Help with binge eating disorder
Binge-eating disorder - Diagnosis and treatment
Diagnosis
To diagnose binge-eating disorder, your medical care provider may recommend a psychological evaluation, including discussion of your eating habits.
Your medical care provider also may want you to have other tests to check for health consequences of binge-eating disorder, such as high cholesterol, high blood pressure, heart problems, diabetes, GERD and some sleep-related breathing disorders. These tests may include:
- A physical exam
- Blood and urine tests
- A sleep disorder center consultation
More Information
- Urinalysis
Treatment
The goals for treatment of binge-eating disorder are to reduce eating binges and achieve healthy eating habits. Because binge eating can be so entwined with shame, poor self-image and other negative emotions, treatment may also address these and any other mental health issues, such as depression. By getting help for binge eating, you can learn how to feel more in control of your eating.
Psychotherapy
Whether in individual or group sessions, psychotherapy (also called talk therapy) can help teach you how to exchange unhealthy habits for healthy ones and reduce bingeing episodes. Examples of psychotherapy include:
- Cognitive behavioral therapy (CBT). CBT may help you cope better with issues that can trigger binge-eating episodes, such as negative feelings about your body or a depressed mood. It may also give you a better sense of control over your behavior and help you regulate eating patterns.
- Interpersonal psychotherapy. This type of therapy focuses on your relationships with other people. The goal is to improve your interpersonal skills — how you relate to others, including family, friends and co-workers. This may help reduce binge eating that's triggered by problematic relationships and unhealthy communication skills.
- Dialectical behavior therapy. This form of therapy can help you learn behavioral skills to help you tolerate stress, regulate your emotions and improve your relationships with others, all of which can reduce the desire to binge eat.

Medications
Lisdexamfetamine dimesylate (Vyvanse), a drug for attention-deficit hyperactivity disorder, is the first FDA-approved medication to treat moderate to severe binge-eating disorder in adults. A stimulant, Vyvanse can be habit-forming and abused. Common side effects include a dry mouth and insomnia, but more-serious side effects can occur.
Several other types of medication may help reduce symptoms. Examples include:
- Topiramate (Topamax), an anticonvulsant. Normally used to control seizures, topiramate has also been found to reduce binge-eating episodes. However, there are side effects, such as dizziness, nervousness, sleepiness and trouble concentrating, so discuss the risks and benefits with your medical care provider.
- Antidepressants. Antidepressants may reduce binge-eating. It's not clear how these can reduce binge eating, but it may relate to how they affect certain brain chemicals associated with mood.

While these medications can be helpful in controlling binge-eating episodes, they may not have much impact on weight reduction.
Behavioral weight-loss programs
Many people with binge-eating disorder have a history of failed attempts to lose weight on their own. However, weight-loss programs typically aren't recommended until the binge-eating disorder is treated, because dieting may trigger more binge-eating episodes, making weight loss less successful.
When appropriate, weight-loss programs are generally done under medical supervision to ensure that your nutritional requirements are met. Weight-loss programs that address binge triggers can be especially helpful when you're also getting cognitive behavioral therapy.
More Information
- Cognitive behavioral therapy
- Psychotherapy
Request an Appointment at Mayo Clinic
Lifestyle and home remedies
Typically, treating binge-eating disorder on your own isn't effective. But in addition to professional help, you can take these self-care steps to reinforce your treatment plan:
But in addition to professional help, you can take these self-care steps to reinforce your treatment plan:
- Stick to your treatment. Don't skip therapy sessions. If you have a meal plan, do your best to stick to it and don't let setbacks derail your overall efforts.
- Avoid dieting, unless it's supervised. Trying to diet can trigger more binge episodes, leading to a vicious cycle that's hard to break. Talk with your medical care provider about appropriate weight management strategies for you — don't diet unless it's recommended for your eating disorder treatment and supervised by your medical care provider.
- Eat breakfast. Many people with binge-eating disorder skip breakfast. But, if you eat breakfast, you may be less prone to eating higher calorie meals later in the day.
- Arrange your environment. Availability of certain foods can trigger binges for some people. Keep tempting binge foods out of your home or limit your exposure to those foods as best you can.

- Get the right nutrients. Just because you may be eating a lot during binges doesn't mean you're eating the kinds of food that supply all the essential nutrients. Ask your medical care provider if you need to adjust your diet to provide essential vitamins and minerals.
- Stay connected. Don't isolate yourself from caring family members and friends who want to see you get healthy. Understand that they have your best interests at heart.
- Get active. Ask your medical care provider what kind of physical activity is appropriate for you, especially if you have health problems related to being overweight.
Alternative medicine
Most dietary supplements and herbal products designed to suppress the appetite or aid in weight loss are ineffective and may be misused by people with eating disorders. And natural doesn't always mean safe. Weight-loss supplements or herbs can have serious side effects and dangerously interact with other medications.
If you use dietary supplements or herbs, discuss the potential risks with your medical care provider.
Coping and support
Living with an eating disorder is especially difficult because you have to deal with food on a daily basis. Here are some tips to help you cope:
- Ease up on yourself. Don't buy into your own self-criticism.
- Identify situations that may trigger destructive eating behavior so you can develop a plan of action to deal with them.
- Look for positive role models who can help lift your self-esteem. Remind yourself that the ultrathin models or actresses showcased in women's magazines often don't represent healthy, realistic bodies.
- Try to find a trusted relative or friend whom you can talk with about what's going on.
- Try to find someone who can be your partner in the battle against binge eating — someone you can call on for support instead of bingeing.

- Find healthy ways to nurture yourself by doing something just for fun or to relax, such as yoga, meditation or simply a walk.
- Consider journaling about your feelings and behaviors. Journaling can make you more aware of your feelings and actions, and how they're related.
Get support
If you have binge-eating disorder, you and your family may find support groups helpful for encouragement, hope and advice on coping. Support group members can understand what you're going through because they've been there themselves. Ask your medical care provider if he or she knows of a group in your area.
Preparing for your appointment
Treatment of binge-eating disorder may require a team approach that includes doctors and other medical care providers, mental health professionals and dietitians with experience in eating disorders.
Here's some information to help you get ready for your appointments. Ask a family member or friend to go with you, if possible, to help you remember key points and give a fuller picture of the situation.
What you can do
Before your appointment make a list of:
- Symptoms you're experiencing, including any that may seem unrelated to the reason for your appointment
- Key personal information, including any major stresses or recent life changes
- All medications you're taking, as well as any herbs, vitamins or other supplements, and their dosages
- A typical day's eating, which can help your medical care provider or mental health professional understand your eating habits
Questions to ask your medical care provider or mental health professional include:
- What treatments are available, and which do you recommend?
- If medication is a part of treatment, is a generic drug available?
- Are there any brochures or other printed material I can have? What websites do you recommend?
Don't hesitate to ask other questions during your appointment.
What to expect from your doctor
Your medical care provider or mental health professional is likely to ask you a number of questions, such as:
- What does your typical daily food intake look like?
- Do you eat unusually large amounts of food or until you're uncomfortably full?
- Do you feel your eating is out of control?
- Have you tried to lose weight? If so, how?
- Do you think about food often?
- Do you eat even when you're full or not hungry?
- Do you ever eat in secret?
- Do you feel depressed, ashamed or guilty about your eating?
- Do you ever make yourself vomit to get rid of calories?
- Are you concerned about your weight?
- Do you exercise? How often?
Your medical care provider or mental health professional will ask additional questions based on your responses, symptoms and needs. Preparing and anticipating questions will help you make the most of your appointment time.
By Mayo Clinic Staff
Related
Associated Procedures
Products & Services
Binge eating disorder | Office on Women's Health
Binge eating disorder is the most common type of eating disorder in the United States. People with binge eating disorder often feel out of control and eat a large amount of food at one time (called a binge). Unlike other eating disorders, people who have binge eating disorder do not throw up the food or exercise too much. Binge eating disorder is a serious health problem, but people with binge eating disorder can get better with treatment.
What is binge eating disorder?
Binge eating disorder is a type of eating disorder. Eating disorders are mental health problems that cause extreme and dangerous eating behaviors. These extreme eating behaviors cause other serious health problems and sometimes death. Some eating disorders also involve extreme exercise.
According to the American Psychiatric Association, women with binge eating disorder feel out of control and eat too much (binge), at least once a week for at least three months. During binges women with binge eating disorder usually eat faster than normal, eat until they are uncomfortable, eat when they are not physically hungry, and feel embarrassed, disgusted, or depressed because of the binges. Women with this type of eating disorder may be overweight or obese.
During binges women with binge eating disorder usually eat faster than normal, eat until they are uncomfortable, eat when they are not physically hungry, and feel embarrassed, disgusted, or depressed because of the binges. Women with this type of eating disorder may be overweight or obese.
What is the difference between binge eating disorder and other eating disorders?
Women with eating disorders, such as binge eating disorder, bulimia, and anorexia, have a mental health condition that affects how they eat, and sometimes how they exercise. These eating disorders threaten their health.
Unlike people with anorexia or bulimia, people with binge eating disorder do not throw up their food, exercise a lot, or starve themselves. People with binge eating disorder are often overweight or obese. But not all people with binge eating disorder are overweight, and being overweight does not always mean you have binge eating disorder.
It is possible to have more than one eating disorder in your lifetime. Regardless of what type of eating disorder you may have, you can get better with treatment.
Regardless of what type of eating disorder you may have, you can get better with treatment.
Who is at risk for binge eating disorder?
Binge eating disorder affects more than 3% of women in the United States. More than half of people with binge eating disorder are women.1
Binge eating disorder affects women of all races and ethnicities. It is the most common eating disorder among Hispanic, Asian-American, and African-American women.2,3,4
Some women may be more at risk for binge eating disorder.
- Women and girls who diet often are 12 times more likely to binge eat than women and girls who do not diet.5
- Binge eating disorder affects more young and middle-aged women than older women. On average, women develop binge eating disorder in their early to mid-20s.6 But eating disorders are happening more often in older women. In one study, 13% of American women over 50 had signs of an eating disorder.
 7
7
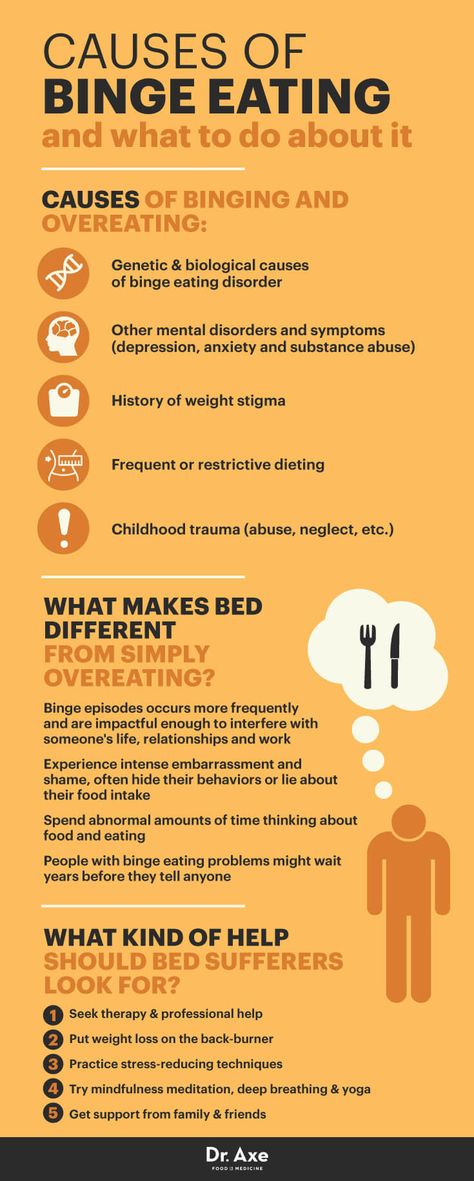
What are the symptoms of binge eating disorder?
It can be difficult to tell whether someone has binge eating disorder. Many women with binge eating disorder hide their behavior because they are embarrassed.
You may have binge eating disorder if, for at least once a week over the past three months, you have binged. Binge eating disorder means you have at least three of these symptoms while binging:8
- Eating faster than normal
- Eating until uncomfortably full
- Eating large amounts of food when not hungry
- Eating alone because of embarrassment
- Feeling disgusted, depressed, or guilty afterward
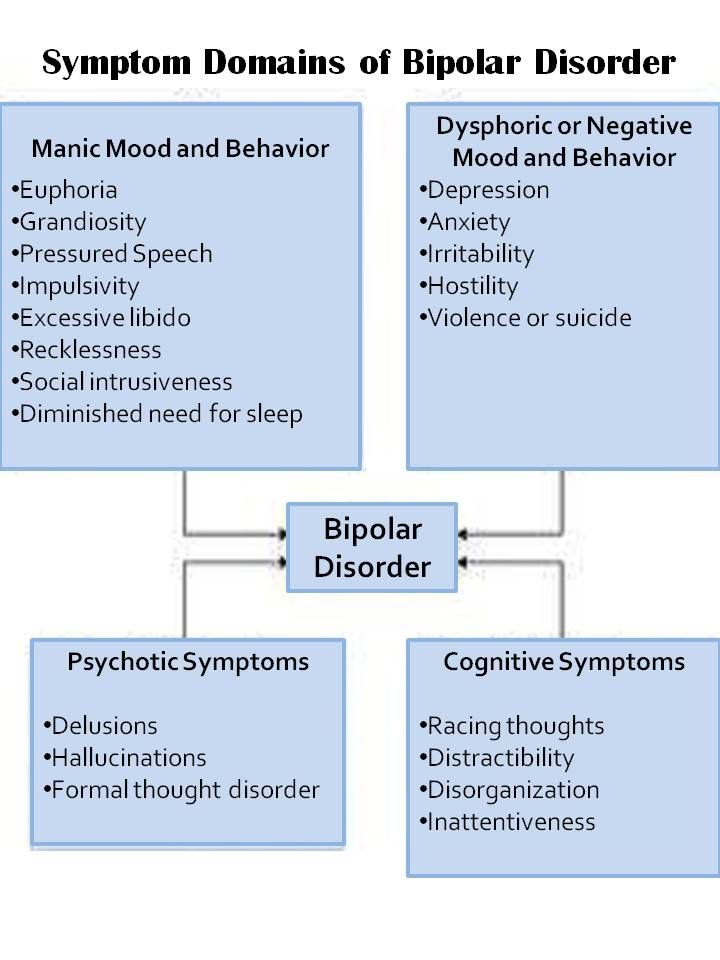
People with binge eating disorder may also have other mental health problems, such as depression, anxiety, or substance abuse.
What causes binge eating disorder?
Researchers are not sure exactly what causes binge eating disorder and other eating disorders. Researchers are finding that eating disorders might happen because of a complex combination of genetic, biological, behavioral, psychological, and social factors may be the cause. This combination includes having specific genes, a person's biology, body image and self-esteem, social experiences, family health history, and sometimes other mental health illnesses.
This combination includes having specific genes, a person's biology, body image and self-esteem, social experiences, family health history, and sometimes other mental health illnesses.
Studies suggest that people with binge eating disorder may use overeating as a way to deal with anger, sadness, boredom, anxiety, or stress.9,10
Researchers are studying how changing levels of brain chemicals may affect eating habits. Neuroimaging, or pictures of the brain, may lead to a better understanding of binge eating disorder.11
Learn more about current research and read peer-reviewed articles on binge eating disorder.
How does binge eating disorder affect a woman's health?
Many, but not all, women with binge eating disorder are overweight or obese. Obesity raises your risk for many serious health problems:12
- Type 2 diabetes
- Heart disease
- High blood pressure
- High cholesterol
- Gallbladder disease
- Certain types of cancer, including breast, endometrial (a type of uterine cancer), colorectal, kidney, esophageal, pancreatic, thyroid, and gallbladder cancer13
- Problems with your menstrual cycle, including preventing ovulation, which can make it harder to get pregnant
People with binge eating disorder often have other serious mental health disorders such as depression, anxiety, or problems with substance use.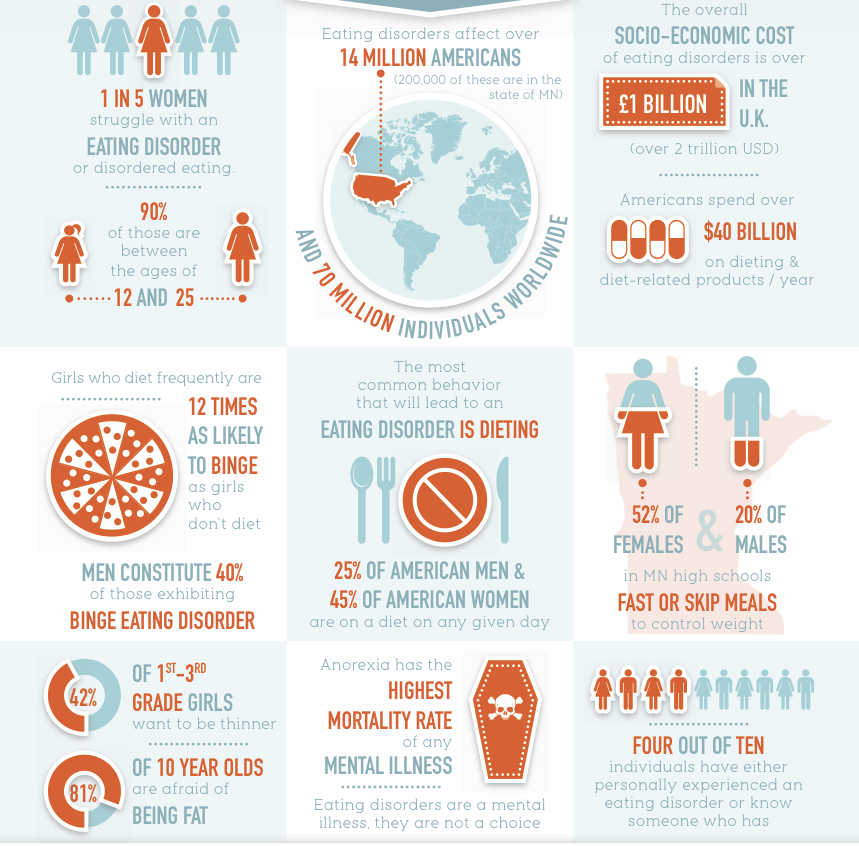 These problems can seriously affect a woman's everyday life and can be treated.
These problems can seriously affect a woman's everyday life and can be treated.
How is binge eating disorder diagnosed?
Your doctor or nurse will ask you questions about your symptoms and medical history. It may be difficult to talk to a doctor or nurse about secret eating behaviors. But doctors and nurses want to help you be healthy. Being honest about your eating behaviors with a doctor or nurse is a good way to ask for help.
Your doctor may also do blood, urine, or other tests for other health problems, such as heart problems or gallbladder disease, that can be caused by binge eating disorder.
How is binge eating disorder treated?
Your doctor may refer you to a team of doctors, nutritionists, and therapists who will work to help you get better.
Treatment plans may include one or more of the following:
- Psychotherapy. Sometimes called "talk therapy," psychotherapy is counseling to help you change any harmful thoughts or behaviors.
 This therapy may focus on the importance of talking about your feelings and how they affect what you do. For example, you might talk about how stress triggers a binge. You may work one-on-one with a therapist or in a group with others who have binge eating disorder.
This therapy may focus on the importance of talking about your feelings and how they affect what you do. For example, you might talk about how stress triggers a binge. You may work one-on-one with a therapist or in a group with others who have binge eating disorder. - Nutritional counseling. A registered dietitian can help you eat in a healthier way.
- Medicine, such as appetite suppressants or antidepressants prescribed by a doctor. Antidepressants may help some girls and women with binge eating disorder who also have anxiety or depression.
Most girls and women do get better with treatment and are able to eat in healthy ways again.14 Some may get better after the first treatment. Others get well but may relapse and need treatment again.
How does binge eating disorder affect pregnancy?
Binge eating disorder can cause problems getting pregnant and during pregnancy, including having an infant that is large-for-gestational-age. 15 Pregnancy can also trigger binge eating disorder.
15 Pregnancy can also trigger binge eating disorder.
Obesity raises the level of the hormone estrogen in your body. Higher levels of estrogen can stop you from ovulating, or releasing an egg from the ovary. This can make it more difficult to get pregnant. However, if you do not want to have children right now and have sex, you should use birth control.
Overweight or obesity may also cause problems during pregnancy. Overweight and obesity raises your risk for:
- Gestational hypertension (high blood pressure during pregnancy) and preeclampsia (high blood pressure and kidney problems during pregnancy). If not controlled, both problems can threaten the life of the mother and the baby.
- Gestational diabetes (diabetes that starts during pregnancy). If not controlled, gestational diabetes can cause you to have a large baby. This raises your risk for a C-section.16
Pregnancy can raise the risk for binge eating disorder in women who are at higher risk for eating disorders. In one study, almost half of the women with binge eating disorder got the condition during pregnancy. The research suggests that binge eating during pregnancy may be caused by:17
In one study, almost half of the women with binge eating disorder got the condition during pregnancy. The research suggests that binge eating during pregnancy may be caused by:17
- Worry over pregnancy weight gain. Women may binge because they feel a loss of control over their bodies because of the pregnancy weight.
- Greater stress during pregnancy
- Depression
- History of smoking and alcohol abuse
- Lack of social support
After pregnancy, postpartum depression and weight from pregnancy can trigger binge eating disorder in women with a history of binge eating. Women with binge eating disorder before pregnancy often gain more weight during pregnancy than women without an eating disorder. Researchers think that weight gain during pregnancy may cause some women who had binge eating disorder before pregnancy to binge eat during pregnancy.18
If I had an eating disorder in the past, can I still get pregnant?
Yes. Women who have recovered from binge eating disorder, are at a healthy weight, and have normal menstrual cycles have a better chance of getting pregnant and having a safe and healthy pregnancy.
Women who have recovered from binge eating disorder, are at a healthy weight, and have normal menstrual cycles have a better chance of getting pregnant and having a safe and healthy pregnancy.
Tell your doctor if you had an eating disorder in the past and are trying to become pregnant.
If I take medicine to treat binge eating disorder, can I breastfeed my baby?
Maybe. Some medicines used to treat binge eating disorder can pass through breastmilk. Certain antidepressants can be used safely during breastfeeding.
Talk to your doctor to find out what medicine works best for you. Learn more about medicines and breastfeeding in our Breastfeeding section. You can also enter a medicine into the LactMed® database to find out if the medicine passes through breastmilk and about any possible side effects for your nursing baby.
Did we answer your question about binge eating disorder?
For more information about binge eating disorder, call the OWH Helpline at 1-800-994-9662 or contact the following organizations:
- MentalHealth.
 gov
gov - National Institute of Mental Health, NIH, HHS
Phone Number: 866-615-6464 - Substance Abuse and Mental Health Services Administration (SAMHSA) Treatment Referral Helpline
Phone Number: 1-877-SAMHSA7 (1-877-726-4727) - Weight-control Information Network, NIDDK, NIH, HHS
Phone Number: 877-946-4627 - American Psychological Association
Phone Number: 800-374-2721 - National Eating Disorders Association (NEDA)
Phone Number: 800-931-2237 - The Obesity Society
Phone Number: 301-563-6526
Sources
- Hudson, J.I., Hiripi, E., Pope, H.G., Jr., Kessler, R.C. (2007). The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biological Psychiatry; 61: 348-58.
- Nicdao, E.G., Hong, S., Takeuchi, D.T. (2007). Prevalence and correlates of eating disorders among Asian Americans: results from the National Latino and Asian American Study. International Journal of Eating Disorders; 40: S22-S26.

- Alegria, M., Woo, M., Cao, Z., Torres, M., Meng, X.-l., Streigel-Moore, R. (2007). Prevalence and correlates of eating disorders in Latinos in the United States. International Journal of Eating Disorders; 40: S15-S21.
- Marques, L., Alegria, M., Becker, A.E., Chen, C., Fang, A., Chosak, A., et al. (2011). Comparative Prevalence, Correlates of Impairment, and Service Utilization for Eating Disorders across U.S. Ethnic Groups: Implications for Reducing Ethnic Disparities in Health Care Access for Eating Disorders. International Journal of Eating Disorders; 44(5): 412-420.
- Neumark-Sztainer, D. (2005). I'm, Like, SO Fat!; Helping Your Teen Make Healthy Choices about Eating and Exercise in a Weight-Obsessed World. New York: Guilford Press.
- Berkman, N. D., Brownley, K. A., Peat, C. M., et al. (2015). Management and Outcomes of Binge-Eating Disorder. Comparative Effectiveness Reviews, No. 160. Agency for Healthcare Research and Quality (US), Rockville , MD.

- Gagne, D.A., Von Holle, A., Brownley, K.A., Runfola, C.D., Hofmeier, S., Branch, K.E., et al. (2012). Eating disorder symptoms and weight and shape concerns in a large web-based convenience sample of women ages 50 and above: Results of the gender and body image (GABI) study. International Journal of Eating Disorders; 45(7): 832-844.
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Association Publishing; 2013.
- Joke, V., Vansteenkiste, M., Soenens, B., Boone, L., Mouratidis, A. (2013). Daily ups and downs in women's binge eating symptoms: The role of basic psychological needs, general self-control, and emotional eating. Journal of Social and Clinical Psychology; 32(3): 335-61.
- Kelly, N.R., Lydecker, J.A., Mazzeo, S.E. (2012). Positive cognitive coping strategies and binge eating in college women. Eating Behaviors; 13(3): 289-92.

- Rikani, A.A., Choudhry, Z., Choudhry, A.M., Ikram, H., Asghar, M.W., Kajal, D., et al. (2013). A critique of the literature on etiology of eating disorders. Annals of Neurosciences; 20(4): 157-161.
- National Heart, Lung, and Blood Institute. (2013). What Are the Health Risks of Overweight and Obesity?
- National Cancer Institute. (2012). Obesity and Cancer Risk.
- Fairburn, C. G., Cooper, Z., Doll, H. A., et al. (2000). The natural course of bulimia nervosa and binge eating disorder in young women. Arch Gen Psychiatry, 57(7), 659–665.
- Charbonneau, K.D., Seabrook, J.A. (2019). Adverse Birth Outcomes Associated with Types of Eating Disorders: A Review. Canadian Journal of Dietetic Practice and Research; 80(3): 131-136.
- Eunice Kennedy Shriver National Institute of Child Health and Human Development. (2012). NIH Obesity Research Featured in HBO's The Weight of the Nation.
- Berg, C.K., Torgersen, L.
 , Von Holle, A., Hamer, A., Bulik, C.M., Reichborn-Kjennerud, T. (2011). Factors associated with binge eating disorder in pregnancy. International Journal of Eating Disorders; 44(2): 124-133.
, Von Holle, A., Hamer, A., Bulik, C.M., Reichborn-Kjennerud, T. (2011). Factors associated with binge eating disorder in pregnancy. International Journal of Eating Disorders; 44(2): 124-133. - Knoph, C., Von Holle, A., Zerwas, S., Torgersen, L., Tambs, K., et al. (2013). Course and predictors of maternal eating disorders in the postpartum period. International Journal of Eating Disorders; 46(4): 355-368.
All material contained on these pages are free of copyright restrictions and maybe copied, reproduced, or duplicated without permission of the Office on Women’s Health in the U.S. Department of Health and Human Services. Citation of the source is appreciated.
Page last updated: February 22, 2022
Medical treatment of compulsive overeating by a psychologist, treat the disease by a psychotherapist
Sometimes it happens that delicious food, appetizing appearance of dishes cause a person to get up from the table with a feeling of a full stomach. If such situations occur rarely, overeating can be controlled, then there is nothing to worry about. If we are talking about causeless and uncontrolled appetite, which is preceded by stress or negative emotions, then we can suspect a dangerous eating disorder - compulsive or uncontrolled overeating. It is important not to miss the moment and turn to a psychotherapist in time.
If such situations occur rarely, overeating can be controlled, then there is nothing to worry about. If we are talking about causeless and uncontrolled appetite, which is preceded by stress or negative emotions, then we can suspect a dangerous eating disorder - compulsive or uncontrolled overeating. It is important not to miss the moment and turn to a psychotherapist in time.
Article content:
- Disease description
- Causes
- Psychological aspect of the problem
- Methods of psychotherapy in the treatment of illness
- Possible complications
Description of the disease
Compulsive overeating (CP) is a dangerous pathological condition. The patient is unable to control his appetite due to stress. The essence and nature of a compulsive disease is well explained by its second name - psychogenic overeating, since the causes of the development of an eating disorder should be sought not in the physiological, but in the mental sphere.
Any stressful situation can provoke a painful condition: the loss of a loved one, the loss of keys, a conversation with superiors in a raised tone, and other unpleasant situations.
Bouts of psychogenic overeating may recur from time to time. As with other eating disorders, the patient considers himself healthy. The exception is excess weight, which accompanies psychogenic overeating. Uncontrolled appetite has clear differences from other foodborne illnesses:
- if during anorexia the patient ceases to adequately perceive his own body, then with compulsive overeating the problem of excess weight becomes obvious and is the root cause of contacting a psychologist, psychotherapist, other doctors;
- The binge patient usually does not seek to get rid of food by inducing artificial vomiting, while the symptoms of bulimia are characterized by obligatory cleansing procedures, which the patient cannot refuse.
Causes of occurrence
Normal physiological need - to eat exactly when there is a feeling of hunger. If food intake is reduced to nervous chewing, no attention is paid to the amount eaten, it is worth considering that it is bulimia or uncontrolled overeating that can cause increased weight, the appearance of extra centimeters in volume.
If food intake is reduced to nervous chewing, no attention is paid to the amount eaten, it is worth considering that it is bulimia or uncontrolled overeating that can cause increased weight, the appearance of extra centimeters in volume.
Physiological factors can provoke compulsive overeating - dysfunction of the hypothalamus and genetic predisposition. Genetic scientists have identified three genes whose presence in the genetic code leads to obesity and can provoke the development of an eating disorder.
The psychological aspect of the problem of psychogenic overeating
Physiological and genetic causes may be a consequence of the development of an eating disorder, but the psyche plays a central role.
Leading psychotherapists in describing clinical cases of compulsive overeating note that the onset of the disease is preceded by negative life events. Such stress can be caused by social and physiological factors.
In order to understand whether you have a problem or whether you need the help of a psychotherapist, you should honestly answer a number of questions.
- Have you noticed that your diet is difficult to control?
- all your thoughts are related to food?
- Do you prefer to eat alone?
- Do you tend to overeat when stressed out, distracted from current problems?
- Do you experience guilt that affects your enjoyment of eating?
- How often do you start eating without feeling hungry?
- Do you find it difficult to refuse food if you are treated?
If you answered yes to 4 or more questions, it makes sense to contact a medical institution for advice and clarification of the causes of nutritional problems.
Methods of psychotherapy in the treatment of illness
The solution to the fight against food addiction is to seek help from a specialist. Only a psychologist is able to help find the causes of binge eating disorder and form a healthy model of dealing with stress.
The Center for the Study of Eating Disorders uses the latest psychotherapy techniques accepted in the international medical community.
Depending on the severity of the condition, a treatment algorithm is selected. It can be done on an outpatient or inpatient basis under the supervision of a psychotherapist. The following areas of psychotherapy are used to treat patients with compulsive psychogenic overeating, bulimia, anorexia and other eating disorders:
- CBT - cognitive behavioral therapy;
- DBT - Dialectical Behavioral Psychotherapy;
- FBT - Family Involved Therapy.
All methods have scientifically proven effectiveness, are actively used in practice by psychotherapists and other doctors of "CIRPP" in the fight against overeating.
Family Therapy
Successful Family Psychological Therapy, which was developed for the treatment of patients with eating disorders by the leading specialists of the Maudsley Clinic.
A multi-family group has been organized in CIRP, in which not only patients, but also their relatives, as co-dependent persons, undergo therapy. In the course of group therapy, the psychotherapist helps to jointly develop the right adaptation tactics, build the right behavior model, and provides the necessary support to parents whose children suffer from eating disorders.
Cognitive behavioral therapy
The program is aimed at finding the causes of eating disorders (bulimia, anorexia, compulsive uncontrolled overeating, etc.). It is important to find out the root cause of the disease, this will help in choosing the right tactics.
DBT - Dialectical Behavior Therapy
The use of Dialectical Behavior Therapy has a positive effect in the treatment of patients with compulsive overeating. The method is aimed at finding new ways to deal with stress, teaching effective emotional regulation techniques that are not related to eating or deliberately refusing it.
At the end of the treatment phase, the patient will be able to painlessly give up destructive ways of dealing with stress, strict weight control and dietary regimens. Bouts of uncontrolled overeating will be left behind.
Psychologists of "CIRPP" use the latest methods of working with people suffering from eating disorders, psychogenic overeating. In addition to providing basic medication, resuscitation, developing an individual diet, the DBT program includes the work of online psychotherapy groups, art therapy, dance therapy led by a psychotherapist, and other eating behavior adjustment programs.
Possible complications
Late treatment of an eating disorder can adversely affect the condition of a patient suffering from regular overeating. If there is no treatment, then there is a high probability of developing other complications:
- decrease or increase in blood pressure;
- aggressive or lethargic behaviour;
- metabolic disorder;
- obesity;
- depression;
- alcohol or drug addiction;
- diseases of the cardiovascular system;
- type 2 diabetes and others.

Gradually, complications can become chronic, which reduces the chances of a full recovery. It is not difficult to avoid such a scenario - it is enough to be attentive to your own health, pay attention to alarming symptoms and consult a doctor in time.
Getting help from a psychologist, nutritionist or psychotherapist is easy: sign up for an initial medical consultation by calling +7(499) 703-20-51 or through the online form.
Author: Maksim Borisovich Sologub
Head Physician of TsIRPP
psychiatrist, psychotherapist.
signs, causes and treatment. Test
Many people already know about anorexia nervosa and bulimia. To this list of common eating disorders, another one has been added - compulsive overeating. It has recently been included in the updated International Classification of Diseases (ICD-11).
How compulsive overeating differs from ordinary binge eating, why it is dangerous to seize your emotions and how to cope with the disease, said Tatiana Romanovskaya, an assistant at the Department of Psychiatry with Medical Psychology at Belarusian State Medical University, a member of the Belarusian Psychiatric Association .
Compulsive overeating
How does the disease manifest itself?
Compulsive overeating is an attack in which a large amount of food is consumed in a relatively short period of time and there is a feeling of loss of control. After an attack, which can sometimes last all day, a person feels guilty, dissatisfied with himself. Such behavior can be considered a disorder if it is repeated at least twice a week for several months.
Binge eating occurs in 8-10% of overweight people and 25-50% of those seeking weight loss help. Distinguish between hedonic and compulsive overeating. With a hedonistic person, he simply loves to eat, the process of overeating is a pleasure and only sometimes a slight pangs of conscience: he ate a frying pan of fried potatoes - "it's okay, I'll lose weight tomorrow." And with compulsive overeating, it is difficult to stop, there are problems with the quality and quantity of food. Feeling physical and psychological discomfort, the person continues to eat. This is not a lack of will, as some people think, but an eating disorder that needs to be treated.
Feeling physical and psychological discomfort, the person continues to eat. This is not a lack of will, as some people think, but an eating disorder that needs to be treated.
Why is this happening?
Compulsive overeating develops during adolescence, when the first experiments with diets begin, often leading to anorexia nervosa or bulimia. Later, this restrictive behavior leads to the opposite - to overeating and weight gain, because, unlike bulimia nervosa, patients do not resort to cleansing practices (do not induce vomiting, do not take laxatives, do not exhaust themselves with training).
The disorder may develop in adolescents whose parents frequently use diets or have a history of eating problems that transmit ideas about the value of being light. Or if children grow up in an atmosphere of emotional and psychological abuse. Thus, they seize stress. This is a compensatory mechanism for coping with feelings of loneliness, anxiety, restlessness.
Compulsive overeating often occurs as a response to depression.
At an older age, uncontrolled eating also serves as a mechanism for coping with emotional experiences, not necessarily traumatic. It can be monotony, boredom, lack of pleasure. The less a person "feeds" himself with other emotions, the more close "friend" he becomes a refrigerator, in which you can find a variety of tastes that are missing in life. Or they are looking for a “home psychotherapist” in the refrigerator. For example, the husband drinks, and the wife "snacks": in constant anxiety, waiting for him in the evenings, she compulsively eats, for example, packs of cookies.
Another reason is the difficulty with expressing feelings, when a person does not recognize or denies his emotional experiences, does not know how to cope with them, does not have support, cannot speak out.
Compulsive overeating can also occur against the background of eating habits. For example, one or two meals a day, then hunger provokes compensatory overeating. It is also difficult to control food intake can provoke sausages, sausages, sausages - any processed food saturated with monosodium glutamate. Foods rich in easily digestible carbohydrates also stimulate appetite and hunger, as this is associated with fluctuations in blood glucose and insulin levels.
It is also difficult to control food intake can provoke sausages, sausages, sausages - any processed food saturated with monosodium glutamate. Foods rich in easily digestible carbohydrates also stimulate appetite and hunger, as this is associated with fluctuations in blood glucose and insulin levels.
Any diet aggravates the symptoms of compulsive overeating, the person is in the "hunger (diet) - breakdown" system. This is the case when they say: "minus 3 - plus 7".
Why is compulsive overeating dangerous?
In this disease, a person usually abuses fatty, sweet foods, in connection with which excess weight appears and the metabolic syndrome quickly develops - an increase in the mass of visceral fat, metabolic disorders.
Compulsive overeating has been proven to lead to type 2 diabetes, hypercholesterolemia (an abnormal increase in cholesterol levels), and arterial hypertension.
Treating compulsive overeating
How does psychotherapy help?
Psychotherapy is the only way and method of treatment for compulsive overeating. The work is going in two directions. The first is diet therapy, the development of a nutrition plan. If a person starts the morning with marshmallows and ends with boiled sausage, the chances of recovery are low. Dietary literacy needs to be taught.
The work is going in two directions. The first is diet therapy, the development of a nutrition plan. If a person starts the morning with marshmallows and ends with boiled sausage, the chances of recovery are low. Dietary literacy needs to be taught.
The second direction is directly psychotherapy. The gold standard in the treatment of the disease is cognitive behavioral therapy. Usually these are group classes, the course lasts from 12 weeks to a year. One of the tasks is to learn to isolate irrational thoughts about food, yourself, problem situations and interact with them. There are many irrational thoughts: “food helps me relax”, “fruits are not food”, “sugar is needed for the brain”, “I am genetically fat, so everything is useless”, “you can’t eat after 18.00”, etc.
These settings have nothing rational. For example, let's take the postulate about the harmfulness of eating after 18.00. Daily calorie intake is important, not the time of intake.
Be sure to work with emotions: a psychotherapist teaches people to be aware of them and express them, teaches the skills of relaxation and reducing emotional discomfort.
It is often necessary to involve the whole family in therapy, especially when it comes to adolescents who lack support and understanding in the family. For example, a girl is overweight, she is trying to normalize her diet, and family members eat pies and at the same time call her to willpower, devalue her efforts. This often undermines the already not very strong self-confidence, increases problems with eating behavior. Parents need to remember that in adolescence, compulsive overeating is associated with depression and an increased risk of suicide.
Why such a long course?
In some countries, protocols call for follow-up of patients with eating disorders, including compulsive overeating, for 6–10 years. The fact is that the disease has a high recurrence rate.
Very often people simply lack the skills to cope with the situation. I had a client who underwent treatment for compulsive overeating, but after a while she returned. It turned out that she began to overeat at work. The management informed her that her position would be reduced (she is 50 years old, she worked at this enterprise for a long time), and then they organized a new rate and asked her to train an employee. Not having the strength to refuse, feeling offended, the patient went to the eating room, where she ate and could not stop. Eating, as it were, legalized her absence from the workplace and allowed her to be distracted. Having learned about the reduction, she did not fight for herself, but tried to “swallow” the insult.
It turned out that she began to overeat at work. The management informed her that her position would be reduced (she is 50 years old, she worked at this enterprise for a long time), and then they organized a new rate and asked her to train an employee. Not having the strength to refuse, feeling offended, the patient went to the eating room, where she ate and could not stop. Eating, as it were, legalized her absence from the workplace and allowed her to be distracted. Having learned about the reduction, she did not fight for herself, but tried to “swallow” the insult.
What methods are used?
Keeping a food diary and a diary of emotions, meditation, self-hypnosis with positive attitudes ("I love myself", "I mean more").
Most psychological problems arise from the desire to become better, to be loved. So the first condition is to normalize the perception of oneself. There are special exercises for this (a person answers questions, for which he respects himself, appreciates what he likes in himself). Even with an eating disorder, it is important to accept your body. Therefore, it is recommended to look at yourself in the mirror daily in the nude or underwear. The goal is to form the right attitude towards the body: “my body looks like I take care of my health.” It's like a child or a pet. We cannot demand agility and smooth coat from a dog if we do not walk it and feed it poorly.
Even with an eating disorder, it is important to accept your body. Therefore, it is recommended to look at yourself in the mirror daily in the nude or underwear. The goal is to form the right attitude towards the body: “my body looks like I take care of my health.” It's like a child or a pet. We cannot demand agility and smooth coat from a dog if we do not walk it and feed it poorly.
Do I need medication?
Sometimes psychotherapy alone will not help. According to indications, antidepressants can be prescribed, which reduce anxiety, depression, compulsiveness (obsessive seizures).
What should relatives do?
Do not judge, do not depreciate, do not speak rude. People generally do not associate eating behavior with a mental state. And there is a connection. Therefore, advise a relative to contact a psychologist or psychotherapist.
Test: Do you have signs of an eating disorder .