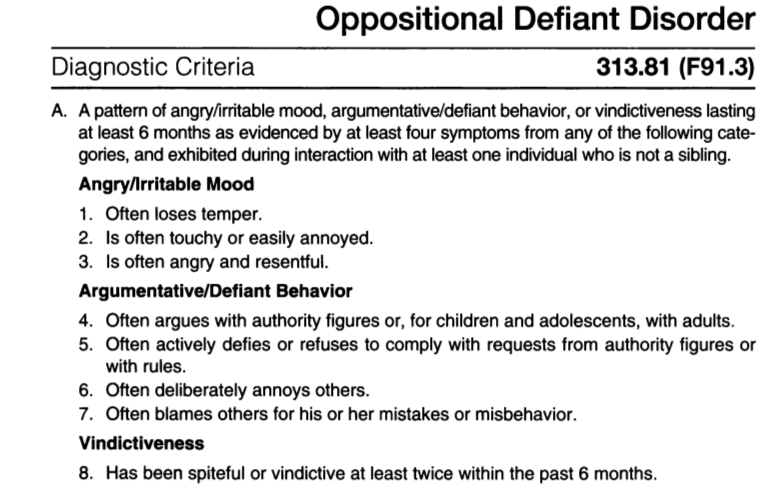
Generalized anxiety disorder diagnosis criteria
Generalized Anxiety Disorder (GAD) | Johns Hopkins Medicine
Generalized Anxiety Disorder (GAD) | Johns Hopkins MedicineWhat is generalized anxiety disorder?
If you tend to worry a lot, even when there's no reason, you may have generalized anxiety disorder (GAD). GAD means that you are worrying constantly and can't control the worrying. Healthcare providers diagnose GAD when your worrying happens on most days and for at least 6 months.
Worrying may be something you are so used to, you may think it's just "how you are." Common worries include your health, money, family, or work. While everyone worries about these things once in awhile, if you always expect the worst, it can get in the way of living a normal life.
If you have GAD, you may also have another mental health condition such as depression.
What causes GAD?
GAD can develop when you can't cope well with your internal stress. It also runs in families, but it's not understood why some people get it and others don't. Researchers have shown that the areas of the brain that control fear and anxiety are involved.
The symptoms of GAD can happen as a side effect of a medicine or substance abuse. It can also be related to medical conditions, such as hyperthyroidism, that increase hormones. This can make the body response more excitable. GAD can be triggered by family or environmental stress. Chronic illness and disease can also trigger GAD.
What are the symptoms of GAD?
If you have GAD, you likely know that your anxiety is more intense than the situation calls for, but still you can't stop these unfounded concerns. While each person may experience symptoms differently, the following are the most common symptoms:
- Trouble falling or staying asleep
- Trembling
- Twitching
- Tense muscles
- Headaches
- Irritability
- Sweating
- Hot flashes
- Lightheadedness
- Trouble breathing
- Nausea
- Urinating often
- Lump in the throat
- Fatigue
- Poor concentration
- Being easily startled
- Unable to relax
The symptoms of GAD may look like other mental health conditions. Always see your healthcare provider for a diagnosis.
Always see your healthcare provider for a diagnosis.
GAD begins gradually, usually in childhood or adolescence, but can begin in adulthood, too. It is more common in women. It often runs in families.
How is GAD diagnosed?
Your healthcare provider or mental health professional diagnoses GAD. They can help determine whether your symptoms are related to another problem. The symptoms happen on most days and last 6 months or longer.
How is GAD treated?
Your healthcare provider will consider your overall health, and other factors when advising treatment for you.
Treatment may include:
- Medicine
- Counseling (cognitive behavioral therapy, or psychotherapy)
- Relaxation techniques
- Working with a therapist to boost coping skills
- Making lifestyle changes to reduce stress and avoid stimulating substances. Also, seek help with quitting smoking, drug or alcohol use.
When should I call my healthcare provider?
If you have any symptoms of GAD, see your healthcare provider.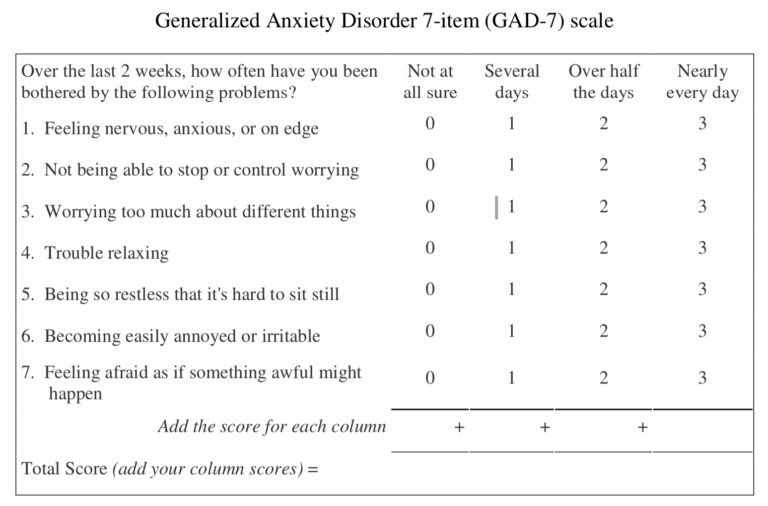
Key points about GAD?
- Generalized anxiety disorder is a condition of excessive worry about everyday issues and situations.
- It lasts longer than 6 months.
- In addition to feeling worried you may also feel restlessness, fatigue, trouble concentrating, irritability, increased muscle tension, and trouble sleeping.
- The best treatment involves a combination of both medicines and cognitive behavioral therapy. Symptoms tend to be chronic but get less severe as person gets older.
Next steps
Tips to help you get the most from a visit to your healthcare provider:
- Know the reason for your visit and what you want to happen.
- Before your visit, write down questions you want answered.
- Bring someone with you to help you ask questions and remember what your provider tells you.
- At the visit, write down the name of a new diagnosis, and any new medicines, treatments, or tests. Also write down any new instructions your provider gives you.
- Know why a new medicine or treatment is prescribed, and how it will help you. Also know what the side effects are.
- Ask if your condition can be treated in other ways.
- Know why a test or procedure is recommended and what the results could mean.
- Know what to expect if you do not take the medicine or have the test or procedure.
- If you have a follow-up appointment, write down the date, time, and purpose for that visit.
- Know how you can contact your provider if you have questions.
Related
-
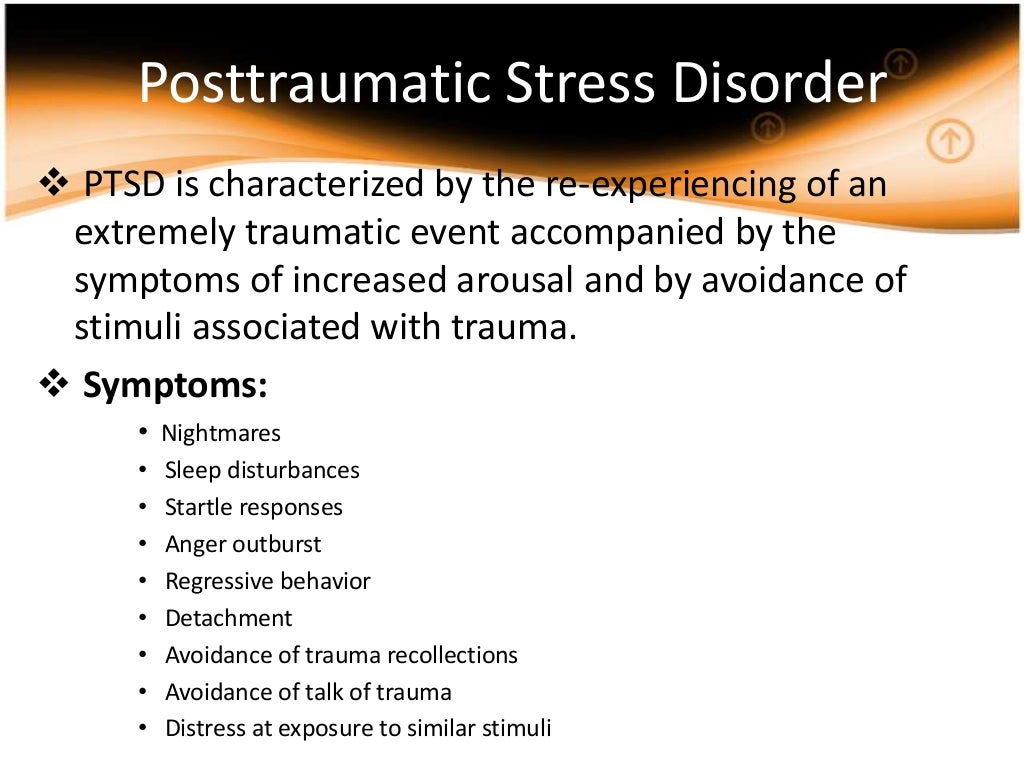
Post-Traumatic Stress Disorder (PTSD)
Posttraumatic Stress Disorder (PTSD)
-
Phobias
Phobias
-
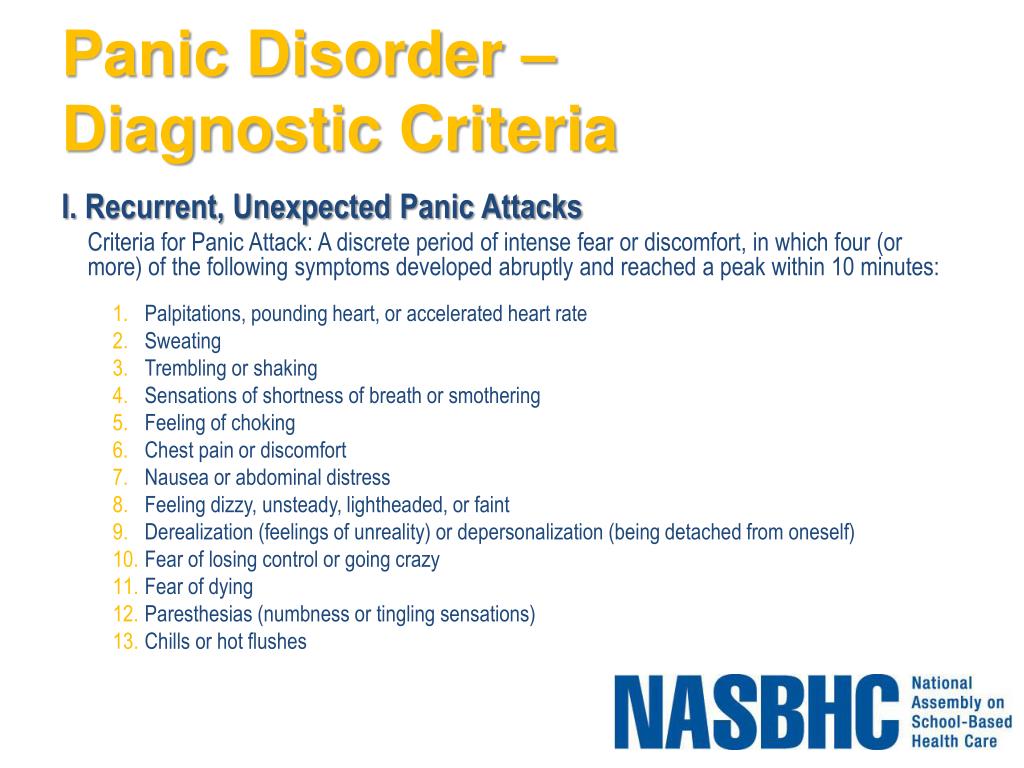
Panic Disorder
Panic Disorder
Related Topics
A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7 | Anxiety Disorders | JAMA Internal Medicine
Abstract
Background
Generalized anxiety disorder (GAD) is one of the most common mental disorders; however, there is no brief clinical measure for assessing GAD. The objective of this study was to develop a brief self-report scale to identify probable cases of GAD and evaluate its reliability and validity.
The objective of this study was to develop a brief self-report scale to identify probable cases of GAD and evaluate its reliability and validity.
Methods A criterion-standard study was performed in 15 primary care clinics in the United States from November 2004 through June 2005. Of a total of 2740 adult patients completing a study questionnaire, 965 patients had a telephone interview with a mental health professional within 1 week. For criterion and construct validity, GAD self-report scale diagnoses were compared with independent diagnoses made by mental health professionals; functional status measures; disability days; and health care use.
Results
A 7-item anxiety scale (GAD-7) had good reliability, as well as criterion, construct, factorial, and procedural validity. A cut point was identified that optimized sensitivity (89%) and specificity (82%). Increasing scores on the scale were strongly associated with multiple domains of functional impairment (all 6 Medical Outcomes Study Short-Form General Health Survey scales and disability days). Although GAD and depression symptoms frequently co-occurred, factor analysis confirmed them as distinct dimensions. Moreover, GAD and depression symptoms had differing but independent effects on functional impairment and disability. There was good agreement between self-report and interviewer-administered versions of the scale.
Although GAD and depression symptoms frequently co-occurred, factor analysis confirmed them as distinct dimensions. Moreover, GAD and depression symptoms had differing but independent effects on functional impairment and disability. There was good agreement between self-report and interviewer-administered versions of the scale.
Conclusion The GAD-7 is a valid and efficient tool for screening for GAD and assessing its severity in clinical practice and research.
One of the most common anxiety disorders seen in general medical practice and in the general population is generalized anxiety disorder (GAD). The disorder has an estimated current prevalence in general medical practice of 2.8% to 8.5%1-3 and in the general population of 1.6% to 5.0%.4-6 Whereas depression in clinical settings has generated substantial research, there have been far fewer studies of anxiety. In part, this may be because of the paucity of brief validated measures for anxiety compared with the numerous measures for depression,7,8 such as the Primary Care Evaluation of Mental Disorders 9-item Patient Health Questionnaire (PHQ). 9-11 This situation is unfortunate, given the high prevalence of anxiety disorders, as well as their associated disability and the availability of effective treatments, both pharmacological and nonpharmacological.12,13
9-11 This situation is unfortunate, given the high prevalence of anxiety disorders, as well as their associated disability and the availability of effective treatments, both pharmacological and nonpharmacological.12,13
Measures of anxiety are seldom used in clinical practice because of their length, proprietary nature, lack of usefulness as a diagnostic and severity measure,14-17 and requirement of clinician administration rather than patient self-report.18,19 The goal of this study was to develop a brief scale to identify probable cases of GAD and to assess symptom severity. We conducted a study in multiple primary care sites to select the items for the final scale and to evaluate its reliability and validity.
Methods
Gad scale development
We first selected potential items for a brief GAD scale. The initial item pool consisted of 9 items that reflected all of the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) symptom criteria for GAD and 4 items on the basis of review of existing anxiety scales. A 13-item questionnaire was developed that asked patients how often, during the last 2 weeks, they were bothered by each symptom. Response options were “not at all,” “several days,” “more than half the days,” and “nearly every day,” scored as 0, 1, 2, and 3, respectively. In addition, an item to assess duration of anxiety symptoms was included. Our goal was to determine the number of items necessary to achieve good reliability and procedural, construct, and diagnostic criterion validity.
The initial item pool consisted of 9 items that reflected all of the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) symptom criteria for GAD and 4 items on the basis of review of existing anxiety scales. A 13-item questionnaire was developed that asked patients how often, during the last 2 weeks, they were bothered by each symptom. Response options were “not at all,” “several days,” “more than half the days,” and “nearly every day,” scored as 0, 1, 2, and 3, respectively. In addition, an item to assess duration of anxiety symptoms was included. Our goal was to determine the number of items necessary to achieve good reliability and procedural, construct, and diagnostic criterion validity.
Patient sample
Patients were enrolled from November 2004 through June 2005 from a research network of 15 primary care sites located in 12 states (13 family practice, 2 internal medicine) administered centrally by Clinvest, Inc (Springfield, Mo). The purpose of the project's first phase (n = 2149) was to select the scale items and cutoff scores to be used for making a GAD diagnosis. The purpose of the second phase (n = 591) was to determine the scale's test-retest reliability. In all, 2982 subjects were approached and 2739 (91.9%) completed the study questionnaire with no or minimal missing data. To minimize sampling bias, we approached consecutive patients at each site in clinic sessions until the target quota for that week was achieved.
The purpose of the project's first phase (n = 2149) was to select the scale items and cutoff scores to be used for making a GAD diagnosis. The purpose of the second phase (n = 591) was to determine the scale's test-retest reliability. In all, 2982 subjects were approached and 2739 (91.9%) completed the study questionnaire with no or minimal missing data. To minimize sampling bias, we approached consecutive patients at each site in clinic sessions until the target quota for that week was achieved.
In the first phase, 1654 subjects also agreed to a telephone interview, and of these, a random sample of 965 were interviewed within 1 week of their clinic visit by 1 of 2 mental health professionals (MHPs)—a PhD clinical psychologist and a senior psychiatric social worker. In the study's second phase, 591 subjects who had completed the research questionnaire were sent a 1-page questionnaire that consisted of the 13 potential GAD scale items. Of these, 236 subjects returned the completed 1-page questionnaire with no or minimal missing data within a week of completing the research questionnaire at the clinic. The mean GAD scale score of subjects returning the questionnaire did not differ from that of subjects who did not return the questionnaire. The study was approved by the Sterling Institutional Review Board, Springfield, Mo.
The mean GAD scale score of subjects returning the questionnaire did not differ from that of subjects who did not return the questionnaire. The study was approved by the Sterling Institutional Review Board, Springfield, Mo.
Self-report research questionnaire
Before seeing their physicians, patients completed a 4-page questionnaire that included the 13 items being tested for use in the GAD scale, as well as questions about age, sex, education, ethnicity, and marital status; the Medical Outcomes Study Short-Form General Health Survey (SF-20),20,21 which measures functional status in 6 dimensions; and either the 12-item anxiety subscale from the Symptom Checklist-9016 (first study phase only) or the Beck Anxiety Inventory14 (second study phase only). Depression was assessed with the PHQ-8, which includes all items from the PHQ-9 except for the item about suicidal ideation; PHQ-8 and PHQ-9 scores are highly correlated and have nearly identical operating characteristics. 22 Finally, patients completed items regarding physician visits and disability days during the previous 3 months.
22 Finally, patients completed items regarding physician visits and disability days during the previous 3 months.
Mhp interview
The 2 MHPs conducted structured psychiatric interviews by telephone, blinded to the results of the self-report research questionnaire. The interview consisted of the GAD section of the Structured Clinical Interview for DSM-IV,23 modified with several additional questions to assess in greater detail some of the GAD diagnostic criteria of DSM-IV. The resulting DSM-IV GAD diagnosis, with the DSM-IV 6-month duration criterion, was used as the criterion standard for assessing the validity of the new scale. The interview also included the 13 potential GAD scale items to test agreement between self-report and clinician administration (ie, procedural validity).24
Data analysis
The best items for the GAD scale were selected by rank ordering the correlation of each item with the total 13-item scale score in the sample of 1184 patients who did not undergo the MHP interview. Item-total score correlations were reexamined in 2 independent subsamples of the study population: the 965 patients who underwent the MHP interview and the 591 patients in the second phase of the study. In addition, we conducted receiver operating characteristic analyses with varying numbers of items in these 965 patients by using an MHP diagnosis of GAD as the criterion standard. Divergent validity of each item was assessed by calculating the difference between the item correlations with the 13-item anxiety score and the PHQ-8 depression score. Convergent validity was assessed by examining correlations of the final version of the GAD scale with the Beck Anxiety Inventory and the anxiety subscale of the Symptom Checklist-90, even though neither scale is specific for GAD.
Item-total score correlations were reexamined in 2 independent subsamples of the study population: the 965 patients who underwent the MHP interview and the 591 patients in the second phase of the study. In addition, we conducted receiver operating characteristic analyses with varying numbers of items in these 965 patients by using an MHP diagnosis of GAD as the criterion standard. Divergent validity of each item was assessed by calculating the difference between the item correlations with the 13-item anxiety score and the PHQ-8 depression score. Convergent validity was assessed by examining correlations of the final version of the GAD scale with the Beck Anxiety Inventory and the anxiety subscale of the Symptom Checklist-90, even though neither scale is specific for GAD.
To assess construct validity, we used analysis of covariance to examine associations between anxiety severity on the final GAD scale and SF-20 functional status scales, self-reported disability days, and physician visits, controlling for demographic variables. For criterion validity, we investigated sensitivity, specificity, predictive values, and likelihood ratios for a range of cutoff scores of the final scale with respect to the MHP diagnosis. To investigate whether anxiety as measured by the GAD-7 and depression as measured by the PHQ-8 reflect distinct dimensions, we assessed factorial validity by using confirmatory factor analyses. Finally, procedural validity and test-retest reliability were assessed by means of intraclass correlation.25
For criterion validity, we investigated sensitivity, specificity, predictive values, and likelihood ratios for a range of cutoff scores of the final scale with respect to the MHP diagnosis. To investigate whether anxiety as measured by the GAD-7 and depression as measured by the PHQ-8 reflect distinct dimensions, we assessed factorial validity by using confirmatory factor analyses. Finally, procedural validity and test-retest reliability were assessed by means of intraclass correlation.25
Results
Description of patients
The mean (SD) age of the patients was 47.4 (15.5) years (range, 18-95 years). Most (65%) were female; 80% were white non-Hispanic, 8% were African American, and 9% were Hispanic; 64% were married, 13% were divorced, and 15% were never married; and 31% had a high school degree or equivalent, whereas 62% had attended some college.
Item selection for the gad scales
The GAD-7 (Figure 1) consists of the 7 items with the highest correlation with the total 13-item scale score (r = 0. 75-0.85). Receiver operating characteristic analysis with this set of items showed an area under the curve (0.906) as good as scales with as much as the full 13-item set. These 7 items also had the highest rank correlations in the developmental sample (n = 1184) and the 2 replication samples (n = 965 and n = 591). The 2 core criteria (A and B) of the DSM-IV definition of GAD are captured by the first 3 items of the scale.26 Of note, 6 of the 7 items had the greatest divergent validity (ie, the highest difference between the item-total scale score correlation and item-PHQ-8 depression score correlation [Δ r = 0.16-0.21]). Because each of the 7 items is scored from 0 to 3, the GAD-7 scale score ranges from 0 to 21.
75-0.85). Receiver operating characteristic analysis with this set of items showed an area under the curve (0.906) as good as scales with as much as the full 13-item set. These 7 items also had the highest rank correlations in the developmental sample (n = 1184) and the 2 replication samples (n = 965 and n = 591). The 2 core criteria (A and B) of the DSM-IV definition of GAD are captured by the first 3 items of the scale.26 Of note, 6 of the 7 items had the greatest divergent validity (ie, the highest difference between the item-total scale score correlation and item-PHQ-8 depression score correlation [Δ r = 0.16-0.21]). Because each of the 7 items is scored from 0 to 3, the GAD-7 scale score ranges from 0 to 21.
Reliability and procedural validity
The internal consistency of the GAD-7 was excellent (Cronbach α = .92). Test-retest reliability was also good (intraclass correlation = 0.83). Comparison of scores derived from the self-report scales with those derived from the MHP-administered versions of the same scales yielded similar results (intraclass correlation = 0. 83), indicating good procedural validity.
83), indicating good procedural validity.
Diagnostic criterion validity and scale operating characteristics
Table 1 summarizes the operating characteristics of the GAD-7 at various cut points. As expected, as the cut point increases, sensitivity decreases and specificity increases in a continuous fashion. At a cut point of 10 or greater, sensitivity and specificity exceed 0.80, and sensitivity is nearly maximized. Results were similar for men and women and for those aged less and those aged more than the mean age of 47 years. The proportion of primary care patients who score at this level is high (23%). A cut point of 15 or greater maximizes specificity and approximates a prevalence (9%) more in line with current epidemiologic estimates of GAD prevalence in primary care. However, sensitivity at this high cut point is low (48%). Most patients (89%) with GAD had GAD-7 scores of 10 or greater, whereas most patients (82%) without GAD had scores less than 10.
The mean (SD) GAD-7 score was 14.4 (4.7) in the 73 patients with GAD diagnosed according to the MHP and 4.9 (4.8) in the 892 patients without GAD. The prevalence of GAD according to the MHP interview was 9% in women and 4% in men. In the entire sample of 2739 patients, the mean GAD-7 score was 6.1 in women and 4.6 in men.
Although the GAD-7 scale inquires about symptoms in the past 2 weeks, the criterion-standard MHP interview required at least a 6-month duration of symptoms consistent with DSM-IV diagnostic criteria for GAD. Nonetheless, the operating characteristics of the scale were good because most patients with high symptom scores had chronic symptoms. Of the 433 patients with GAD-7 scores of 10 or greater, 96% had symptoms for 1 month or more, and 67% had symptoms for 6 months or more.
Construct validity
There was a strong association between increasing GAD-7 severity scores and worsening function on all 6 SF-20 scales (Table 2). As GAD-7 scores went from mild to moderate to severe, there was a substantial stepwise decline in functioning in all 6 SF-20 domains. Most pairwise comparisons within each SF-20 scale between successive GAD-7 severity levels were significant. The relationship between GAD severity and functional impairment was similar in men and women.
As GAD-7 scores went from mild to moderate to severe, there was a substantial stepwise decline in functioning in all 6 SF-20 domains. Most pairwise comparisons within each SF-20 scale between successive GAD-7 severity levels were significant. The relationship between GAD severity and functional impairment was similar in men and women.
Figure 2 illustrates graphically the relationship between increasing GAD-7 scale scores and worsening functional status. Decrements in SF-20 scores are shown in terms of effect size (ie, the difference in mean SF-20 scores, expressed as the number of SDs, between each GAD-7 interval subgroup and the reference group). The reference group is the group with the lowest GAD-7 scores (ie, 0-4), and the SD used is that of the entire sample. Effect sizes of 0.5 and 0.8 are typically considered moderate and large between-group differences, respectively.27
When the GAD-7 was examined as a continuous variable, its strength of association with the SF-20 scales was concordant with the pattern seen in Figure 2.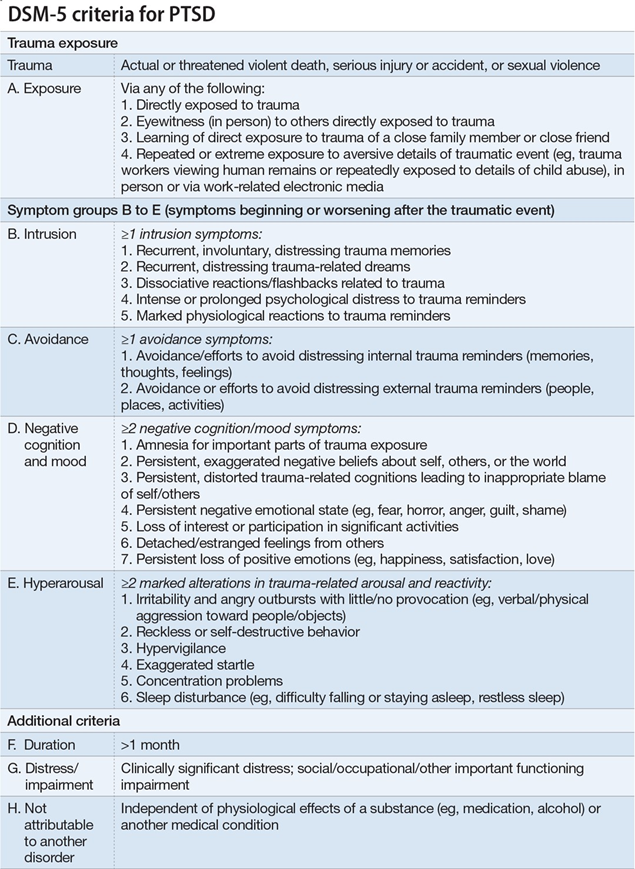 The GAD-7 correlated most strongly with mental health (0.75), followed by social functioning (0.46), general health perceptions (0.44), bodily pain (0.36), role functioning (0.33), and physical functioning (0.30).
The GAD-7 correlated most strongly with mental health (0.75), followed by social functioning (0.46), general health perceptions (0.44), bodily pain (0.36), role functioning (0.33), and physical functioning (0.30).
Table 3 shows the association between GAD-7 severity levels and 3 other measures of construct validity: self-reported disability days, clinic visits, and the general amount of difficulty patients attribute to their symptoms. Greater levels of anxiety severity were associated with a monotonic increase in disability days, health care use, and symptom-related difficulty in activities and relationships. When the GAD-7 was examined as a continuous variable, its correlation was 0.27 with disability days, 0.22 with physician visits, and 0.63 with symptom-related difficulty.
Convergent validity of the GAD-7 was good, as demonstrated by its correlations with 2 anxiety scales: the Beck Anxiety Inventory (r = 0.72) and the anxiety subscale of the Symptom Checklist-90 (r = 0. 74). Consistent with results of previous studies of anxiety and depression,4,28 the GAD-7 and Symptom Checklist-90 anxiety scales also strongly correlated with our depression measure, the PHQ-8 (r = 0.75 and r = 0.74, respectively). Nonetheless, measuring anxiety and depression was complementary rather than duplicative. We determined the prevalence of high anxiety and high depression symptom severity in our sample, defined as severe scores (≥15) on the GAD-7 and PHQ-8 depression scales, respectively. In the 2114 patients who completed the GAD-7 and the PHQ-8, there were 1877 (88.8%) patients with neither high anxiety nor high depression, 99 (4.68%) with high anxiety only, 68 (3.2%) with high depression only, and 70 (3.31%) with high anxiety and high depression. Thus, more than half (99/169) of patients with high anxiety scores did not have high depression scores. Also, when patients had high anxiety and high depression scores, there was an additive effect on the SF-20 mental health and social functioning scales, as well as self-reported disability days and health care use.
74). Consistent with results of previous studies of anxiety and depression,4,28 the GAD-7 and Symptom Checklist-90 anxiety scales also strongly correlated with our depression measure, the PHQ-8 (r = 0.75 and r = 0.74, respectively). Nonetheless, measuring anxiety and depression was complementary rather than duplicative. We determined the prevalence of high anxiety and high depression symptom severity in our sample, defined as severe scores (≥15) on the GAD-7 and PHQ-8 depression scales, respectively. In the 2114 patients who completed the GAD-7 and the PHQ-8, there were 1877 (88.8%) patients with neither high anxiety nor high depression, 99 (4.68%) with high anxiety only, 68 (3.2%) with high depression only, and 70 (3.31%) with high anxiety and high depression. Thus, more than half (99/169) of patients with high anxiety scores did not have high depression scores. Also, when patients had high anxiety and high depression scores, there was an additive effect on the SF-20 mental health and social functioning scales, as well as self-reported disability days and health care use.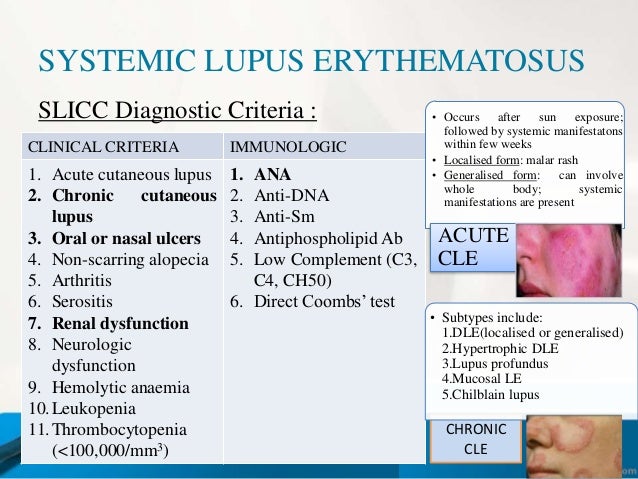
Factorial validity
Principal component analysis of a set of 15 items that includes the 8 depression items of the PHQ-8 and the 7 anxiety items of the GAD-7 indicated that the first 2 emergent factors had an eigenvalue greater than 1. Sixty-three percent of the total variance was explained by the first 2 factors. The varimax-rotated component-matrix clearly confirmed the original allocation of the items to the PHQ scales, with all depression items having the highest factor loadings on 1 factor (0.58-0.75) and all anxiety items having the highest factor loadings on the second factor (0.69-0.81).
Comment
This study has several major findings. First, a 7-item anxiety scale—the GAD-7—is a useful tool with strong criterion validity for identifying probable cases of GAD. Second, the scale is also an excellent severity measure as demonstrated by the fact that increasing scores on the GAD-7 are strongly associated with multiple domains of functional impairment and disability days. Third, although many patients had anxiety and depressive symptoms, factor analysis confirms GAD and depression as distinct dimensions.
Third, although many patients had anxiety and depressive symptoms, factor analysis confirms GAD and depression as distinct dimensions.
This study reports the development and validation of a measure for evaluating the presence and severity of GAD in clinical practice, the GAD-7, one of the few GAD measures that is also specifically linked to the DSM-IV (Text Revision) criteria.19,26 A score of 10 or greater on the GAD-7 represents a reasonable cut point for identifying cases of GAD. Cut points of 5, 10, and 15 might be interpreted as representing mild, moderate, and severe levels of anxiety on the GAD-7, similar to levels of depression on the PHQ-9.10 The GAD-7 may be particularly useful in assessing symptom severity and monitoring change across time, although its responsiveness to change remains to be tested in treatment studies.
Construct validity was demonstrated by the fact that increasing scores on the GAD-7 scale were strongly associated with multiple domains of functional impairment. Furthermore, there was a strong association with self-reported disability days and a modest association with increased health care use.
Furthermore, there was a strong association with self-reported disability days and a modest association with increased health care use.
To facilitate assessment of change in severity of anxiety symptoms, the GAD-7 asks about recent symptoms (ie, in the past 2 weeks). However, most patients with high scores had chronic symptoms, which is why the operating characteristics proved good with use of our criterion-standard MHP interviews based on the conventional GAD duration criterion of 6 months. However, the National Comorbidity Survey showed that patients with episodes of 1 to 5 months do not differ greatly from those with episodes of 6 months or more in onset, persistence, impairment, comorbidity, parental GAD, or sociodemographic correlates.5 Kessler et al5 conclude that there is little basis for excluding these people from a diagnosis. Notably, 96% of patients with GAD-7scores of 10 or greater in our primary care sample had symptoms of a month or more, whereas 67% had symptoms of 6 months or longer.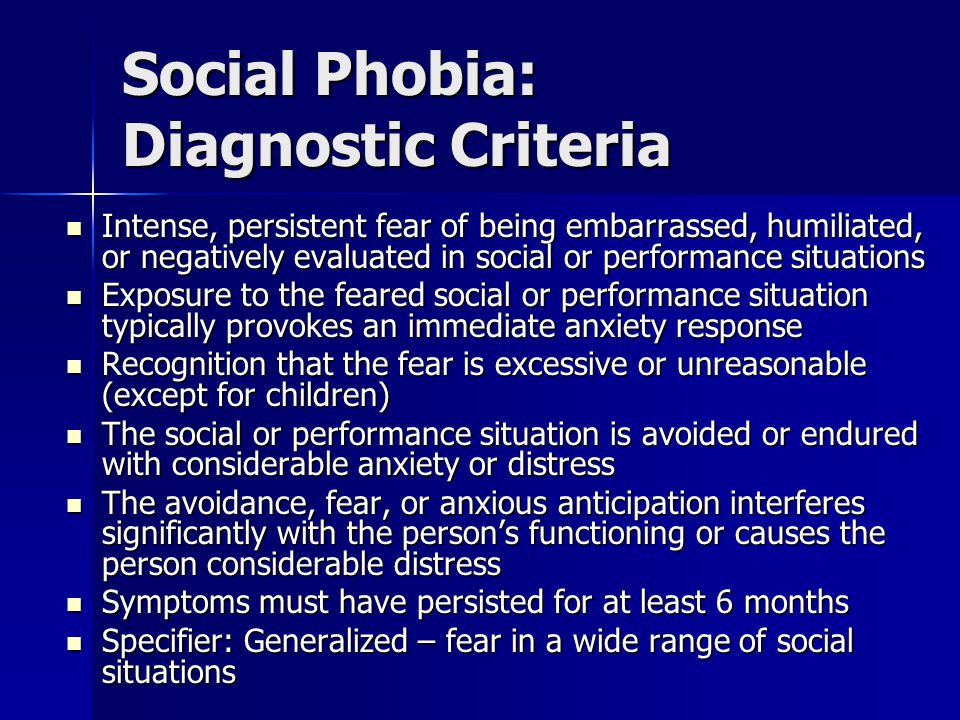 It may be that in treatment trials in which response to therapy is evaluated, assessing GAD symptom change during a shorter time (eg, the past week) may be desirable.
It may be that in treatment trials in which response to therapy is evaluated, assessing GAD symptom change during a shorter time (eg, the past week) may be desirable.
The high comorbidity of anxiety and depressive disorders and the high correlation between depressive and anxiety measures is well known.17,29 Not surprisingly, our depression measure, the PHQ-8, strongly correlated with the GAD-7 and the Symptom Checklist-90 anxiety scales. Nonetheless, factor analysis confirmed the value of assessing anxiety and depression as 2 separate dimensions. In addition, a number of patients with high anxiety symptoms according to the GAD-7 did not have high depression symptom severity, and patients with increasing severity of anxiety symptoms had corresponding greater impairment in multiple domains of functional status. Together, these findings indicate that using only a depression measure to identify depressed patients who may benefit from treatment will miss a clinically important part of the patient population with disabling anxiety who also would benefit from treatment.
Several limitations of our study should be noted. First, the GAD-7 scale focuses on only 1 anxiety disorder, although there are many patients with other anxiety disorders, such as social phobia and posttraumatic stress disorder, who need clinical attention. However, GAD is one of the most common mental disorders seen in outpatient practice. Second, the GAD-7 provides only probable diagnoses that should be confirmed by further evaluation. Third, because our study was cross-sectional, prospective observational and treatment studies are needed to determine the responsiveness of the GAD-7 in assessing change across time. Because there is already evidence for the responsiveness of the PHQ-9 and PHQ-2 depression scales,30,31 future research also likely will demonstrate that the GAD-7 scale is useful in assessing changes in the severity of anxiety over time.
This study has a number of strengths, including its large sample size, diverse clinical settings, and its generalizability to primary care, where most patients with anxiety and depression are treated. 2 Also, the GAD-7 is efficient in that it is brief and can be completed entirely by the patient. This latter feature is particularly important, given the time constraints and competing demands for busy clinicians.32 Although the GAD-7 was developed and validated in primary care, we expect that, like the PHQ-9 depression measure, the GAD-7 will have considerable utility in busy mental health settings and clinical research, which is especially important given the high prevalence and substantial disability associated with GAD.
2 Also, the GAD-7 is efficient in that it is brief and can be completed entirely by the patient. This latter feature is particularly important, given the time constraints and competing demands for busy clinicians.32 Although the GAD-7 was developed and validated in primary care, we expect that, like the PHQ-9 depression measure, the GAD-7 will have considerable utility in busy mental health settings and clinical research, which is especially important given the high prevalence and substantial disability associated with GAD.
Back to top
Article Information
Correspondence: Robert L. Spitzer, MD, Department of Psychiatry, New York State Psychiatric Institute, Unit 60, 1051 Riverside Dr, New York, NY 10032 ([email protected]).
Accepted for Publication: January 2, 2006.
Funding/Support: The development of the GAD-7 scale was underwritten by an unrestricted educational grant from Pfizer Inc (New York, NY). Dr Spitzer had full access to the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Dr Spitzer had full access to the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Acknowledgment: Mark Davies, MS, assisted in the statistical analysis. Jeffrey G. Johnson, PhD, assisted in data collection and commented on early drafts. Diane Engel, MSW, also assisted in data collection.
References
1.
Olfson MFireman BWeissman MMLeon ACSheehan DVKathol RG Mental disorders and disability among patients in a primary care group practice. Am J Psychiatry 1997;1541734- 1740PubMedGoogle Scholar
2.
Roy-Byrne PPWagner A Primary care perspectives on generalized anxiety disorder. J Clin Psychiatry 2004;65 ((suppl 13)) 20- 26PubMedGoogle Scholar
3.
Leon ACOlfson MBroadhead WE et al. Prevalence of mental disorders in primary care: implications for screening. Arch Fam Med 1995;4857- 861PubMedGoogle ScholarCrossref
4.
Wittchen HUZhao SKessler RCEaton WW DSM-III-R generalized anxiety disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1994;51355- 364PubMedGoogle ScholarCrossref
5.
Kessler RCBrandenburg NLane M et al. Rethinking the duration requirement for generalized anxiety disorder: evidence from the National Comorbidity Survey Replication. Psychol Med 2005;351073- 1082PubMedGoogle ScholarCrossref
6.
Kessler RCKeller MBWittchen HU The epidemiology of generalized anxiety disorder. Psychiatr Clin North Am 2001;2419- 39PubMedGoogle ScholarCrossref
7.
Williams JWPignone MRamirez GPerez SC Identifying depression in primary care: a literature synthesis of case-finding instruments. Gen Hosp Psychiatry 2002;24225- 237PubMedGoogle ScholarCrossref
8.
Löwe BSpitzer RLGräfe K et al. Comparative validity of three screening questionnaires for DSM-IV depressive disorders and physicians' diagnoses. J Affect Disord 2004;78131- 140PubMedGoogle ScholarCrossref
9.
Spitzer
RLKroenke
KWilliams
JBPatient Health Questionnaire Primary Care Study Group, Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study.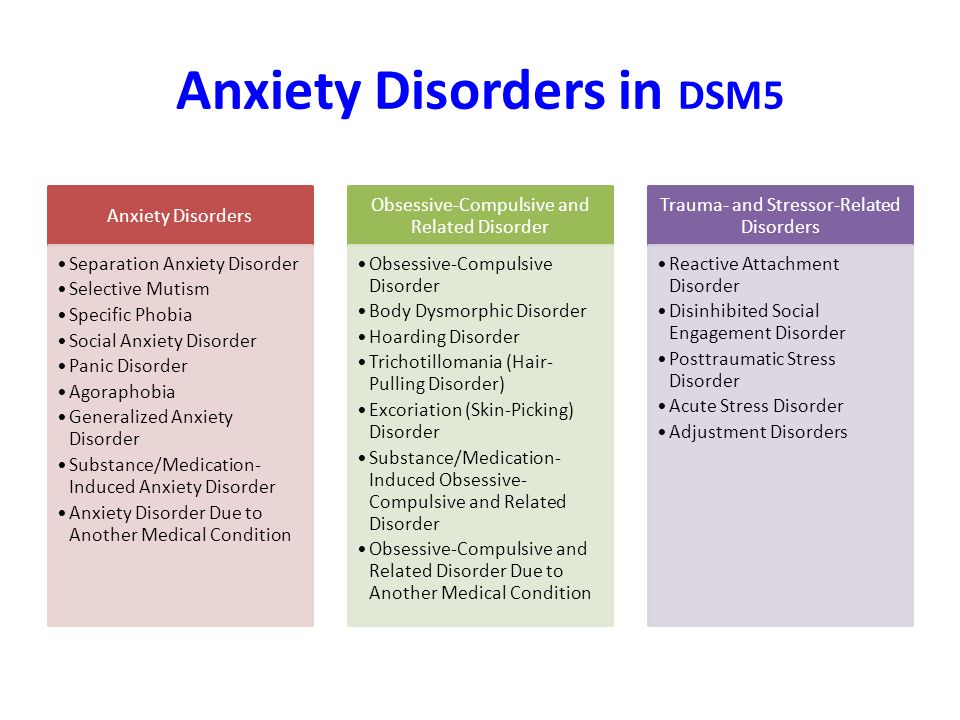 JAMA 1999;2821737- 1744PubMedGoogle ScholarCrossref
JAMA 1999;2821737- 1744PubMedGoogle ScholarCrossref
10.
Kroenke KSpitzer RLWilliams JB The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001;16606- 613PubMedGoogle ScholarCrossref
11.
Löwe BGräfe KZipfel SWitte SLoerch BHerzog W Diagnosing ICD-10 depressive episodes: superior criterion validity of the Patient Health Questionnaire. Psychother Psychosom 2004;73386- 390PubMedGoogle ScholarCrossref
12.
Fricchione G Clinical practice: generalized anxiety disorder. N Engl J Med 2004;351675- 682PubMedGoogle ScholarCrossref
13.
Westen DMorrison K A multidimensional meta-analysis of treatments for depression, panic, and generalized anxiety disorder: an empirical examination of the status of empirically supported therapies. J Consult Clin Psychol 2001;69875- 899PubMedGoogle ScholarCrossref
14.
Beck ATEpstein NBrown GSteer RA An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol 1988;56893- 897PubMedGoogle ScholarCrossref
15.
Zimmerman MMattia JI A self-report scale to help make psychiatric diagnoses: the Psychiatric Diagnostic Screening Questionnaire. Arch Gen Psychiatry 2001;58787- 794PubMedGoogle ScholarCrossref
16.
Derogatis LRLipman RSRickels KUhlenhuth EHCovi L The Hopkins Symptom Checklist (HSCL): a measure of primary symptom dimensions. Mod Probl Pharmacopsychiatry 1974;779- 110PubMedGoogle Scholar
17.
Bjelland IDahl AAHaug TTNeckelmann D The validity of the Hospital Anxiety and Depression Scale: an updated literature review. J Psychosom Res 2002;5269- 77PubMedGoogle ScholarCrossref
18.
Hamilton M The assessment of anxiety states by rating. Br J Med Psychol 1959;3250- 55Google ScholarCrossref
19.
Antony
MMedOrsillo
SMedRoemer
Led Practitioner's Guide to Empirically Based Measures of Anxiety.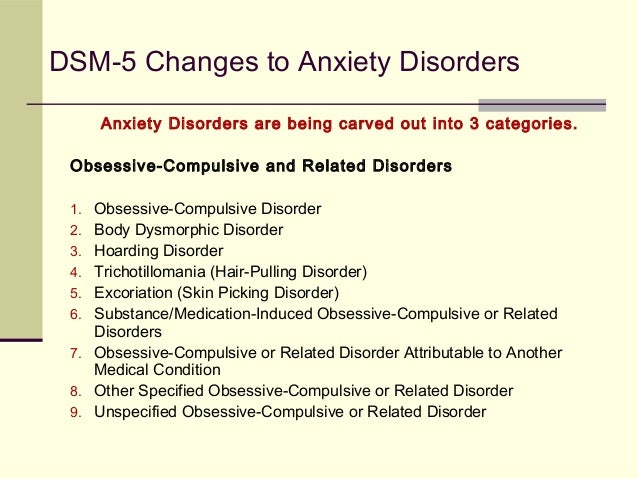 New York, NY Kluwer Academic/Plenum Publishers2001;
New York, NY Kluwer Academic/Plenum Publishers2001;
20.
Stewart ALHays RDWare JE Jr The MOS short-form general health survey: reliability and validity in a patient population. Med Care 1988;26724- 735PubMedGoogle ScholarCrossref
21.
Ware JESherbourne CD The MOS 36-item short-form health survey (SF-36), I: conceptual framework and item selection. Med Care 1992;30473- 483PubMedGoogle ScholarCrossref
22.
Kroenke KSpitzer RL The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Ann 2002;91- 7Google Scholar
23.
First
MBSpitzer
RLWilliams
JBWGibbon
M Structured Clinical Interview for DSM-IV (SCID). Washington, DC American Psychiatric Association1995;
Washington, DC American Psychiatric Association1995;
24.
Pinto-Meza ASerrano-Blanco APenarrubia MTBlanco EHaro JM Assessing depression in primary care with the PHQ-9: can it be carried out over the telephone? J Gen Intern Med 2005;20738- 742PubMedGoogle ScholarCrossref
25.
Deyo RADiehr PPatrick DL Reproducibility and responsiveness of health status measures: statistics and strategies for evaluation. Control Clin Trials 1991;12142S- 158SPubMedGoogle ScholarCrossref
26.
American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders DSM-IV-TR (Text Revision). 4th ed. Washington, DC American Psychiatric Association2000;
27.
Kazis LEAnderson JJMeenan RF Effect sizes for interpreting changes in health status. Med Care 1989;27S178- S189PubMedGoogle ScholarCrossref
28.
Carter RMWittchen HUPfister HKessler RC One-year prevalence of subthreshold and threshold DSM-IV generalized anxiety disorder in a nationally representative sample. Depress Anxiety 2001;1378- 88PubMedGoogle ScholarCrossref
29.
Clark DASteer RABeck AT Common and specific dimensions of self-reported anxiety and depression: implications for the cognitive and tripartite models. J Abnorm Psychol 1994;103645- 654PubMedGoogle ScholarCrossref
30.
Löwe
BUnützer
JCallahan
CMPerkins
AJKroenke
K Monitoring depression treatment outcomes with the Patient Health Questionnaire-9. Med Care 2004;421194- 1201PubMedGoogle ScholarCrossref
Med Care 2004;421194- 1201PubMedGoogle ScholarCrossref
31.
Löwe BKroenke KGräfe K Detecting and monitoring depression with a 2-item questionnaire (PHQ-2). J Psychosom Res 2005;58163- 171PubMedGoogle ScholarCrossref
32.
Klinkman MS Competing demands in psychosocial care: a model for the identification and treatment of depressive disorders in primary care. Gen Hosp Psychiatry 1997;1998- 111PubMedGoogle ScholarCrossref
Generalized anxiety disorder
"That is why it is necessary first and foremost to treat the soul, if you want the head and the rest of the body to feel good" Plato
DEFINITION
Chronic anxiety that is not associated with specific environmental circumstances.
Frequency of mental disorders in Europe
ECNP/EBC. 2011;21:655–79.
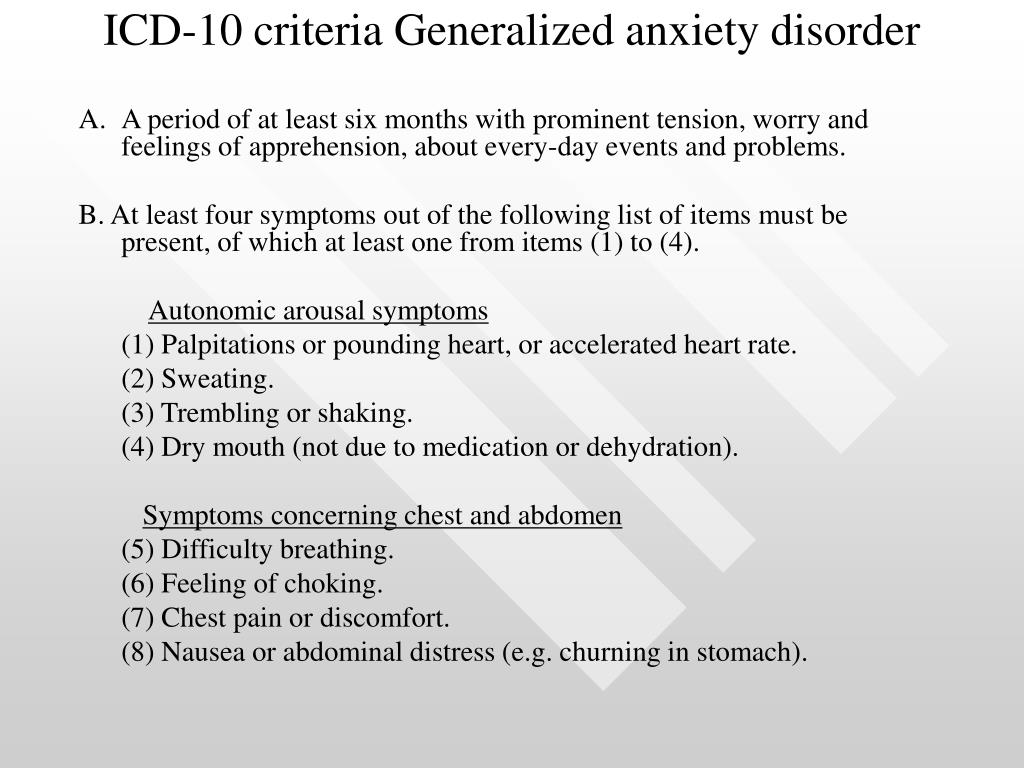
CRITERIA FOR GENERALIZED ANXIETY DISORDER (ICD-10)
A. A period of at least 6 months with marked internal tension, restlessness and a sense of apprehension about everyday events and problems.B. At least 4 symptoms must be present and one of them must be one of the first four:
palpitations or palpitations, sweating, tremors or tremors, dry mouth, difficulty breathing, feeling of choking, chest pain or discomfort, nausea or abdominal discomfort, feeling dizzy or unsteady or fainting, derealization or depersonalization, fear of losing control or craziness, fear of death, hot flashes or chills, numbness or tingling, muscle tension or pain, restlessness or inability to relax, feeling nervous or mentally stressed, sensation of a lump in the throat or difficulty swallowing, increased response to small surprises or fright , difficulty concentrating or "emptiness in the head", constant irritability, difficulty falling asleep due to anxiety.
 nine0015 C. The disorder does not meet the criteria for panic, phobic, obsessive-compulsive disorder, or hypochondriacal disorder.
nine0015 C. The disorder does not meet the criteria for panic, phobic, obsessive-compulsive disorder, or hypochondriacal disorder. D. An anxiety disorder is not due to a medical condition (eg, hyperthyroidism), an organic psychiatric disorder, substance use, or benzodiazepine withdrawal.
CLASSIFICATION OF ANXIETY DISORDERS (ICD-10)
• Agoraphobia [F40.0].• Social phobias [F40.1].
Specific phobias [F40.2]. nine0015 Other phobic anxiety disorders [F40.8].
• Panic disorder [F41.0].
• Generalized anxiety disorder [F41.1].
• Mixed anxiety and depressive disorder [F41.2].
• Obsessive-compulsive disorders [F42].
• Acute stress reaction [F43.0].
Post-traumatic stress disorder [F43.1].
• Mixed anxiety and depressive reaction [F43.22].
Adjustment disorder with predominance of other emotions [F43.23]. nine0015 Organic anxiety disorder [F06.4].
• Other mental and behavioral disorders due to alcohol [F10.8].
Protective role of anxiety in coronary disease
Meyer T, et al.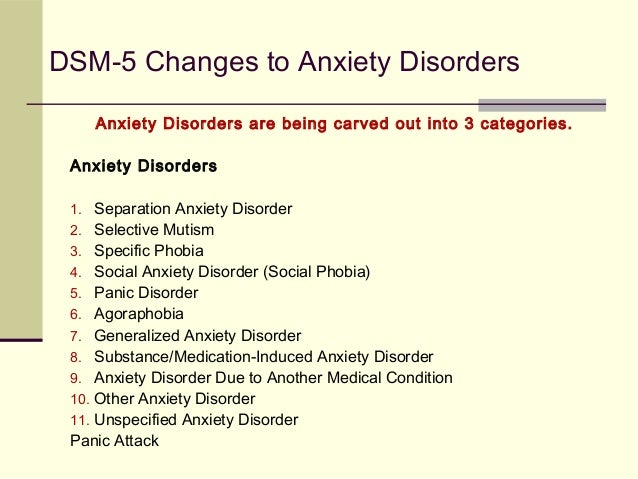 Psychosom Med. 2010;72:9–15.
Psychosom Med. 2010;72:9–15.
FORMULATION OF THE DIAGNOSIS
□ Stable angina I FC. Generalized anxiety disorder. [I20.8]□ Generalized anxiety disorder, irritable bowel syndrome with diarrhea and constipation. [F41.1] nine0015 □ Irritable bowel syndrome with diarrhea and constipation due to generalized anxiety disorder. [K58.0]
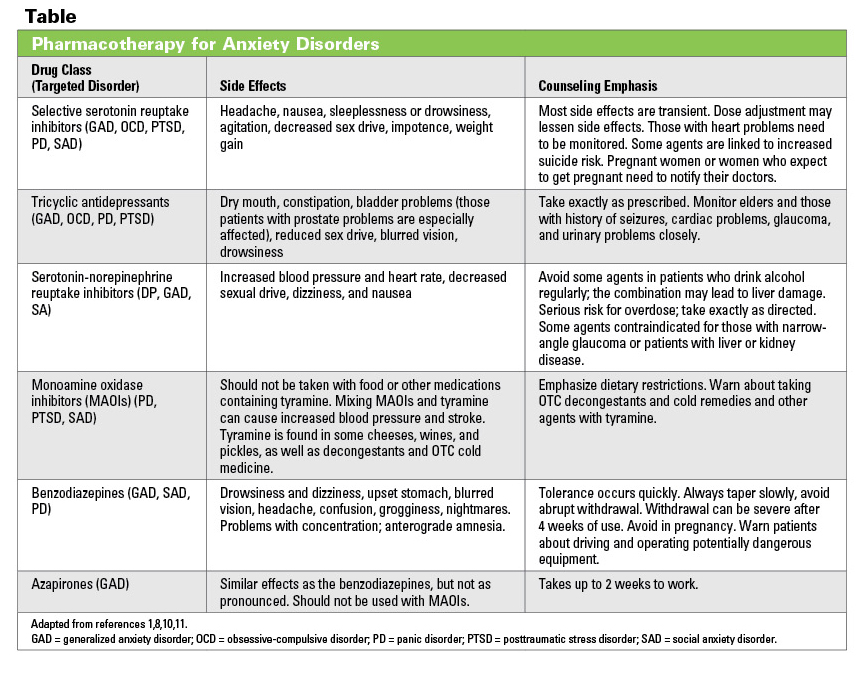
TREATMENT
• Antidepressants >1 year.• Nonbenzodiazepine tranquilizers, clonazepam <3 mo.
• Benzodiazepine tranquilizers <3 weeks.
• Beta-blockers (metoprolol, bisoprolol).
• Psychotherapy.
Anxiety and return visits with cardialgia
Musey Jr P, et al. Am J Card. 2018;7:1133–41. nine0004
TRANQUILIZERS
Benzodiazepines• Diazepam 2–20 mg/day.
• Clonazepam 1.5–6 mg/day in 3 divided doses.
• Lorazepam 2-4 mg/day.
• Phenazepam (bromodihydrochlorophenylbenzodiazepine) 0.5–2 mg/day.
• Chlordiazepoxide 15–100 mg/day.
Non-benzodiazepine
• Alprazolam 0. 5–2 mg 3 times.
5–2 mg 3 times.
• Buspirone 5-20 mg 2-3 times.
• Hydroxyzine 25–100 mg 3 times. nine0015 • Fabomotizol 20 mg 3 times.
Choice of treatment for generalized anxiety
Slee A, et al. Br J Psych. 2021;218:158–64. SSRIs, selective serotonin reuptake inhibitors; SNRIs, serotonin and norepinephrine reuptake inhibitors; TCAs, tricyclic antidepressants.
ANTIDEPRESSANTS
Selective serotonin reuptake inhibitors• Sertraline 25–200 mg/day.
• Fluoxetine 20–60 mg/day. nine0015 • Escitalopram 10–20 mg/day.
Noradrenergic and serotonergic
• Mianserin 30–60 mg/day.
• Mirtazapine 15–45 mg/day.
Other groups
• Amitriptyline, imipramine 50–150 mg/day.
• Venlafaxine 150–225 mg/day.
• Trazodone 75-300 mg/day.
02/26/2021. © Belyalov F.I., 2004–2022.
Anxiety disorder: symptoms, diagnosis and treatment
nine0003 PsychotherapistKrashkina
Irina Ivanovna
Experience 32 years
Psychotherapist, candidate of medical sciences, member of the Russian Professional Psychotherapeutic League
Make an appointment
Anxiety disorder is a type of neurotic condition in which a person experiences continuous anxiety about life circumstances, their appearance and relationships with people around them. Staying in this state for a long time creates uncomfortable living conditions for a person, which become the reason for him to withdraw into himself, not to develop his own abilities and limit his social circle. nine0004
Staying in this state for a long time creates uncomfortable living conditions for a person, which become the reason for him to withdraw into himself, not to develop his own abilities and limit his social circle. nine0004
Symptoms and signs
It is believed that when an anxiety disorder appears, the symptoms are as follows:
- severe form of anxiety and emotional stress before the onset of panic attacks;
- frequent mood swings;
- persistent sleep disorder;
- constant conflicts with others;
- reduced acuity of reactions and inhibited thinking;
- increased sweating, rapid pulse; nine0128
- fatigue and weakness, leading to decreased performance;
- complaints about the appearance of pain in different parts of the body.
These symptoms of an anxiety disorder are signs of autonomic and mental disorders.
The hallmarks of symptoms of generalized anxiety disorder are:
- total manifestation of anxiety before any life circumstances; nine0128
- inability to concentrate on domestic activities or work;
- constant motor voltage;
- inability to relax;
- indigestion and stomach pain;
- heart disease.
Symptoms of an anxiety-depressive disorder occur against the background of constant depression:
- lack of interest in the manifestations of life and close people; nine0127 lack of positive emotions;
- sudden feeling of fear;
- vegetative disorders - rapid pulse, shortness of breath, lack of air, increased sweating, proximity to fainting, etc.
Causes of the onset and development of the disease
Experts believe that the following factors contribute to the appearance of the disease:
- the presence of persistent circulatory disorders, hormonal failures or chronic heart disease; nine0128
- chronic form of dependence on alcohol, drugs, psychoactive substances, as well as a sharp cessation of their use;
- traumatic brain injuries and their consequences;
- being in a situation of prolonged stress;
- character traits - melancholic temperament, disturbing accents in the temperament of the character;
- tendency to exaggerate dangers due to their high susceptibility;
- neurotic and mental disorders: depression, neurasthenia, hysteria, schizophrenia, paranoia, various manias; nine0128
- mental trauma in children at an early age and in adults in extreme situations - war, earthquake, being in a state close to death, loss of a loved one or his support, and others.
Psychologists view the process of anxiety in different ways:
- adherents of psychoanalysis believe that the reason is the regular suppression of their own desires;
- the second believe that the reason is the break in the connection between the stimulus and the response of the psyche to the stimulus; nine0128
- still others believe that the reason is in the reaction of the psyche to the distorted mental images of a person.
Disease classification
Anxiety disorder according to the ICD is a neurotic disorder along with fears, suspiciousness and post-traumatic disorders. One of the main signs of an anxious personality disorder is the pathology of the origin of anxiety, the disproportionate degree of protection to the stimulus factor.
Pathological anxiety: nine0004
- is not caused by a real danger;
- is not proportionate to the significance of the situation;
- is not associated with a lack of time and knowledge;
- is being actively ousted;
- brings significant discomfort to a person's life;
- is much more pronounced than normal;
- is long in time;
- has satellites in the form of tension and expectation of consequences, concern and doubt, feelings of helplessness.
 nine0128
nine0128
Types of anxiety disorder:
- anxiety-depressive disorder is caused by the constant presence of anxiety without sources of danger, it has pathological changes in the patient's personality;
- phobic anxiety disorder is based on dwelling on past unpleasant consequences;
- social anxiety disorder is characterized by the patient's avoidance of contact with other people;
- mixed anxiety disorder causes a simultaneous feeling of pathological anxiety and depressed mood; nine0128
- anxiety-panic disorder is characterized by the presence of panic attacks;
- Anxiety-neurotic disorder is associated with anxiety before any diseases, severe shyness and unrest;
- generalized anxiety disorder is accompanied by excessive fussiness, anxiety without certain dangers and threats.
Risk factors and groups
Risk factors include child abuse, hereditary mental disorders, historical family poverty, or other antisocial manifestations.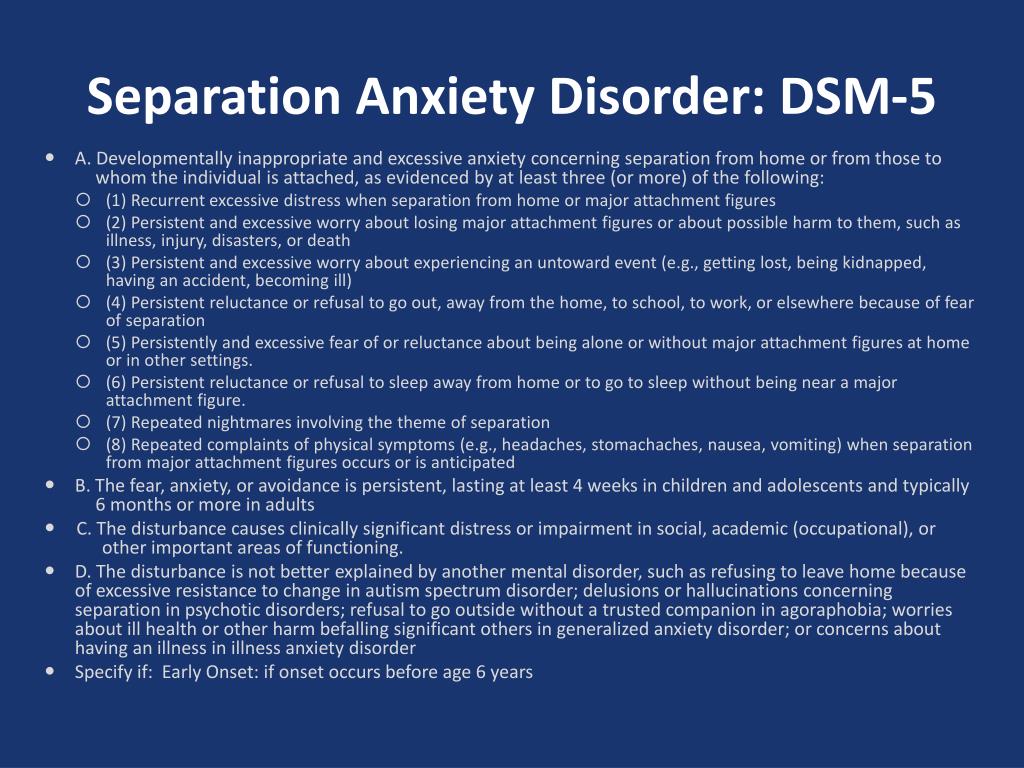 nine0004
nine0004
The risk group includes people prone to neurotic diseases - depression, hysteria; people taking alcohol, drugs, psychotropic drugs; women between the ages of 20 and 30.
Complications
In the absence of adequate treatment, anxiety disorder leads to the following socio-psychological complications:
- low self-esteem;
- self-isolation from society;
- insomnia; nine0128
- the appearance of a feeling of hopelessness;
- exhaustion of the body.
Social complications are job loss, financial problems, relationship breakdown, alcoholism, drug addiction, substance abuse, and others. Physical complications - irritation in the intestines, heartburn, lack of interest in sex, weight loss or excess weight gain, headaches and muscle strain, decreased immunity, the development of allergies, accelerated aging, cancer, heart disease and many others. nine0004
Diagnostics
The accumulated information about this disease made it possible to test reliable methods of drug and psychotherapeutic treatment.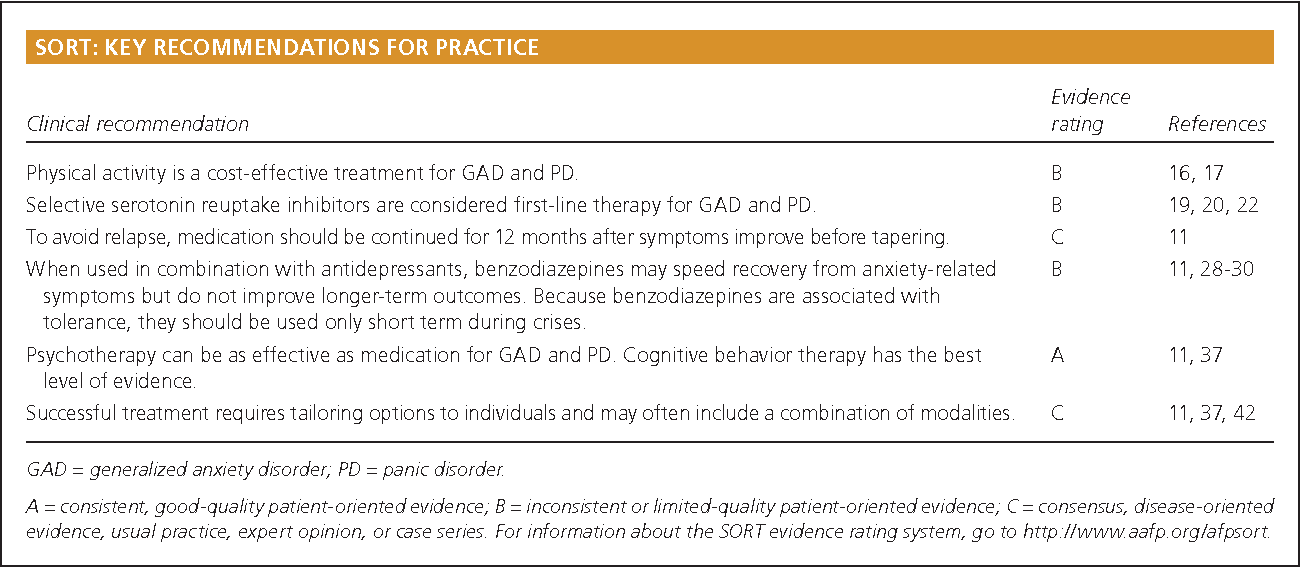 This disease belongs to the areas of professional interest of a psychiatrist and a medical psychologist.
This disease belongs to the areas of professional interest of a psychiatrist and a medical psychologist.
Specialists use the following methods for diagnosing a neurotic disease:
- initial individual consultation involves a survey to identify emotional reactions, obtain information about the patient's lifestyle, motives and interests; nine0128
- psychodiagnostic examination and projective testing aimed at identifying pathological anxiety and related disorders;
- observations of the patient and his life, relationships with the outside world and with people.
Preparing to see a doctor
Before entering the psychotherapist's office, the patient is advised to formulate all his problems, report on the use of all psychoactive substances, including the start/end dates and the total duration of the use. In addition, the positive attitude of the patient to the treatment and the effect that it will bring is extremely important. nine0004
nine0004
Treatment
Anxiety disorders are treated with a complex of methods based on changing the patient's lifestyle, psychotherapy and taking medications. Treatment for generalized anxiety disorder is based on the use of psychoactive-type medications, such as antidepressants. In no case should you arbitrarily stop taking medications. Psychotherapy of anxiety disorder is carried out by various methods - individual, group, family. The main direction of the impact of therapy is an increased impact on the attitude towards the fears and anxieties that have appeared. nine0004
Among traditional medicine, it is possible to use medicinal herbs, infusions and decoctions from them, for example, lemon balm, chamomile. These herbs act on the human body, bringing a relaxing effect, thanks to this effect, anxiety disorders and their cause temporarily reduce their degree of activity.
Self-treatment of an anxiety disorder threatens with pains and neuroses of a different nature, which need to be treated more deeply.