mental health cpt codes
A Guide to Medicare Mental Health Billing Codes
Navigating the requirements of Medicare can be a challenge. But here’s some good news — CPT codes are the same for all payers, whether they are a private insurer or a government program, like Medicare. Once you know the appropriate codes to use for each of the services you provide to clients, that piece of the puzzle is solved.
But here’s some good news — CPT codes are the same for all payers, whether they are a private insurer or a government program, like Medicare. Once you know the appropriate codes to use for each of the services you provide to clients, that piece of the puzzle is solved.
The rules around timed and untimed codes, however, are more complex. Medicare has strict specifications for calculating how to bill for time increments, and you’ll want to be sure you follow their guidelines. Here’s what you need to know about CPT billing codes for mental health and Medicare’s 8-Minute Rule.
Medicare CPT Billing Codes for Mental Health
Here’s a list of the most common CPT codes for mental health services, which you’ll use with every payer, both private and public.
- 90832 — Individual psychotherapy for 30 minutes
- 90833 — Individual psychotherapy for 30 performed with an E/M service
- 90834 — Individual psychotherapy for 45 minutes
- 90836 — Individual psychotherapy for 45 performed with an E/M service
- 90837 — Individual psychotherapy for 60 minutes
- 90838 — Individual psychotherapy for 60 performed with an E/M service
- 90846 — Family psychotherapy for 50 minutes without the patient present
- 90847 — Family psychotherapy for 50 minutes with the patient present
- 90853 — Group psychotherapy
- 96127 — Brief behavioral or emotional assessment
- 96130 — Evaluation services including reporting, treatment planning, clinical decision-making, interpreting test results, and providing feedback to patient, caregivers, or family members
- 96131 — Testing evaluation services, psychological and neuropsychological
- 96136 — Test administration and scoring, first 30 minutes
- 96137 — Test administration and scoring, additional 30 minutes
- 99354 — Prolonged services, first 60 minutes
- 99355 — Prolonged services, first 60 minutes with an E/M service
- H0032 — Mental health service plan
Many of the codes have rules around how much time you must spend with a client in order to claim the code. This is where the 8-Minute Rule comes into play. While this rule comes from Medicare, most private payers have followed suit. So it’s good to have a working knowledge of this rule regardless of whether you accept Medicare.
This is where the 8-Minute Rule comes into play. While this rule comes from Medicare, most private payers have followed suit. So it’s good to have a working knowledge of this rule regardless of whether you accept Medicare.
Medicare’s 8-Minute Rule for Timed Codes
There are two kinds of CPT codes: service-based codes and time-based codes. Service-based codes can only be billed once, regardless of the amount of time spent to perform the service. Time-based codes require a therapist to bill based on the time spent with the client while delivering the service. Though it sounds simple enough, it can be challenging when a therapist bills both service-based and time-based code for a client.
The Medicare 8-Minute Rule outlines the process you should use to determine how many “units” you should bill for services using time-based CPT codes. In short, you must spend a minimum of 8 minutes with a client to bill for a unit, but there are guidelines for additional time spent.
CMS, the Center for Medicare and Medicaid Services, provides this guidance: “When only one service is provided in a day, providers should not bill for services performed for less than 8 minutes. For any single timed CPT code in the same day measured in 15 minute units, providers bill a single 15-minute unit for treatment greater than or equal to 8 minutes through and including 22 minutes. If the duration of a single modality or procedure in a day is greater than or equal to 23 minutes through and including 37 minutes, then 2 units should be billed.”
For any single timed CPT code in the same day measured in 15 minute units, providers bill a single 15-minute unit for treatment greater than or equal to 8 minutes through and including 22 minutes. If the duration of a single modality or procedure in a day is greater than or equal to 23 minutes through and including 37 minutes, then 2 units should be billed.”
Though it seems fairly straight-forward, there are nuances that can make applying the 8-minute rule difficult. Here are some examples to help you understand how to comply with this guideline.
Billing for Single Treatments
When one service is provided in a day, billing is fairly straight-forward — time-based CPT codes are measured in 15-minute units. Providers shouldn’t bill for any service performed for less than 8 minutes. So, if you use 7 minutes for treatment, you wouldn’t be able to bill. For a therapeutic service lasting 8 minutes, you can bill for one 15-minute unit of time. At 22 minutes, the time is still counted as one unit of time, but 23 minutes counts as two (since it is 8 minutes past the 15-minute mark). Billing is still done in 15-minute increments, and the 8-minute rule is used to determine when the 15-minute time increment shifts for billing purposes.
Billing is still done in 15-minute increments, and the 8-minute rule is used to determine when the 15-minute time increment shifts for billing purposes.
Billing for Multiple Treatments
The chart and the example above works for single treatments in a day, but what about when you provide multiple treatments within a single day? Let’s look at a couple of different scenarios.
1. Multiple Short Treatments
When you provide more than one timed treatment and each is less than 8 minutes, you would bill one unit of time. Per the guidelines, whenever multiple timed treatments are offered within one day, with each taking less than 8 minutes, you should total up the time spent on all treatments, then bill one unit of time for the CPT code that you spent the most time on. So, if two treatments are provided that are under 8 minutes each, where one is 7 minutes and one is 5, the total exceeds 8 — so one unit of time can be billed, and the time will be billed to the treatment that was 7 minutes of time.
2. Multiple Treatments of at Least 8 Minutes
In this situation, you’re providing more than one service in a day and each of the services are over 8 minutes of time. Regardless of the treatment time, the CMS guidelines say you should total up the time spent on all treatments and bill based on the total time. So, if three treatments are provided that are 8 minutes, 10 minutes, and 14 minutes, the total time is 32 minutes which equates to two units of 15-minute time increments. (Or, divide the total time of 32 minutes by 15 and round down to the nearest number of units.) In this example, the CPT code corresponding to the 14-minute treatment will be billed 2 units of time.
While mental health CPT codes are straightforward, Medicare’s rules around timed codes are a bit challenging and require calculations. But the chart above makes it easy to quickly determine what to bill. Keep it as a handy reference!
See how KASA can help make billing simpler so you can focus on helping your clients.
Learn More About KASA Billing Services
Population pharmacokinetic analysis in Lixoft Monolix | Platova
1. Guideline on reporting the results of population pharmacokinetic analyses. Doc. Ref. CHMP/EWP/185990/06. June 21, 2007. Electronic resource. European Medicines Agency Official website. URL: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003067.pdf (accessed: 12/13/2020).
2. Owen JS, Fiedler-Kelly J. Introduction to population pharmacokinetic / pharmacodynamic analysis with nonlinear mixed effects models. Hoboken, New Jersey: John Wiley & Sons; 2014. 301 p.
3. Lavielle M, Mentre F. Estimation of population pharmacokinetic parameters of saquinavir in HIV patients with the MONOLIX software. J Pharmacokinet Pharmacodyn. 2007;34(2):229–249. DOI:10.1007/s10928-006-9043-z.
4. Dedov I.I., Tyulpakov A.N., Chekhonin V.P., Baklaushev V.P., Archakov A.I., Moshkovsky S.A. Personalized medicine: current state and prospects. Bulletin of RAMN. 2012;(12):4–12.
Bulletin of RAMN. 2012;(12):4–12.
5. Sheiner LB. The population approach to pharmacokinetic data analysis: rationale and standard data analysis methods. Drug Metab Rev. 1984; 15(1-2):153–171. DOI:10.3109/03602538409015063.
6. Guidance for Industry. Population Pharmacokinetics. FDA. CDER. CBER. February, 1999. Electronic resource. US. Food and Drug Administration (FDA). official website. URL: http://www.fda.gov/downloads/Drugs/Guidances/UCM072137.pdf (accessed: 12/13/2020).
7. Therapeutic drug monitoring: a tool for personalized medicine (guidelines) / ed. acad. RAMS V.G. Kukes (Russia) and prof. D. Berry (Great Britain). M.: Publishing house of the Autonomous non-profit organization "International Association of Clinical Pharmacologists and Pharmacists"; 2013: 48 p.
8. Long-Boyle JR, Savic R, Yan S, et al. Population pharmacokinetics of busulfan in pediatric and young adult patients undergoing hematopoietic cell transplant: a model-based dosing algorithm for personalized therapy and implementation into routine clinical use.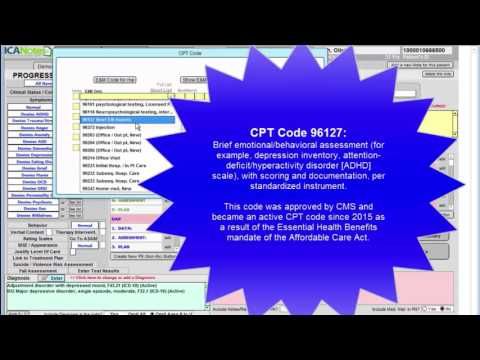 Ther Drug Monit. 2015;37(2):236–245. DOI:10.1097/FTD.0000000000000131.
Ther Drug Monit. 2015;37(2):236–245. DOI:10.1097/FTD.0000000000000131.
9. Soloviev V.N., Firsov A.A., Filov V.A. Pharmacokinetics. M.: Medicine; 1980. 494 p.
10. Karkishchenko N.N., Khoronko V.V., Sergeeva S.A., Karkishchenko V.N. Pharmacokinetics. Rostov-on-Don: Phoenix; 2001. 384 p.
11. Sergienko V.I., Jelliff R., Bondareva I.B. Applied Pharmacokinetics: Fundamentals and Clinical Applications. M.: Publishing house of the Russian Academy of Medical Sciences; 2003. 208 p.
12. Miroshnichenko I.I. Rational dosing and monitoring of medicines. Moscow: LLC Publishing House Medical Information Agency; 2011: 353–371.
13. Heeremans EH, Proost JH, Eleveld DJ, et al. Population pharmacokinetics and pharmacodynamics in anesthesia, intensive care and pain medicine. Curr Opin Anaesthesiol. 2010;23(4):479-484. DOI:10.1097/ACO.0b013e32833a1d2f.
14. Watanabe-Uchida M, Watanabe T, Narukawa M. The Current State and Future Prospects of Population Pharmacokinetic Research in Postmarketing Clinical Studies in Japan. Yakugaku Zasshi. 2019;139(10):1297–1303. DOI:10.1248/yakushi.18-00227.
Yakugaku Zasshi. 2019;139(10):1297–1303. DOI:10.1248/yakushi.18-00227.
15. Beal SL, Sheiner LB. NONMEM users guides In EDS. text data. San Francisco: NONMEM Project Group. University of California, CA; 1992 (CD-ROM).
16. Kholodov L.E., Yakovlev V.P. Clinical pharmacokinetics. M.: Medicine; 1985. 464 p.
17. Moon YJ, Wang L, DiCenzo R, Morris ME. Quercetin pharmacokinetics in humans. Biopharm Drug Dispos. 2008;29(4):205–217. DOI:10.1002/bdd.605.
18. Vonesh EF, Carter RL. Mixed-effects nonlinear regression for unbalanced repeated measures. Biometrics.1992;48(1):1–17.
19. Bauer RJ, Guzy S, Chee Ng. A survey of population analysis methods and software for complex pharmacokinetic and pharmacodynamic models with examples. AAPS J. 2007;9(1): E60-E83. DOI:10.1208/aapsj07.
20. Joerger M. Covariate pharmacokinetic model building in oncology and its potential clinical relevance. AAPS J. 2012;14(1):119–132. DOI:10.1208/s12248-012-9320-2.
21. Gorkov V.A., Karamysheva E.I. Introduction to pharmacokinetics. Pharmacokinetics and pharmacodynamics. 2004;(1):2–4.
22. WinNonlin® User's Guide in EDS.: Pharsight Corporation. University of California, 800 West El Camino Real, Suite 200, Mountain View, California 94040, 2009. (CD-ROM).
23. Gibaldi M, Perrier D. Pharmacokinetics. New York: Marcell Decker; 1982.
24. Gabrielsson J, Weiner D. Pharmacokinetic and pharmacodynamic data analysis: concepts and applications. Stockholm: Swedish Pharmaceutical Press; 2000 (third edition), 925 rubles
25. Rosenbaum S. Basic pharmacokinetics and pharmacodynamics: an integrated textbook and computer simulations. New Jersey: J. Wiley & Sons; 2011, 430 p.
26. Davda JP, Dodds MG, Gibbs MA, Wisdom W, Gibbs J. A model-based meta-analysis of monoclonal antibody pharmacokinetics to guide optimal firstin-human study design. MAbs. 2014;6(4):1094–1102. DOI:10.4161/mabs.29095.
27. Bonate PL, Howard DR. Compartmental models in pharmacokinetics in drug development: clinical study design and analysis. AAPS. 2004;1:291–362.
Compartmental models in pharmacokinetics in drug development: clinical study design and analysis. AAPS. 2004;1:291–362.
28. Clifford AJ, Müller H-G. Mathematical modeling in experimental nutrition. New York: Plenum Press; 1998, 426 p.
29. Frommer A, Szyld DB. H-Splittings and two-stage iterative methods. Numerische Mathematik. 1992;63(1):345–356.
30. Tatarinova T, Neely M, Bartroff J, et al. Two general methods for population pharmacokinetic modeling: non-parametric adaptive grid and non-parametric Bayesian. J Pharmacokinet Pharmacodyn. 2013;40(2):189-199. DOI:10.1007/s10928-013-9302-8.
31. Jelliffe RW, Schumitzky A. Modeling, adaptive control, and optimal drug therapy. Med Prog Technol. 1990;16(1-2)95-110.
32. Savic RM, Mentré F, Lavielle M. Implementation and evaluation of the SAEM algorithm for longitudinal ordered categorical data with an illustration in pharmacokinetics – pharmacodynamics. AAPS J. 2011;13(1):44–53. DOI:10.1208/s12248-010-9238-5.
33. Urien C, Bardin C, Bader-Meunier B et al. Anakinra pharmacokinetics in children and adolescents with systemic-onset juvenile idiopathic arthritis and autoinflammatory syndromes. BMC Pharmacol Toxicol. 2013;14:40. doi:10.1186/2050-6511-14-40.
34. Karlsson MO, Beal SL, Sheiner LB. Three new residual error models for population PK/PD analyses. J Pharmacokinetics Biopharm. 1995;23(6):651–672. DOI:10.1007/BF02353466.
35. Mold DR, Upton RN. Basic concepts in population modeling, simulation, and model-based drug development-part 2: introduction to pharmacokinetic modeling methods. CPT Pharmacometrics Syst Pharmacol. 2013;2(4):e38. DOI:10.1038/psp.2013.14.
36. Miroshnichenko I.I., Platova A.I. Problems of personalization of psychopharmacotherapy. Psychiatry. 2015;(3):85–94.
37. Gatsonis C, Sampson AR. Multiple correlation: exact power and sample size calculations. Psycholl Bull. 1989;106(3):516–524. DOI:10.1037/0033-2909.106.3.516.
38. Kang D, Schwartz JB, Verotta D. Sample size computation method for non-linear mixed effects models with applications to pharmacokinetics models. Stat Med. 2004;23(16): 2551–2566. DOI:10.1002/sim.1695.
Sample size computation method for non-linear mixed effects models with applications to pharmacokinetics models. Stat Med. 2004;23(16): 2551–2566. DOI:10.1002/sim.1695.
39. Samson A, Lavielle M, Mentré F. The SAEM algorithm for group comparison tests in longitudinal data analysis based on non-linear mixedeffects model. Stat Med. 2007;26(27):4860–4875. DOI:10.1002/sim.2950.
40. Retout S, Comets E, Samson A, Mentré F. Design in nonlinear mixed effects models: optimization using the Fedorov–Wynn algorithm and power of the Wald test for binary covariates. Stat Med. 2007;26(28):5162–5179. DOI:10.1002/sim.2910.
41. Bertrand J, Comets E, Laffont CM, Chenel M, Mentré F. Pharmacogenetics and population pharmacokinetics: impact of the design on three tests using the SAEM algorithm. J Pharmacokinet Pharmacodyn. 2009;36(4):317–339. DOI:10.1007/s10928-009-9124-x.
42. Combes FP, Retout S, Frey N, Mentré F. Powers of the likelihood ratio test and the correlation test using empirical bayes estimates for various shrinkages in population pharmacokinetics. CPT Pharmacometrics Syst Pharmacol. 2014;3(4):e109. DOI:10.1038/psp.2014.5.
CPT Pharmacometrics Syst Pharmacol. 2014;3(4):e109. DOI:10.1038/psp.2014.5.
Why is it important to pay attention to your mental health?
Why is it important to pay attention to your mental health?
Many have heard the catchphrase "all diseases are from the nerves." However, as a simple and natural step in case of bodily ailment to seek medical help, just as often the state of stress, anxiety, depression of mood are left without proper attention.
It is known that when people receive appropriate mental health care, they do not often seek medical help in general. There is evidence that people with unresolved mental health problems visit general practitioners twice as often as those who receive specialized, psychiatric and psychological care.
Excessive anxiety and stress can contribute to the development of certain heart diseases, weaken the immune system. Psychological problems also increase the likelihood of incorrect behavioral choices, which manifests itself in addiction to smoking and drugs, alcohol abuse. There is a close relationship between the psyche and the physical state of a person. Feelings of anxiety, constant stress and worries can lead to poor health. People who care about mental health tend to achieve great success, both professionally and personally. Mental health is important in terms of communication, especially in the family. It allows you to maintain a healthy atmosphere in the circle of close people, properly educate children, giving them the necessary care and a psychological model to follow. Mentally healthy people are more resistant to the influence of negative social factors, less prone to the formation of "bad habits". Thus, when a person is free from depression, anxiety, excessive tension and worry, he is able to live fully, fully realized and enjoy.
There is a close relationship between the psyche and the physical state of a person. Feelings of anxiety, constant stress and worries can lead to poor health. People who care about mental health tend to achieve great success, both professionally and personally. Mental health is important in terms of communication, especially in the family. It allows you to maintain a healthy atmosphere in the circle of close people, properly educate children, giving them the necessary care and a psychological model to follow. Mentally healthy people are more resistant to the influence of negative social factors, less prone to the formation of "bad habits". Thus, when a person is free from depression, anxiety, excessive tension and worry, he is able to live fully, fully realized and enjoy.
The state of mental health can only be fully assessed by a specialist. However, for the current assessment of one's own state or the state of the psyche of relatives and friends and making a decision on seeking help, it is enough to pay attention to a number of simple criteria.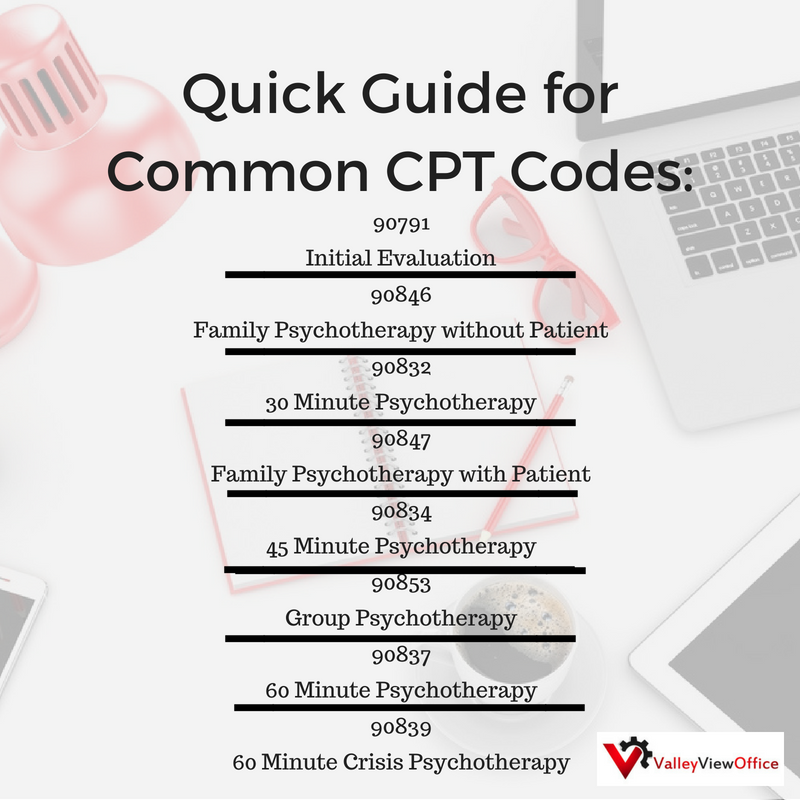
1. Sleep state. Difficulties in falling asleep, restless sleep, unusually early awakenings, and, conversely, increased drowsiness, lack of a feeling of rest upon awakening - all these are sleep disorders that may indicate a dysfunction of the nervous system, and, in themselves, lead to its overstrain, but, means an increased risk of psychiatric disorders.
2. Health level. Mental performance is characterized by the activity of mental processes: attention, memory, thinking. A decrease in mental performance, manifested in the form of insufficient memory functioning, problems with concentration, and difficulty making decisions, can be a sign of many mental disorders and diseases.
3. Emotional state. The emotional sphere is extremely sensitive to various manifestations of trouble. The predominance of negative emotional reactions (bad mood, tearfulness, irritability, anger), their unusual and high intensity, especially in situations of inconsistency with the situation in which they manifest themselves, difficulties in managing their own emotional state - all these are reasons to pay attention to the state of mental health.