Manic depression genetics
SAMHSA’s National Helpline | SAMHSA
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Main page content
-
SAMHSA’s National Helpline is a free, confidential, 24/7, 365-day-a-year treatment referral and information service (in English and Spanish) for individuals and families facing mental and/or substance use disorders.
Also visit the online treatment locator.
SAMHSA’s National Helpline, 1-800-662-HELP (4357) (also known as the Treatment Referral Routing Service), or TTY: 1-800-487-4889 is a confidential, free, 24-hour-a-day, 365-day-a-year, information service, in English and Spanish, for individuals and family members facing mental and/or substance use disorders.
This service provides referrals to local treatment facilities, support groups, and community-based organizations.
Also visit the online treatment locator, or send your zip code via text message: 435748 (HELP4U) to find help near you. Read more about the HELP4U text messaging service.
The service is open 24/7, 365 days a year.
English and Spanish are available if you select the option to speak with a national representative. Currently, the 435748 (HELP4U) text messaging service is only available in English.
In 2020, the Helpline received 833,598 calls. This is a 27 percent increase from 2019, when the Helpline received a total of 656,953 calls for the year.
The referral service is free of charge. If you have no insurance or are underinsured, we will refer you to your state office, which is responsible for state-funded treatment programs. In addition, we can often refer you to facilities that charge on a sliding fee scale or accept Medicare or Medicaid. If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
The service is confidential. We will not ask you for any personal information. We may ask for your zip code or other pertinent geographic information in order to track calls being routed to other offices or to accurately identify the local resources appropriate to your needs.
No, we do not provide counseling. Trained information specialists answer calls, transfer callers to state services or other appropriate intake centers in their states, and connect them with local assistance and support.
-
Suggested Resources
What Is Substance Abuse Treatment? A Booklet for Families
Created for family members of people with alcohol abuse or drug abuse problems. Answers questions about substance abuse, its symptoms, different types of treatment, and recovery. Addresses concerns of children of parents with substance use/abuse problems.
Addresses concerns of children of parents with substance use/abuse problems.It's Not Your Fault (NACoA) (PDF | 12 KB)
Assures teens with parents who abuse alcohol or drugs that, "It's not your fault!" and that they are not alone. Encourages teens to seek emotional support from other adults, school counselors, and youth support groups such as Alateen, and provides a resource list.After an Attempt: A Guide for Taking Care of Your Family Member After Treatment in the Emergency Department
Aids family members in coping with the aftermath of a relative's suicide attempt. Describes the emergency department treatment process, lists questions to ask about follow-up treatment, and describes how to reduce risk and ensure safety at home.Family Therapy Can Help: For People in Recovery From Mental Illness or Addiction
Explores the role of family therapy in recovery from mental illness or substance abuse. Explains how family therapy sessions are run and who conducts them, describes a typical session, and provides information on its effectiveness in recovery.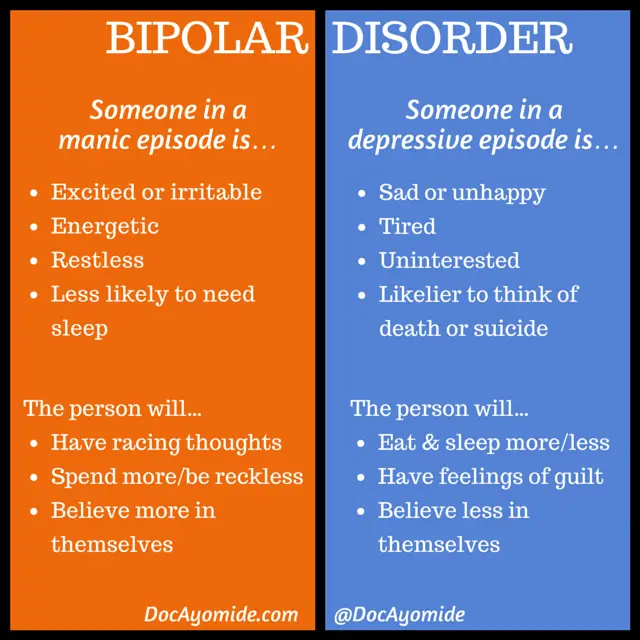
For additional resources, please visit the SAMHSA Store.
Last Updated: 08/30/2022
SAMHSA Behavioral Health Treatment Services Locator
HomeWelcome to the Behavioral Health Treatment Services Locator, a confidential and anonymous source of information for persons seeking treatment facilities in the United States or U.S. Territories for substance use/addiction and/or mental health problems.
PLEASE NOTE: Your personal information and the search criteria you enter into the Locator is secure and anonymous. SAMHSA does not collect or maintain any information you provide.
Please enter a valid location.
please type your address
-
FindTreatment.
 gov
gov Millions of Americans have a substance use disorder. Find a treatment facility near you.
-
988 Suicide & Crisis Lifeline
Call or text 988
Free and confidential support for people in distress, 24/7.
-
National Helpline
1-800-662-HELP (4357)
Treatment referral and information, 24/7.
-
Disaster Distress Helpline
1-800-985-5990
Immediate crisis counseling related to disasters, 24/7.
- Overview
- Locator OverviewLocator Overview
- Locator OverviewLocator Overview
- Finding Treatment
- Find Facilities for VeteransFind Facilities for Veterans
- Find Facilities for VeteransFind Facilities for Veterans
- Facility Directors
- Register a New FacilityRegister a New Facility
- Register a New FacilityRegister a New Facility
- Other Locator Functionalities
- Download Search ResultsDownload Search Results
- Use Google MapsUse Google Maps
- Print Search ResultsPrint Search Results
- Use Google MapsUse Google Maps
- Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
 Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers).
Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). - Icon from Find practitioners and treatment programs providing buprenorphine for opioid addiction (heroin or pain relievers). Find programs providing methadone for the treatment of opioid addiction (heroin or pain relievers).
The Locator is authorized by the 21st Century Cures Act (Public Law 114-255, Section 9006; 42 U.S.C. 290bb-36d). SAMHSA endeavors to keep the Locator current. All information in the Locator is updated annually from facility responses to SAMHSA’s National Substance Use and Mental Health Services Survey (N-SUMHSS). New facilities that have completed an abbreviated survey and met all the qualifications are added monthly. Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Updates to facility names, addresses, telephone numbers, and services are made weekly for facilities informing SAMHSA of changes. Facilities may request additions or changes to their information by sending an e-mail to [email protected], by calling the BHSIS Project Office at 1-833-888-1553 (Mon-Fri 8-6 ET), or by electronic form submission using the Locator online application form (intended for additions of new facilities).
Bipolar affective disorder and everything you need to know about it
More than 60 million people in the world suffer from bipolar affective disorder (BAD). The essence of the disease is that a person has alternating periods of altered mood throughout his life: from a state with a minus sign to a state with a plus sign. How and why is this happening?
Marina KINKULKINA, psychiatrist of the highest category, head of the department of psychiatry and narcology, director of the Institute of Electronic Medical Education, First Moscow State Medical University. I. M. Sechenova, Corresponding Member of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences
I. M. Sechenova, Corresponding Member of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences
Moreover, it is often not just about sadness or fun, as is often the case with emotional people, but about extreme degrees of either despair or euphoria. The change in these moods can take place both gradually and suddenly, and often for no apparent reason. This disease is attributed to Byron and Hemingway, Virginia Woolf and Edgar Poe, Van Gogh, Schumann, Vivien Leigh and many others. There is an assumption that even “our everything” suffered from a mild degree of BAD (contemporaries often mentioned mood swings) A. S. Pushkin. Modern stars - Catherine Zeta-Jones and Mel Gibson - openly admit to having this mental disorder. And rapper Kanye West even put the inscription on the cover of his album: "I hate being bipolar, it's amazing." A very accurate description of the essence of this disease.
Genetics does not solve everything
BAD affects both men and women, but the weaker sex - more often.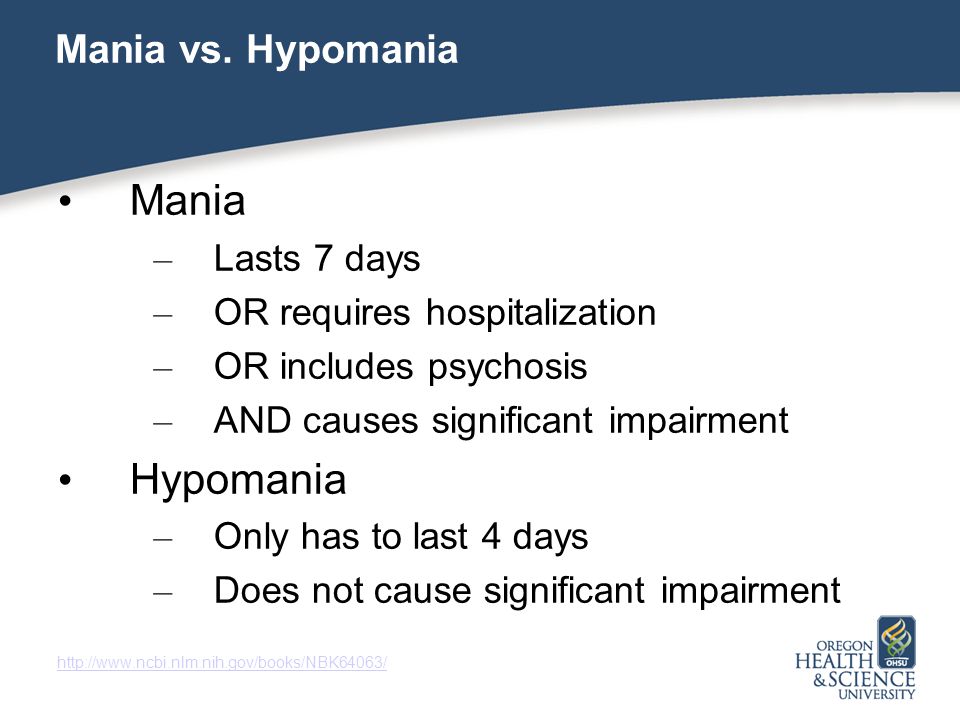 As for the age of onset of the disease, this disorder can also appear in a teenager (especially if there is an appropriate heredity), and in an adult, and even in an elderly person. Everything is individual. The main risk factor is genetics, but a specific gene that would be responsible for the development of bipolar disorder has not been identified. This is a polygenic disorder, and it makes no sense to take genetic tests to find out how great the risk of getting sick is, because scientists still do not have a consensus on what specific combination of genes can lead to a violation. But even if there is a genetic predisposition, it is not certain that the disease will develop. This was proven by studies on identical twins, one of which developed bipolar disorder over the years, while the other did not. Accordingly, there must be some other predisposing moments. Science knows about some of them: life at the limit of possibilities with constant hands-on work, stress and chronic lack of sleep, as well as night shift work, frequent flights with a significant change in hourly flights and, of course, the use of psychoactive substances contribute to the development of the disease.
As for the age of onset of the disease, this disorder can also appear in a teenager (especially if there is an appropriate heredity), and in an adult, and even in an elderly person. Everything is individual. The main risk factor is genetics, but a specific gene that would be responsible for the development of bipolar disorder has not been identified. This is a polygenic disorder, and it makes no sense to take genetic tests to find out how great the risk of getting sick is, because scientists still do not have a consensus on what specific combination of genes can lead to a violation. But even if there is a genetic predisposition, it is not certain that the disease will develop. This was proven by studies on identical twins, one of which developed bipolar disorder over the years, while the other did not. Accordingly, there must be some other predisposing moments. Science knows about some of them: life at the limit of possibilities with constant hands-on work, stress and chronic lack of sleep, as well as night shift work, frequent flights with a significant change in hourly flights and, of course, the use of psychoactive substances contribute to the development of the disease. Therefore, they should be avoided. Scientists have yet to learn about other factors.
Therefore, they should be avoided. Scientists have yet to learn about other factors.
But not boring?
The number of people suffering from bipolar disorder among the population, according to various estimates, varies from fractions of one percent to several percent. Recently, psychiatrists note, the proportion of affective disorders has increased significantly, which can be explained by improved diagnostics. At first glance, the BAR does not look like something scary and dangerous. To ignorant people, this disorder even seems attractive - sometimes sad, sometimes fun, in general, you won’t get bored. In addition, being different from everyone else is now fashionable. And then, there is an opinion that people with BAD have higher intelligence and creative abilities than the “gray masses”. But even if this is so, then none of those who suffer from it will definitely call BAD a pleasant thing. It is especially difficult for those patients who do not seek medical help on time. Without treatment, both phases of bipolar disorder can last for months (although sometimes the disorder occurs with frequently alternating phases). Moreover, it is impossible to say which of the periods of the disease is more difficult, manic or depressive.
Without treatment, both phases of bipolar disorder can last for months (although sometimes the disorder occurs with frequently alternating phases). Moreover, it is impossible to say which of the periods of the disease is more difficult, manic or depressive.
Bad when very bad
Those who have experienced real depression say that this is the worst thing that can happen in life. In this state, the whole world is seen in black, the mood is depressed, self-esteem drops, life loses its meaning. A person suffering from BAD in the depressive phase perceives his very existence as a chain of tragic mistakes, constantly blaming himself for all the troubles and sins, even those that do not even exist. In addition to mental suffering, physical ones also arise: a person even moves with difficulty, as if swimming against the current, it is difficult for him to perform the most familiar actions. In addition, he can feel tension throughout the body, experience various pain sensations. With an average degree of depression, people often complain of debilitating pain in the abdomen and other parts of the body. On this occasion, they turn to doctors, but the diagnosis cannot be made. And the daily pain continues to harass. Psychiatrists call this somatoform symptomatology. With severe depression, many have the so-called atrial depression. Patients complain of pain and heaviness in the chest, they say that "a stone lies on the heart." But even an in-depth examination does not reveal cardiac causes.
With an average degree of depression, people often complain of debilitating pain in the abdomen and other parts of the body. On this occasion, they turn to doctors, but the diagnosis cannot be made. And the daily pain continues to harass. Psychiatrists call this somatoform symptomatology. With severe depression, many have the so-called atrial depression. Patients complain of pain and heaviness in the chest, they say that "a stone lies on the heart." But even an in-depth examination does not reveal cardiac causes.
Often, with depression, patients (especially the elderly) complain of difficulty in thinking, memory impairment, they say that they have become stupid, they believe that they are developing dementia, they are afraid of “losing their mind”. In fact, affective disorders do not destroy the intellect. When treated with antidepressants, when the mood stabilizes, abilities are restored.
But the worst consequence of depression is suicide. Most suicide attempts are made in this state. Sometimes people in a very pronounced depression, believing that they have done something irreparable, and believing that the consequences of their actions can harm loved ones, decide on extended suicides, in which they settle scores not only with their lives, but also take their loved ones with them ( more often children).
Sometimes people in a very pronounced depression, believing that they have done something irreparable, and believing that the consequences of their actions can harm loved ones, decide on extended suicides, in which they settle scores not only with their lives, but also take their loved ones with them ( more often children).
Bad when too good
The manic stage of BAD is subjectively more pleasant. Patients are not just in a very good, but in a great mood: they love the whole world and themselves in it. The reflection in the mirror pleases, there is not the slightest doubt about one’s own talents and mind, there is more than enough strength and energy, a bonus is accelerated mental activity. Many in this stage sleep for an hour a day, but do not experience fatigue. Sometimes they don’t sleep for whole days - and at least they are cheerful, like an “energizer”. It seems to be great. But no. With mania, desires and new ideas arise too quickly, so a person grabs at each new business, but, as a rule, does not bring any to the end. So productivity at this stage is no more than during depression. But it would be nice if that was the only thing.
So productivity at this stage is no more than during depression. But it would be nice if that was the only thing.
The main danger of mania is that a person has no criticism at this moment, and he can do things that he will later regret very much. For example, he can give away all his property to others (sometimes to unfamiliar people or scammers who specifically use this state of his). Or, say, take out loans to go on a trip to the other side of the world, and take a bunch of friends with him. Maybe even steal something - for example, to make an expensive gift. Many patients at these moments enter into hasty intimate relationships, mistaking a chance meeting for the love of their life (and completely “forgetting” that family and children are waiting at home). Finally, often with mania, people, experiencing euphoria, ignore their severe somatic symptoms, as a result, they do not go to the doctor for a long time, and thus trigger a serious illness (pneumonia, for example). In addition, not all patients in the manic phase are "darlings. " Often they show unreasonable aggression if, for example, others do not agree with their "brilliant" advice. As a result of such “angry mania”, conflicts and even situations arise that require the intervention of law enforcement agencies and the hospitalization of the patient without his consent in a psychiatric hospital.
" Often they show unreasonable aggression if, for example, others do not agree with their "brilliant" advice. As a result of such “angry mania”, conflicts and even situations arise that require the intervention of law enforcement agencies and the hospitalization of the patient without his consent in a psychiatric hospital.
Good intentions…
The worst thing that relatives and friends of a person with bipolar disorder can do is ignore his problem, devalue suffering, while blaming the patient himself and appealing to his conscience. For example, they can call on a depressed person to “pull himself together, not become limp”, say that he is “mad with fat”, etc. A patient at the stage of mania is most often accused of immorality, irresponsibility, frivolity, promiscuity in relationships, etc. However, doing so is like blaming a person with diabetes for not being able to eat sweet cake, or a patient with heart failure for not running a marathon. BAD is a disease like many others. And she needs to be treated. The sooner you start the right therapy, the sooner you can stabilize the patient's condition and the better the further prognosis will be.
And she needs to be treated. The sooner you start the right therapy, the sooner you can stabilize the patient's condition and the better the further prognosis will be.
Psychiatrists don't bite
Despite the fact that recently people (especially young people) have ceased to be afraid to turn to psychiatrists, not everyone still decides to go to the doctor. Indeed, on the Internet in the public domain, you can find hundreds of questionnaires to test yourself for any mental disorder. And then, after reading various tips, you can also “cure”. Doctors strongly advise against doing this. The smallest harm of self-treatment is that it will not help or lead to incomplete improvement, but it can also worsen the condition. For example, inadequate intake of antidepressants in bipolar disorder can lead from a depressive phase into a severe manic state, from which it will then be difficult to get out. Only a psychiatrist (and not a psychologist, neurologist or doctor of any other somatic profile) can identify bipolar disorder and choose the right treatment. Treatment should be strictly individual, that is, the doctor selects it based on the characteristics of a particular patient and taking into account a specific moment in the course of the disease. The goal of therapy is not only to equalize the patient's mood, but also to prevent recurrence. In the treatment of bipolar disorder, the main role is played by drugs for stabilizing mood - mood stabilizers (lithium salts, some anticonvulsants (anticonvulsants) and antipsychotics of new generations). Modern drugs are much better tolerated than their predecessors, have fewer side effects, as they are designed for long-term use over many years. Against the background of their intake, women can even become pregnant and give birth. In depression, antidepressants are prescribed in exceptional cases, given the danger of changing the depressive stage to manic.
Treatment should be strictly individual, that is, the doctor selects it based on the characteristics of a particular patient and taking into account a specific moment in the course of the disease. The goal of therapy is not only to equalize the patient's mood, but also to prevent recurrence. In the treatment of bipolar disorder, the main role is played by drugs for stabilizing mood - mood stabilizers (lithium salts, some anticonvulsants (anticonvulsants) and antipsychotics of new generations). Modern drugs are much better tolerated than their predecessors, have fewer side effects, as they are designed for long-term use over many years. Against the background of their intake, women can even become pregnant and give birth. In depression, antidepressants are prescribed in exceptional cases, given the danger of changing the depressive stage to manic.
You won't be able to forget
The insidiousness of BAD is that this disease cannot be cured once and for all. But, alas, often, when the patient's mood can be balanced by medication and he begins to feel good (such a state - intermission - is completely indistinguishable from a state of complete health), he can stop taking the drugs. This is a big mistake that does not allow to achieve a stable result of treatment. Sometimes it is required to use medicines (necessarily under the supervision of a doctor) for several months, but more often for years (with periodic visits to the doctor). It is the long-term use of maintenance therapy individually selected by the doctor that allows patients to achieve a stable good condition and feel the joy of life for many years.
This is a big mistake that does not allow to achieve a stable result of treatment. Sometimes it is required to use medicines (necessarily under the supervision of a doctor) for several months, but more often for years (with periodic visits to the doctor). It is the long-term use of maintenance therapy individually selected by the doctor that allows patients to achieve a stable good condition and feel the joy of life for many years.
Link to publication: www.kiz.ru
Site embed code
More than 60 million people in the world suffer from bipolar affective disorder (BAD). The essence of the disease is that a person has alternating periods of altered mood throughout his life: from a state with a minus sign to a state with a plus sign. How and why is this happening?
Marina KINKULKINA, psychiatrist of the highest category, head of the department of psychiatry and narcology, director of the Institute of Electronic Medical Education, First Moscow State Medical University. I. M. Sechenova, Corresponding Member of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences
I. M. Sechenova, Corresponding Member of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences
Moreover, it is often not just about sadness or fun, as is often the case with emotional people, but about extreme degrees of either despair or euphoria. The change in these moods can take place both gradually and suddenly, and often for no apparent reason. This disease is attributed to Byron and Hemingway, Virginia Woolf and Edgar Poe, Van Gogh, Schumann, Vivien Leigh and many others. There is an assumption that even “our everything” suffered from a mild degree of BAD (contemporaries often mentioned mood swings) A. S. Pushkin. Modern stars - Catherine Zeta-Jones and Mel Gibson - openly admit to having this mental disorder. And rapper Kanye West even put the inscription on the cover of his album: "I hate being bipolar, it's amazing." A very accurate description of the essence of this disease.
Genetics does not solve everything
BAD affects both men and women, but the weaker sex - more often. As for the age of onset of the disease, this disorder can also appear in a teenager (especially if there is an appropriate heredity), and in an adult, and even in an elderly person. Everything is individual. The main risk factor is genetics, but a specific gene that would be responsible for the development of bipolar disorder has not been identified. This is a polygenic disorder, and it makes no sense to take genetic tests to find out how great the risk of getting sick is, because scientists still do not have a consensus on what specific combination of genes can lead to a violation. But even if there is a genetic predisposition, it is not certain that the disease will develop. This was proven by studies on identical twins, one of which developed bipolar disorder over the years, while the other did not. Accordingly, there must be some other predisposing moments. Science knows about some of them: life at the limit of possibilities with constant hands-on work, stress and chronic lack of sleep, as well as night shift work, frequent flights with a significant change in hourly flights and, of course, the use of psychoactive substances contribute to the development of the disease.
As for the age of onset of the disease, this disorder can also appear in a teenager (especially if there is an appropriate heredity), and in an adult, and even in an elderly person. Everything is individual. The main risk factor is genetics, but a specific gene that would be responsible for the development of bipolar disorder has not been identified. This is a polygenic disorder, and it makes no sense to take genetic tests to find out how great the risk of getting sick is, because scientists still do not have a consensus on what specific combination of genes can lead to a violation. But even if there is a genetic predisposition, it is not certain that the disease will develop. This was proven by studies on identical twins, one of which developed bipolar disorder over the years, while the other did not. Accordingly, there must be some other predisposing moments. Science knows about some of them: life at the limit of possibilities with constant hands-on work, stress and chronic lack of sleep, as well as night shift work, frequent flights with a significant change in hourly flights and, of course, the use of psychoactive substances contribute to the development of the disease. Therefore, they should be avoided. Scientists have yet to learn about other factors.
Therefore, they should be avoided. Scientists have yet to learn about other factors.
But not boring?
The number of people suffering from bipolar disorder among the population, according to various estimates, varies from fractions of one percent to several percent. Recently, psychiatrists note, the proportion of affective disorders has increased significantly, which can be explained by improved diagnostics. At first glance, the BAR does not look like something scary and dangerous. To ignorant people, this disorder even seems attractive - sometimes sad, sometimes fun, in general, you won’t get bored. In addition, being different from everyone else is now fashionable. And then, there is an opinion that people with BAD have higher intelligence and creative abilities than the “gray masses”. But even if this is so, then none of those who suffer from it will definitely call BAD a pleasant thing. It is especially difficult for those patients who do not seek medical help on time. Without treatment, both phases of bipolar disorder can last for months (although sometimes the disorder occurs with frequently alternating phases). Moreover, it is impossible to say which of the periods of the disease is more difficult, manic or depressive.
Without treatment, both phases of bipolar disorder can last for months (although sometimes the disorder occurs with frequently alternating phases). Moreover, it is impossible to say which of the periods of the disease is more difficult, manic or depressive.
Bad when very bad
Those who have experienced real depression say that this is the worst thing that can happen in life. In this state, the whole world is seen in black, the mood is depressed, self-esteem drops, life loses its meaning. A person suffering from BAD in the depressive phase perceives his very existence as a chain of tragic mistakes, constantly blaming himself for all the troubles and sins, even those that do not even exist. In addition to mental suffering, physical ones also arise: a person even moves with difficulty, as if swimming against the current, it is difficult for him to perform the most familiar actions. In addition, he can feel tension throughout the body, experience various pain sensations. With an average degree of depression, people often complain of debilitating pain in the abdomen and other parts of the body. On this occasion, they turn to doctors, but the diagnosis cannot be made. And the daily pain continues to harass. Psychiatrists call this somatoform symptomatology. With severe depression, many have the so-called atrial depression. Patients complain of pain and heaviness in the chest, they say that "a stone lies on the heart." But even an in-depth examination does not reveal cardiac causes.
With an average degree of depression, people often complain of debilitating pain in the abdomen and other parts of the body. On this occasion, they turn to doctors, but the diagnosis cannot be made. And the daily pain continues to harass. Psychiatrists call this somatoform symptomatology. With severe depression, many have the so-called atrial depression. Patients complain of pain and heaviness in the chest, they say that "a stone lies on the heart." But even an in-depth examination does not reveal cardiac causes.
Often, with depression, patients (especially the elderly) complain of difficulty in thinking, memory impairment, they say that they have become stupid, they believe that they are developing dementia, they are afraid of “losing their mind”. In fact, affective disorders do not destroy the intellect. When treated with antidepressants, when the mood stabilizes, abilities are restored.
But the worst consequence of depression is suicide. Most suicide attempts are made in this state. Sometimes people in a very pronounced depression, believing that they have done something irreparable, and believing that the consequences of their actions can harm loved ones, decide on extended suicides, in which they settle scores not only with their lives, but also take their loved ones with them ( more often children).
Sometimes people in a very pronounced depression, believing that they have done something irreparable, and believing that the consequences of their actions can harm loved ones, decide on extended suicides, in which they settle scores not only with their lives, but also take their loved ones with them ( more often children).
Bad when too good
The manic stage of BAD is subjectively more pleasant. Patients are not just in a very good, but in a great mood: they love the whole world and themselves in it. The reflection in the mirror pleases, there is not the slightest doubt about one’s own talents and mind, there is more than enough strength and energy, a bonus is accelerated mental activity. Many in this stage sleep for an hour a day, but do not experience fatigue. Sometimes they don’t sleep for whole days - and at least they are cheerful, like an “energizer”. It seems to be great. But no. With mania, desires and new ideas arise too quickly, so a person grabs at each new business, but, as a rule, does not bring any to the end. So productivity at this stage is no more than during depression. But it would be nice if that was the only thing.
So productivity at this stage is no more than during depression. But it would be nice if that was the only thing.
The main danger of mania is that a person has no criticism at this moment, and he can do things that he will later regret very much. For example, he can give away all his property to others (sometimes to unfamiliar people or scammers who specifically use this state of his). Or, say, take out loans to go on a trip to the other side of the world, and take a bunch of friends with him. Maybe even steal something - for example, to make an expensive gift. Many patients at these moments enter into hasty intimate relationships, mistaking a chance meeting for the love of their life (and completely “forgetting” that family and children are waiting at home). Finally, often with mania, people, experiencing euphoria, ignore their severe somatic symptoms, as a result, they do not go to the doctor for a long time, and thus trigger a serious illness (pneumonia, for example). In addition, not all patients in the manic phase are "darlings. " Often they show unreasonable aggression if, for example, others do not agree with their "brilliant" advice. As a result of such “angry mania”, conflicts and even situations arise that require the intervention of law enforcement agencies and the hospitalization of the patient without his consent in a psychiatric hospital.
" Often they show unreasonable aggression if, for example, others do not agree with their "brilliant" advice. As a result of such “angry mania”, conflicts and even situations arise that require the intervention of law enforcement agencies and the hospitalization of the patient without his consent in a psychiatric hospital.
Good intentions…
The worst thing that relatives and friends of a person with bipolar disorder can do is ignore his problem, devalue suffering, while blaming the patient himself and appealing to his conscience. For example, they can call on a depressed person to “pull himself together, not become limp”, say that he is “mad with fat”, etc. A patient at the stage of mania is most often accused of immorality, irresponsibility, frivolity, promiscuity in relationships, etc. However, doing so is like blaming a person with diabetes for not being able to eat sweet cake, or a patient with heart failure for not running a marathon. BAD is a disease like many others. And she needs to be treated. The sooner you start the right therapy, the sooner you can stabilize the patient's condition and the better the further prognosis will be.
And she needs to be treated. The sooner you start the right therapy, the sooner you can stabilize the patient's condition and the better the further prognosis will be.
Psychiatrists don't bite
Despite the fact that recently people (especially young people) have ceased to be afraid to turn to psychiatrists, not everyone still decides to go to the doctor. Indeed, on the Internet in the public domain, you can find hundreds of questionnaires to test yourself for any mental disorder. And then, after reading various tips, you can also “cure”. Doctors strongly advise against doing this. The smallest harm of self-treatment is that it will not help or lead to incomplete improvement, but it can also worsen the condition. For example, inadequate intake of antidepressants in bipolar disorder can lead from a depressive phase into a severe manic state, from which it will then be difficult to get out. Only a psychiatrist (and not a psychologist, neurologist or doctor of any other somatic profile) can identify bipolar disorder and choose the right treatment. Treatment should be strictly individual, that is, the doctor selects it based on the characteristics of a particular patient and taking into account a specific moment in the course of the disease. The goal of therapy is not only to equalize the patient's mood, but also to prevent recurrence. In the treatment of bipolar disorder, the main role is played by drugs for stabilizing mood - mood stabilizers (lithium salts, some anticonvulsants (anticonvulsants) and antipsychotics of new generations). Modern drugs are much better tolerated than their predecessors, have fewer side effects, as they are designed for long-term use over many years. Against the background of their intake, women can even become pregnant and give birth. In depression, antidepressants are prescribed in exceptional cases, given the danger of changing the depressive stage to manic.
Treatment should be strictly individual, that is, the doctor selects it based on the characteristics of a particular patient and taking into account a specific moment in the course of the disease. The goal of therapy is not only to equalize the patient's mood, but also to prevent recurrence. In the treatment of bipolar disorder, the main role is played by drugs for stabilizing mood - mood stabilizers (lithium salts, some anticonvulsants (anticonvulsants) and antipsychotics of new generations). Modern drugs are much better tolerated than their predecessors, have fewer side effects, as they are designed for long-term use over many years. Against the background of their intake, women can even become pregnant and give birth. In depression, antidepressants are prescribed in exceptional cases, given the danger of changing the depressive stage to manic.
You won't be able to forget
The insidiousness of BAD is that this disease cannot be cured once and for all. But, alas, often, when the patient's mood can be balanced by medication and he begins to feel good (such a state - intermission - is completely indistinguishable from a state of complete health), he can stop taking the drugs. This is a big mistake that does not allow to achieve a stable result of treatment. Sometimes it is required to use medicines (necessarily under the supervision of a doctor) for several months, but more often for years (with periodic visits to the doctor). It is the long-term use of maintenance therapy individually selected by the doctor that allows patients to achieve a stable good condition and feel the joy of life for many years.
This is a big mistake that does not allow to achieve a stable result of treatment. Sometimes it is required to use medicines (necessarily under the supervision of a doctor) for several months, but more often for years (with periodic visits to the doctor). It is the long-term use of maintenance therapy individually selected by the doctor that allows patients to achieve a stable good condition and feel the joy of life for many years.
Manic-depressive psychosis. How to recognize and can it be cured?
It is not always possible to distinguish a person with a sick psyche from a healthy one, because during periods of “enlightenment” they are quite ordinary people living the most ordinary life. But in the phase of exacerbation, the disease reveals all the secrets. Today we will talk about such a deviation as manic-depressive psychosis.
The concept of manic-depressive psychosis
The disease has many names - manic-depressive psychosis, MDP, bipolar personality disorder, manic-depressive syndrome, manic-depressive disorder, and in modern psychiatry it is referred to as bipolar affective disorder (BAD).
In its most general form, the term is interpreted as a mental disorder characterized by prolonged polar mood swings. A person can stay in a state of increased excitability and activity for several months - this is how a manic state manifests itself - or go into severe depression for the same period. There are also mixed states.
It is important to understand here that this is not just ordinary mood swings. For a bipolar person, it has extreme highs and lows, when a person is capable of reckless, and sometimes dangerous, actions.
According to the World Health Organization, almost 45 million inhabitants of the planet have TIR. Since the disease is detected at a fairly adult age, there are no accurate statistics on children yet.
Causes of pathology
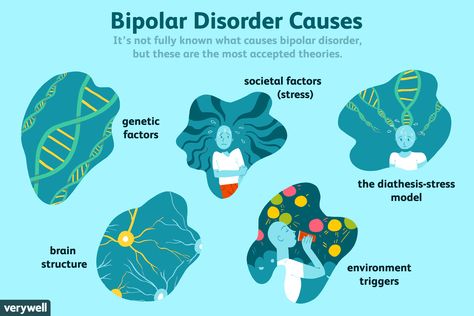
It has not yet been possible to find out the reasons due to which BAD occurs. However, this is the problem with most mental disorders. The main version is hereditary predisposition.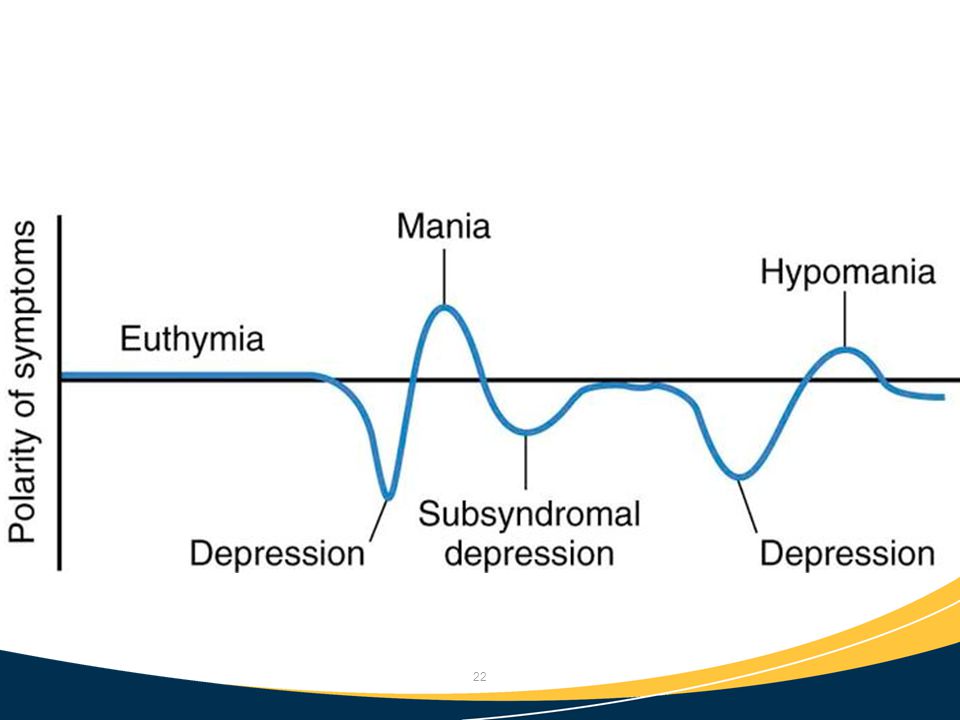
It is also believed that bipolar mental disorders have a complex etiology. What do the results of genetic, biological studies, the study of neuroendocrine structures, as well as a number of psychosocial theories say.
To date, there are no visible reasons for the development of TIR. Presumably, a violation can provoke any factor. For example, another medical condition or personality trait, such as:
- melancholic temperament;
- increased conscientiousness and various psychasthenic traits;
- anxiety, suspiciousness;
- emotional instability.
Note! In women, the risk of developing TIR increases during periods of hormonal changes. Especially those who already had various mental disorders.
Symptoms of disease
Symptoms of the disease depend on the phase in which the person is. There are three of them: manic, depressive and mixed.
Manic phase
The manic stage (episode) has a different degree of severity: from the mildest (hypomania) to very severe, when psychotic symptoms appear.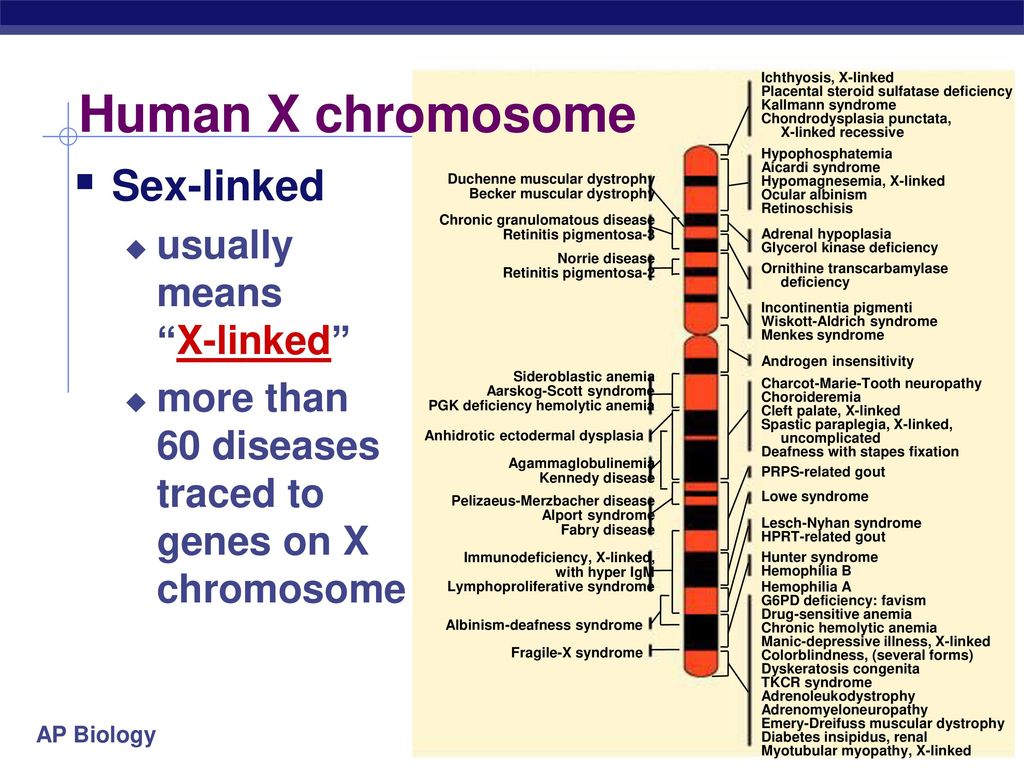 It is believed that hypomania sometimes even benefits the patient, because it makes him more productive and sociable.
It is believed that hypomania sometimes even benefits the patient, because it makes him more productive and sociable.
Symptoms:
- the classic manic triad - a very good mood, quick thinking, increased speech and motor activity.
- a lot of energy, grasping at several things at the same time, but soon give them up.
- a person is often distracted during conversations, can laugh out loud and shout, incoherent speech.
- due to the high speed of thinking, a person may not keep up with his own thoughts, so sometimes it seems that he is delusional.
Another variant of the manic phase is anger. It is characterized by strong irritability, aggressiveness and pickiness towards others.
Depressive phase
During this phase, the patient may experience suicidal ideation, so hospitalization is sometimes required.
Symptoms:
- endogenous depression - when a person is very upset for no reason.
- depressive triad - bad mood, slow thinking and motor speech activity.
- mood swings during the day - in the morning, people, as a rule, can experience melancholy and anxiety.
- lack of appetite, feeling that food has no taste, weight loss.
- psychomotor retardation.
- sometimes women miss their periods.
- the physical feeling of anguish is like a heaviness in the chest.
- decrease or complete disappearance of libido and maternal instinct.
- Protopopov's triad - tachycardia, dilated pupils and constipation.
- delusions, hallucinations (usually auditory).
Sometimes a non-standard variant of the depressive phase happens, when a person, on the contrary, has a great appetite and greatly increases the duration of sleep. In general, doctors distinguish the following options for the course of this period:
- simple depression - there is a classic depressive triad, there are no delusions and hallucinations.

- hypochondriacal depression - delirium with affective coloring, associated with anxiety about one's own health.
- delusional depression - passes very brightly with a feeling of anxiety and worries about the fate of humanity and the planet. For example, a “premonition” of a global cataclysm that will destroy all life.
- agitated depression - manifests itself as nervous excitement.
- anesthetic depression - when a person experiences absolutely no feelings for a long time.
Mixed phase
This is the third variant of the course of the disease, which has its own signs, and therefore stands out in a separate category. It combines the signs of the first two phases, lasting at least two weeks and quickly replacing each other. They appear bright enough.
Symptoms:
- insomnia;
- suicidal mood;
- poor appetite;
- various psychotic traits.
A vivid example of such a phase is a great mood against the background of a deep stupor.
Parasuicide - a demonstrative attempt to commit suicide or simply self-harm without the goal of ending life - occurs in almost half of cases with bipolar affective disorder. If your loved one shows such or similar desires, call our specialists by phone at any time of the day - they are in touch with you 24/7. Doctors will advise you on treatment, give practical advice on how to live with a “difficult” person and how to help him.
Features of bipolar disorder in women
A man and a woman have the same signs of bipolar, as well as suffer from it with the same frequency. However, the disease is characterized by a number of differences:
- in women, bipolarity appears later and, most often, begins with a depressive phase;
- women have more depressive phases than manic or mixed phases;
- the beginning of the phase, as a rule, coincides with hormonal changes;
- MDP increases the risk of developing alcoholism in women by about seven times.

Pay attention! If a woman has such a diagnosis, then the likelihood of developing an “attack” after childbirth increases significantly.
What causes TIR
While the causes of the disease are unknown, it is impossible to track the process of its formation. Recent studies lead scientists to hypothesize that biological factors play an important role here.
Another important point is genetics. Today's accumulated data allow us to determine the quantitative relationship between genetic and environmental factors in the development of bipolar disorder: heredity accounts for 70%, and the external environment - 30%. At the same time, the contribution of random environmental factors was equated to 8%, and family-wide - to 22%.
Classification and stages of development of BAD
Bipolar disorder in the International Classification of Diseases (ICD-10) is designated by the F31 code. Now, according to her, pathology is usually divided into three types:
| Type of mental disorder | How the disease manifests itself |
| bipolar course | when the patient has both manic and depressive phases, but there are intermissions between them - the so-called “light intervals”, when the person is quite normal |
| monopolar flow | when the patient shows only one phase, often depressive |
| continual flow | when there are no intermissions, and the phases alternate with each other |
The alternative to the ICD in America is the DSM. According to it, bipolar disorder is of types 1 and 2:
According to it, bipolar disorder is of types 1 and 2:
- BAD type I is characterized by the presence of manic and depressive episodes;
- type II bipolar disorder is characterized by the predominance of the depressive phase, the manic phase is either absent or there is hypomania.
Complications of manic-depressive psychosis
The worst complication for a bipolar person is suicide. In rare cases, it is conscious when the patient really wants it. Mostly we are talking about accidents associated with parasuicide. This may include an overdose of medications, too deep cuts and other self-harm, careless actions.
It is important to understand that on an emotional upsurge, that is, in a manic phase, a person practically does not feel danger and is not afraid of the consequences. He is full of energy, absolutely confident in himself and believes that he will succeed.
Depressive-manic psychosis deprives a person of the opportunity to analyze information, therefore such people are prone to risk and addictions - alcohol, drugs or gambling. They can spend all their savings on some trinkets or invest in a loss-making enterprise, take out a bad loan, or simply lose everything, up to mortgaging the property. A bipolar person is capable of committing a crime for the sake of interest or on a dare, driving around the city, violating the rules of the road, which will endanger not only himself, but also those around him.
They can spend all their savings on some trinkets or invest in a loss-making enterprise, take out a bad loan, or simply lose everything, up to mortgaging the property. A bipolar person is capable of committing a crime for the sake of interest or on a dare, driving around the city, violating the rules of the road, which will endanger not only himself, but also those around him.
Promiscuous sex can lead to sexually transmitted diseases or unwanted pregnancies.
The diagnosis exhausts them both mentally and physically. People suffer from their own actions, sinking into depression even more. Their immunity deteriorates, psychosomatic illnesses occur, and the quality of life decreases.
A separate problem is the inability to establish full communication with other people.
People with bipolar disorder can behave recklessly, so the support of loved ones is extremely important here. If you are unsure how to help, talk to your doctor. Remember that our doctors are in touch with you around the clock - at any time of the day or night you will receive a detailed consultation and you will be helped!
Diagnosis of manic-depressive psychosis
Manic depression as an official diagnosis is made only after the manifestation of at least two episodes of bipolar disorder, one of which must be manic or mixed.
A psychiatrist will diagnose and treat TIR. For a correct conclusion, it is necessary to collect complete information about the patient and his immediate family. Further special studies are required. For example, the degree of depression is determined by scales.
In the case of manic episodes, the doctor needs to be especially careful. Here it is important to exclude diseases similar in symptoms, external causes and the effect of the action of drugs.
TIR Treatment
The Russian Society of Psychiatrists recommends treating manic-depressive psychosis according to three stages:
- relief therapy - to eliminate symptoms and minimize side effects.
- maintenance therapy - strengthens the effect of the first stage of treatment.
- anti-relapse therapy - designed to prevent recurrence of episodes.
Psychotherapeutic methods
Psychotherapeutic measures must be carried out in combination with medications, which include antiepileptic drugs, antidepressants, tranquilizers, etc. Otherwise, there will be no effect. Today, there are special techniques for the treatment of bipolar affective disorder that help reduce interpersonal conflicts and regulate cyclical changes in various environmental factors.
Otherwise, there will be no effect. Today, there are special techniques for the treatment of bipolar affective disorder that help reduce interpersonal conflicts and regulate cyclical changes in various environmental factors.
In addition, cognitive-behavioral exercises are actively used in the treatment; individual, group, and family forms of psychotherapy to reduce the risk of relapse; and self-monitoring sheets to monitor mood swings.
Important! Some medical institutions conduct special educational programs for their patients, where they are told about the disease, explain its features and methods of treatment. Awareness calms a sick person and helps to form the right attitude towards what is happening to him.
Disease prognosis
The prognosis for manic-depressive psychosis can be different, it all depends on the individual characteristics of the disease. Outpatient treatment is enough for someone, hospitalization is required for someone, and in some cases the pathology is so strong that they will have to apply for disability.
According to WHO estimates, bipolar disorder is the 12th leading cause of disability. It overtook even asthma.
However, a well-designed treatment regimen can significantly improve the patient's quality of life. It is only worth remembering that it will not be possible to completely get rid of the diagnosis - at the moment it is incurable.
FAQ
Bipolar Disorder - What is it?
+
Bipolar affective disorder of the brain or manic-depressive psychosis is a psychiatric disorder characterized by prolonged extreme mood swings.
What is circular psychosis?
+
This is the former name for manic-depressive psychosis, and now bipolar affective disorder.
How to live with bipolar disorder in women?
+
Manic-depressive psychosis is much more common in women than in men. However, the clinical picture is relatively similar, with the only major difference being that the depressive phase predominates in the former.