Dysthymia dsm 5 criteria
Dysthymic Disorder: Background, Etiology, Epidemiology
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Washington, DC: American Psychiatric Association; 2013.
Niculescu AB 3rd, Akiskal HS. Proposed endophenotypes of dysthymia: evolutionary, clinical and pharmacogenomic considerations. Mol Psychiatry. 2001 Jul. 6(4):363-6. [QxMD MEDLINE Link].
Keller MB, Harrison W, Fawcett JA, Gelenberg A, Hirschfeld RM, Klein D, et al. Treatment of chronic depression with sertraline or imipramine: preliminary blinded response rates and high rates of undertreatment in the community. Psychopharmacol Bull. 1995. 31(2):205-12. [QxMD MEDLINE Link].
Klein DN, Schwartz JE, Rose S, Leader JB. Five-year course and outcome of dysthymic disorder: A prospective, naturalistic follow-up study.
Am J Psychiatry. 2000 Jun. 157(6):931-9. [QxMD MEDLINE Link].
Klein DN, Shankman SA, Rose S. Ten-year prospective follow-up study of the naturalistic course of dysthymic disorder and double depression. Am J Psychiatry. 2006 May. 163(5):872-80. [QxMD MEDLINE Link].
Kelly O, Matheson K, Ravindran A, Merali Z, Anisman H. Ruminative coping among patients with dysthymia before and after pharmacotherapy. Depress Anxiety. 2007. 24(4):233-43. [QxMD MEDLINE Link].
Hermens ML, van Hout HP, Terluin B, van der Windt DA, Beekman AT, et al. The prognosis of minor depression in the general population: a systematic review. Gen Hosp Psychiatry. 2004 Nov-Dec. 26(6):453-62. [QxMD MEDLINE Link].
Johnson JG, Cohen P, Kasen S, Brook JS. Personality disorder traits associated with risk for unipolar depression during middle adulthood.
 Psychiatry Res. 2005 Sep 15. 136(2-3):113-21. [QxMD MEDLINE Link].
Psychiatry Res. 2005 Sep 15. 136(2-3):113-21. [QxMD MEDLINE Link]. Ho PS, Yen CH, Chen CY, Huang SY, Liang CS. Changes in cytokine and chemokine expression distinguish dysthymic disorder from major depression and healthy controls. Psychiatry Res. 2017 Feb. 248:20-27. [QxMD MEDLINE Link].
Riolo SA, Nguyen TA, Greden JF, King CA. Prevalence of depression by race/ethnicity: findings from the National Health and Nutrition Examination Survey III. Am J Public Health. 2005 Jun. 95(6):998-1000. [QxMD MEDLINE Link].
Shankman SA, Klein DN. The impact of comorbid anxiety disorders on the course of dysthymic disorder: a 5-year prospective longitudinal study. J Affect Disord. 2002 Jul. 70(2):211-7. [QxMD MEDLINE Link].
Laptook RS, Klein DN, Dougherty LR.
 Ten-year stability of depressive personality disorder in depressed outpatients. Am J Psychiatry. 2006 May. 163(5):865-71. [QxMD MEDLINE Link].
Ten-year stability of depressive personality disorder in depressed outpatients. Am J Psychiatry. 2006 May. 163(5):865-71. [QxMD MEDLINE Link]. Hayden EP, Klein DN. Outcome of dysthymic disorder at 5-year follow-up: the effect of familial psychopathology, early adversity, personality, comorbidity, and chronic stress. Am J Psychiatry. 2001 Nov. 158(11):1864-70. [QxMD MEDLINE Link].
Markowitz JC, Skodol AE, Petkova E, Xie H, Cheng J, Hellerstein DJ, et al. Longitudinal comparison of depressive personality disorder and dysthymic disorder. Compr Psychiatry. 2005 Jul-Aug. 46(4):239-45. [QxMD MEDLINE Link].
Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report.
 Am J Psychiatry. 2006 Nov. 163(11):1905-17. [QxMD MEDLINE Link].
Am J Psychiatry. 2006 Nov. 163(11):1905-17. [QxMD MEDLINE Link]. Rush AJ, Kraemer HC, Sackeim HA, et al. Report by the ACNP Task Force on response and remission in major depressive disorder. Neuropsychopharmacology. 2006 Sep. 31(9):1841-53. [QxMD MEDLINE Link].
Adler DA, Irish J, McLaughlin TJ, Perissinotto C, Chang H, Hood M, et al. The work impact of dysthymia in a primary care population. Gen Hosp Psychiatry. 2004 Jul-Aug. 26(4):269-76. [QxMD MEDLINE Link].
Lerner D, Adler DA, Chang H, Lapitsky L, Hood MY, Perissinotto C. Unemployment, job retention, and productivity loss among employees with depression. Psychiatr Serv. 2004 Dec. 55(12):1371-8. [QxMD MEDLINE Link].
Barbui C, Motterlini N, Garattini L. Health status, resource consumption, and costs of dysthymia.
 A multi-center two-year longitudinal study. J Affect Disord. 2006 Feb. 90(2-3):181-6. [QxMD MEDLINE Link].
A multi-center two-year longitudinal study. J Affect Disord. 2006 Feb. 90(2-3):181-6. [QxMD MEDLINE Link]. Bernal M, Haro JM, Bernert S, Brugha T, de Graaf R, Bruffaerts R, et al. Risk factors for suicidality in Europe: results from the ESEMED study. J Affect Disord. 2007 Aug. 101(1-3):27-34. [QxMD MEDLINE Link].
Bakken K, Vaglum P. Predictors of suicide attempters in substance-dependent patients: a six-year prospective follow-up. Clin Pract Epidemol Ment Health. 2007. 3:20. [QxMD MEDLINE Link].
Casement MD, Shestyuk AY, Best JL, Casas BR, Glezer A, Segundo MA, et al. Anticipation of affect in dysthymia: behavioral and neurophysiological indicators. Biol Psychol. 2008 Feb. 77(2):197-204. [QxMD MEDLINE Link].
Klein DN, Shankman SA, Lewinsohn PM, Rohde P, Seeley JR.
 Family study of chronic depression in a community sample of young adults. Am J Psychiatry. 2004 Apr. 161(4):646-53. [QxMD MEDLINE Link].
Family study of chronic depression in a community sample of young adults. Am J Psychiatry. 2004 Apr. 161(4):646-53. [QxMD MEDLINE Link]. Keitner GI, Ryan CE, Solomon DA. Realistic expectations and a disease management model for depressed patients with persistent symptoms. J Clin Psychiatry. 2006 Sep. 67(9):1412-21. [QxMD MEDLINE Link].
Airaksinen E, Larsson M, Lundberg I, Forsell Y. Cognitive functions in depressive disorders: evidence from a population-based study. Psychol Med. 2004 Jan. 34(1):83-91. [QxMD MEDLINE Link].
Leichsenring F, Hiller W, Weissberg M, Leibing E. Cognitive-behavioral therapy and psychodynamic psychotherapy: techniques, efficacy, and indications. Am J Psychother. 2006. 60(3):233-59. [QxMD MEDLINE Link].
Leichsenring F, Leibing E. Psychodynamic psychotherapy: a systematic review of techniques, indications and empirical evidence. Psychol Psychother. 2007 Jun. 80:217-28. [QxMD MEDLINE Link].
Markowitz JC, Bleiberg KL, Christos P, Levitan E. Solving interpersonal problems correlates with symptom improvement in interpersonal psychotherapy: preliminary findings. J Nerv Ment Dis. 2006 Jan. 194(1):15-20. [QxMD MEDLINE Link].
Markowitz JC, Kocsis JH, Bleiberg KL, Christos PJ, Sacks M. A comparative trial of psychotherapy and pharmacotherapy for "pure" dysthymic patients. J Affect Disord. 2005 Dec. 89(1-3):167-75. [QxMD MEDLINE Link].
Bolton P, Bass J, Neugebauer R, Verdeli H, Clougherty KF, Wickramaratne P. Group interpersonal psychotherapy for depression in rural Uganda: a randomized controlled trial.
 JAMA. 2003 Jun 18. 289(23):3117-24. [QxMD MEDLINE Link].
JAMA. 2003 Jun 18. 289(23):3117-24. [QxMD MEDLINE Link]. Johnson JE, Zlotnick C. A pilot study of group interpersonal psychotherapy for depression in substance-abusing female prisoners. J Subst Abuse Treat. 2008 Jun. 34(4):371-7. [QxMD MEDLINE Link].
Comparative Effectiveness of Second-Generation Antidepressants in the Pharmacologic Treatment of Adult Depression. Accessed: May 19, 2009. AHRQ: Agency for Healthcare Research and Quality. Jan. 24, 2007. Available at http://www.effectivehealthcare.ahrq.gov/index.cfm/search-for-guides-reviews-and-reports/?pageaction=displayproduct&productid=61.
Carvalho AF, Cavalcante JL, Castelo MS, Lima MC. Augmentation strategies for treatment-resistant depression: a literature review. J Clin Pharm Ther. 2007 Oct. 32(5):415-28. [QxMD MEDLINE Link].
Lifschytz T, Segman R, Shalom G, Lerer B, Gur E, Golzer T, et al. Basic mechanisms of augmentation of antidepressant effects with thyroid hormone. Curr Drug Targets. 2006 Feb. 7(2):203-10. [QxMD MEDLINE Link].
Tuunainen A, Kripke DF, Endo T. Light therapy for non-seasonal depression. Cochrane Database Syst Rev. 2004. CD004050. [QxMD MEDLINE Link].
McCullough JP Jr, Klein DN, Borian FE, Howland RH, Riso LP, Keller MB, et al. Group comparisons of DSM-IV subtypes of chronic depression: validity of the distinctions, part 2. J Abnorm Psychol. 2003 Nov. 112(4):614-22. [QxMD MEDLINE Link].
Kessing LV. Epidemiology of Subtypes of Depression. Acta Psychiatr Scand. 2007. 115 (Suppl 433):85-89.
Murphy JA, Byrne GJ. Prevalence and correlates of the proposed DSM-5 diagnosis of Chronic Depressive Disorder. J Affect Disord. 2012 Feb 29. [QxMD MEDLINE Link].
Olfson M, Liu SM, Grant BF, Blanco C. Influence of comorbid mental disorders on time to seeking treatment for major depressive disorder. Med Care. 2012 Mar. 50(3):227-32. [QxMD MEDLINE Link]. [Full Text].
Ryder AG, Schuller DR, Bagby RM. Depressive personality and dysthymia: evaluating symptom and syndrome overlap. J Affect Disord. 2006 Apr. 91(2-3):217-27. [QxMD MEDLINE Link].
Masi G, Millepiedi S, Mucci M, Pascale RR, Perugi G, Akiskal HS. Phenomenology and comorbidity of dysthymic disorder in 100 consecutively referred children and adolescents: beyond DSM-IV. Can J Psychiatry. 2003 Mar. 48(2):99-105. [QxMD MEDLINE Link].
Hellerstein DJ, Batchelder S, Miozzo R, Kreditor D, Hyler S, Gangure D. Citalopram in the treatment of dysthymic disorder. Int Clin Psychopharmacol. 2004 May. 19(3):143-8. [QxMD MEDLINE Link].
Persistent depressive disorder - Symptoms and causes
Overview
Persistent depressive disorder is a continuous, long-term form of depression. You may feel sad and empty, lose interest in daily activities and have trouble getting things done. You may also have low self-esteem, feel like a failure and feel hopeless. These feelings last for years and may interfere with your relationships, school, work and daily activities.
If you have persistent depressive disorder, you may find it hard to be upbeat even on happy occasions. You may be described as having a gloomy personality, constantly complaining or not able to have fun. Persistent depressive disorder is not as severe as major depression, but your current depressed mood may be mild, moderate or severe.
Because persistent depressive disorder is long term, coping with depression symptoms can be challenging. A combination of talk therapy and medicine can be effective in treating this condition.
Products & Services
- Book: Mayo Clinic Family Health Book, 5th Edition
- Newsletter: Mayo Clinic Health Letter — Digital Edition
Symptoms
Persistent depressive disorder symptoms usually come and go over a period of years. The intensity of symptoms can change over time. But symptoms usually don't disappear for more than two months at a time. Also, major depression episodes may occur before or during persistent depressive disorder.
Symptoms of persistent depressive disorder can cause major problems in your life and may include:
- Sadness, emptiness or feeling down.
- Loss of interest in daily activities.
- Tiredness and lack of energy.
- Low self-esteem, self-criticism or feeling you're not capable.
- Trouble focusing clearly and trouble making decisions.
- Problems getting things done well and on time.
- Quickly becoming annoyed, impatient or angry.
- Avoidance of social activities.
- Feelings of guilt and worries over the past.
- Poor appetite or overeating.
- Sleep problems.
- Hopelessness.
In children, symptoms of persistent depressive disorder may include depressed mood and being irritable, which means easily becoming annoyed, impatient or angry.
When to see a doctor
If these feelings have been going on for a long time, you may think they'll always be part of your life. But if you have any symptoms of persistent depressive disorder, seek medical help.
Talk to your health care provider about your symptoms or seek help from a mental health professional. Or you can reach out to someone else who may be able to help guide you to treatment. This could be a friend or loved one, a teacher, a faith leader, or another person you trust.
If you think you may hurt yourself or attempt suicide, call 911 in the U.S. or your local emergency number immediately. Or contact a suicide hotline. In the U.S., call or text 988 to reach the 988 Suicide & Crisis Lifeline, available 24 hours a day, seven days a week. Or use the Lifeline Chat. Services are free and confidential. The Suicide & Crisis Lifeline in the U.S. has a Spanish language phone line at 888-628-9454 (toll-free).
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.
To provide you with the most relevant and helpful information, and understand which
information is beneficial, we may combine your email and website usage information with
other information we have about you. If you are a Mayo Clinic patient, this could
include protected health information. If we combine this information with your protected
health information, we will treat all of that information as protected health
information and will only use or disclose that information as set forth in our notice of
privacy practices. You may opt-out of email communications at any time by clicking on
the unsubscribe link in the e-mail.
If you are a Mayo Clinic patient, this could
include protected health information. If we combine this information with your protected
health information, we will treat all of that information as protected health
information and will only use or disclose that information as set forth in our notice of
privacy practices. You may opt-out of email communications at any time by clicking on
the unsubscribe link in the e-mail.
Causes
The exact cause of persistent depressive disorder is not known. As with major depression, it may involve more than one cause, such as:
- Biological differences. People with persistent depressive disorder may have physical changes in their brains. It's not clear how these changes affect the disorder, but they may eventually help determine the causes.
- Brain chemistry. Neurotransmitters are naturally occurring brain chemicals. Research indicates that changes in neurotransmitters may play a large part in depression and its treatment.
- Inherited traits. Persistent depressive disorder appears to be more common in people whose blood relatives also have the condition. Researchers are trying to find genes that may be involved in causing depression.
- Life events. As with major depression, traumatic events such as the loss of a loved one, financial problems or a high level of stress can trigger persistent depressive disorder in some people.
Risk factors
Persistent depressive disorder often begins early — in childhood, the teen years or young adult life — and continues for a long time. Certain factors appear to increase the risk of developing persistent depressive disorder, including:
- Having a first-degree blood relative, such as a parent or sibling, with major depressive disorder or other depressive disorders.
- Traumatic or stressful life events, such as the loss of a loved one or major financial problems.
- Personality traits that include negativity, such as low self-esteem, being too dependent or self-critical, or always thinking the worst will happen.
- History of other mental health disorders, such as a personality disorder.
Complications
Conditions that may be linked with persistent depressive disorder include:
- Lower quality of life.
- Major depression, anxiety disorders and other mood disorders.
- Substance misuse.
- Relationship difficulties and family conflicts.
- School or work problems and trouble getting things done.
- Continuing pain and general medical illnesses.
- Suicidal thoughts or behavior.
- Personality disorders or other mental health disorders.
Prevention
There's no sure way to prevent persistent depressive disorder. Because it often starts in childhood or during the teenage years, identifying children at risk of the condition may help them get early treatment.
Because it often starts in childhood or during the teenage years, identifying children at risk of the condition may help them get early treatment.
Strategies that may help reduce or prevent symptoms include the following:
- Take steps to control stress, to increase your ability to recover from problems — which is called resilience — and to boost your self-esteem.
- Reach out to family and friends, especially in times of crisis, to help you get through rough spells.
- Get treatment at the earliest sign of a problem to help prevent symptoms from worsening.
- Consider getting long-term treatment to help prevent a relapse of symptoms.
By Mayo Clinic Staff
Related
Associated Procedures
Products & Services
New American classification of mental disorders DSM-5 released to the world
Home > News > The new American classification of mental disorders DSM-5 is released to the world
| DSM-5 consists of three sections: it is (1) an introductory part with instructions for use and a warning about the forensic psychiatric use of the DSM-5; (2) diagnostic criteria and codes for routine clinical use; and (3) tools and techniques to inform clinical decision making. Major changes:
The severity of the disorder is not determined by IQ, but by the level of adaptive functioning. Speech disorders have entered the new category "social communication disorder", in which some of the syndromes coincide with "autism spectrum disorder". The category "Autism Spectrum Disorders" replaces the DSM-4 diagnoses of autism, Asperger's syndrome, childhood disintegrative disorder, and an unspecified general developmental disorder, all of which cease to exist as separate diagnoses. ADHD can start later (before 12) and is treated differently in different areas. Learning disorders and movement disorders are organized differently in this chapter and somewhat combined. nine0003
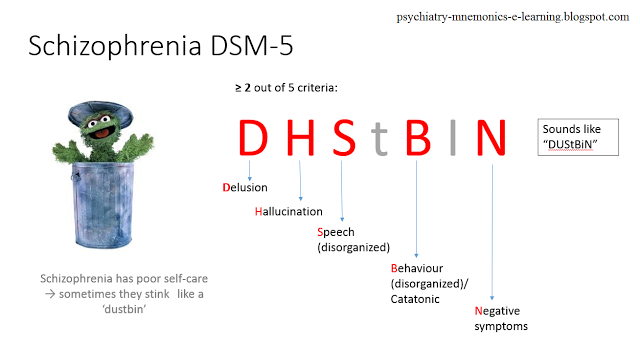
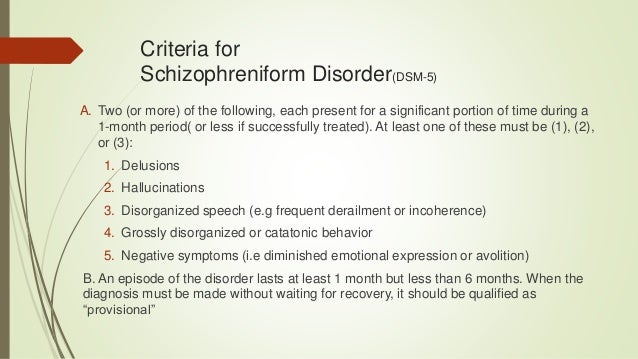
For the diagnosis of schizophrenia, symptoms of the first Schneider rank lose their special weight. One positive symptom is required for a diagnosis to be made.
Bipolar and related disorders are now separated from depressive disorders and placed in a separate category. A clearer definition of mania is given and refinements for mixed episodes are introduced, which lowers the threshold for disorder. Added a residual subcategory ""other"" and a qualifying score for anxiety symptoms.
Disruptive mood dysregulation disorder and premenstrual dysphoric disorder added. Chronic depression and dysthymia are combined into one diagnosis, now it is ""persistent depressive disorder (dysthymia)"" with a number of clarifying indicators.
|
 nine0003
nine0003 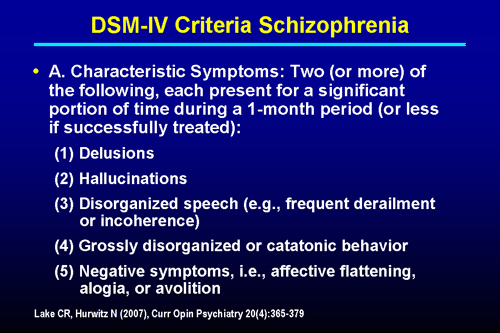 Subtypes are removed - in favor of the dimensional indicator of severity. For schizoaffective disorder, the mood aspect is emphasized, and for delusional disorder, frivolous content is no longer excluded – although it is evaluated separately. The "catatonia" section has been expanded: this code can now be entered as an adjacent diagnosis (specifying indicator) for depressive, bipolar and psychotic disorders. nine0003
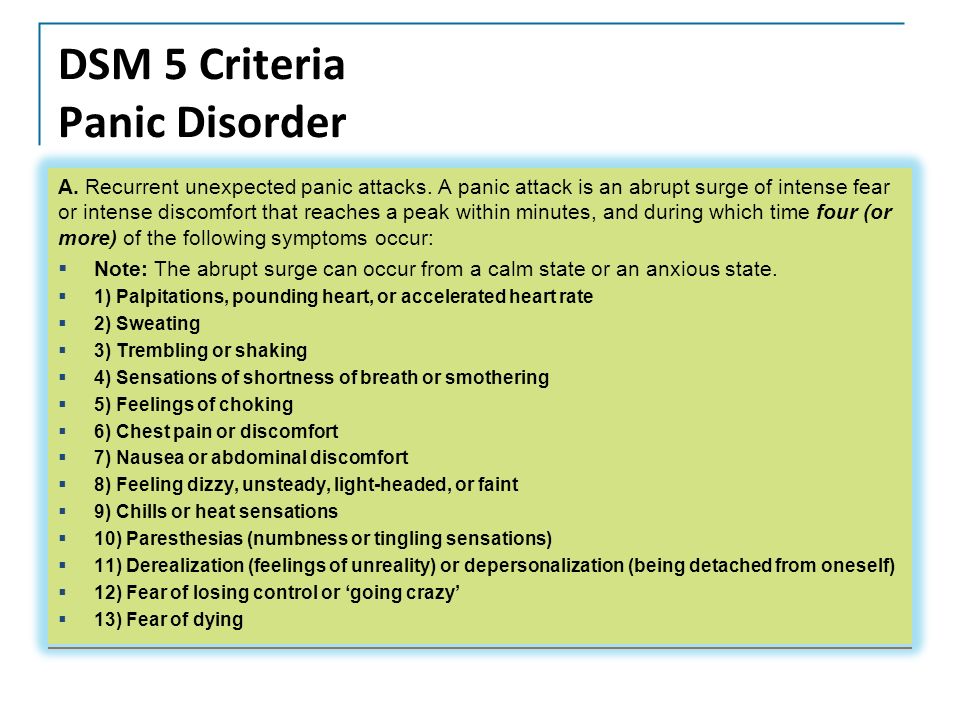
Subtypes are removed - in favor of the dimensional indicator of severity. For schizoaffective disorder, the mood aspect is emphasized, and for delusional disorder, frivolous content is no longer excluded – although it is evaluated separately. The "catatonia" section has been expanded: this code can now be entered as an adjacent diagnosis (specifying indicator) for depressive, bipolar and psychotic disorders. nine0003 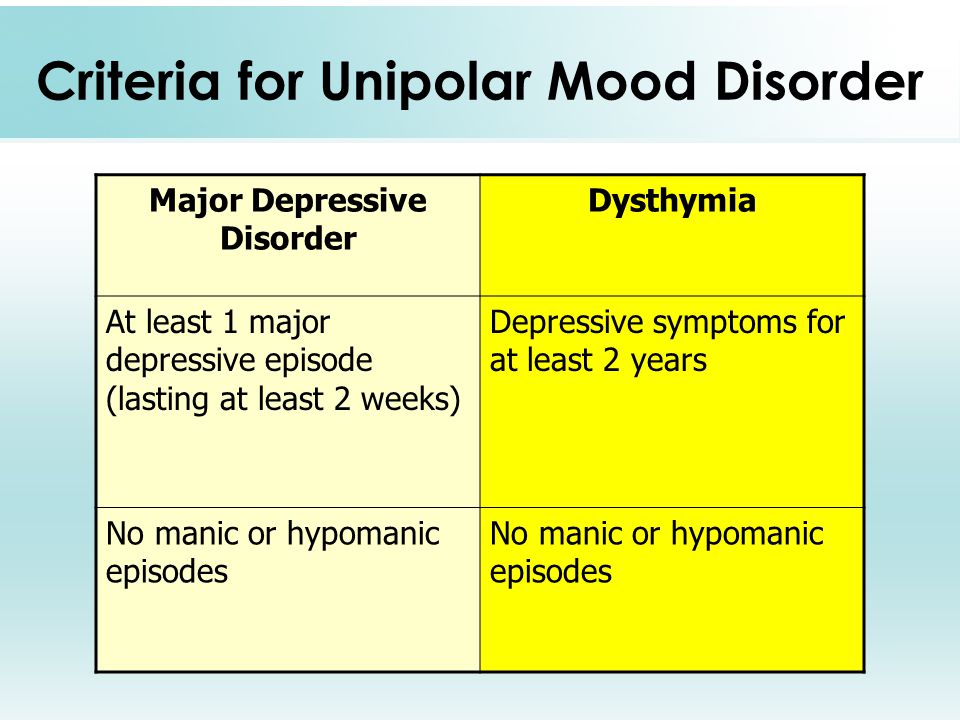 Major depressive disorder remained virtually unchanged, however, for "subthreshold" symptoms, a clarifying indicator ""mixed manifestations"" was introduced. A clarifying indicator for anxious distress has also been introduced. Removed grounds for exclusion for grief. nine(see below) Various phobia criteria are slightly adapted, and agoraphobia and panic are decoupled. Panic attacks can act as a clarifying indicator for other diagnoses. The diagnoses of separation anxiety disorder and selective mutism are no longer specific "childhood" diagnoses. nine0003
Major depressive disorder remained virtually unchanged, however, for "subthreshold" symptoms, a clarifying indicator ""mixed manifestations"" was introduced. A clarifying indicator for anxious distress has also been introduced. Removed grounds for exclusion for grief. nine(see below) Various phobia criteria are slightly adapted, and agoraphobia and panic are decoupled. Panic attacks can act as a clarifying indicator for other diagnoses. The diagnoses of separation anxiety disorder and selective mutism are no longer specific "childhood" diagnoses. nine0003  nine0003
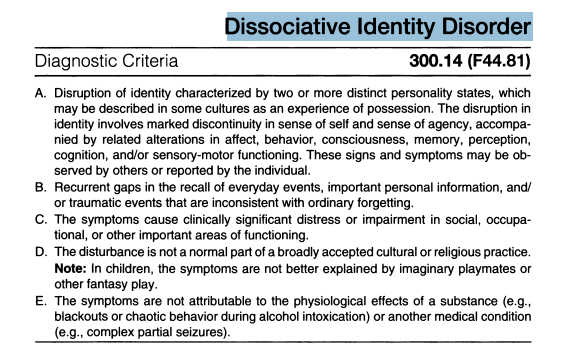
nine0003  Depersonalization and derealization are combined into one disorder. Dissociative fugues have ceased to be a separate diagnosis, and have become a clarifying indicator in ""dissociative amnesia"".
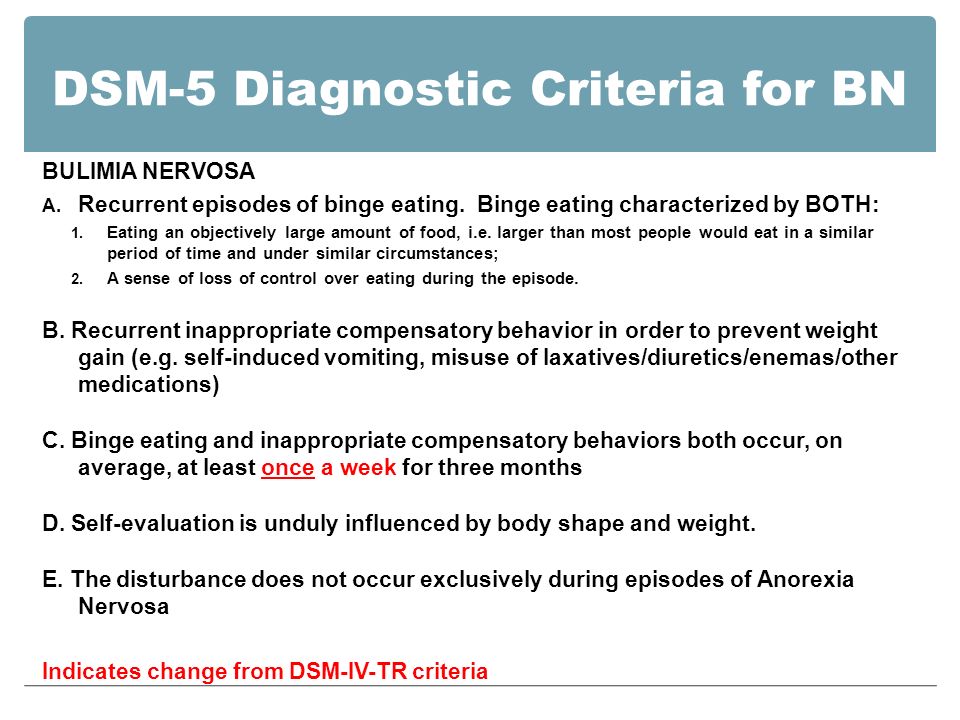
Depersonalization and derealization are combined into one disorder. Dissociative fugues have ceased to be a separate diagnosis, and have become a clarifying indicator in ""dissociative amnesia"".  Anorexia no longer requires amenorrhea and binge eating episodes, although for bulimia nervosa and the new Binge-Eating Disorder category, binge eating episodes must occur at least once a week. nine0003
Anorexia no longer requires amenorrhea and binge eating episodes, although for bulimia nervosa and the new Binge-Eating Disorder category, binge eating episodes must occur at least once a week. nine0003  All disorders are subtyped according to psychological or combined factors, situation, and achievement.
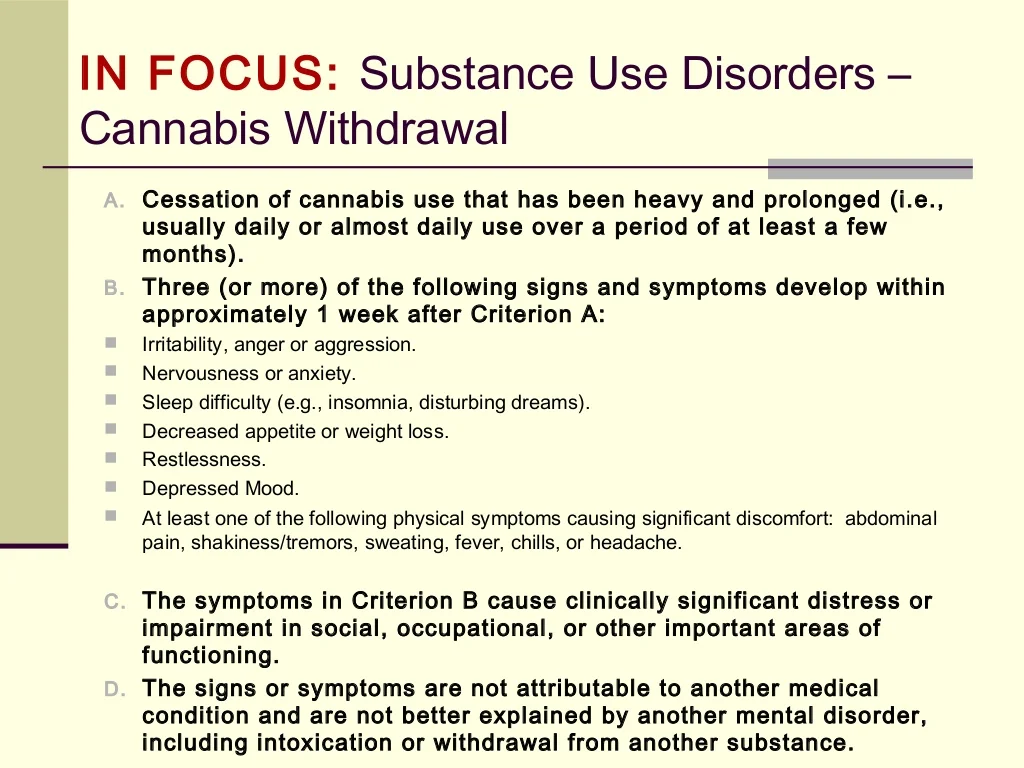
All disorders are subtyped according to psychological or combined factors, situation, and achievement. 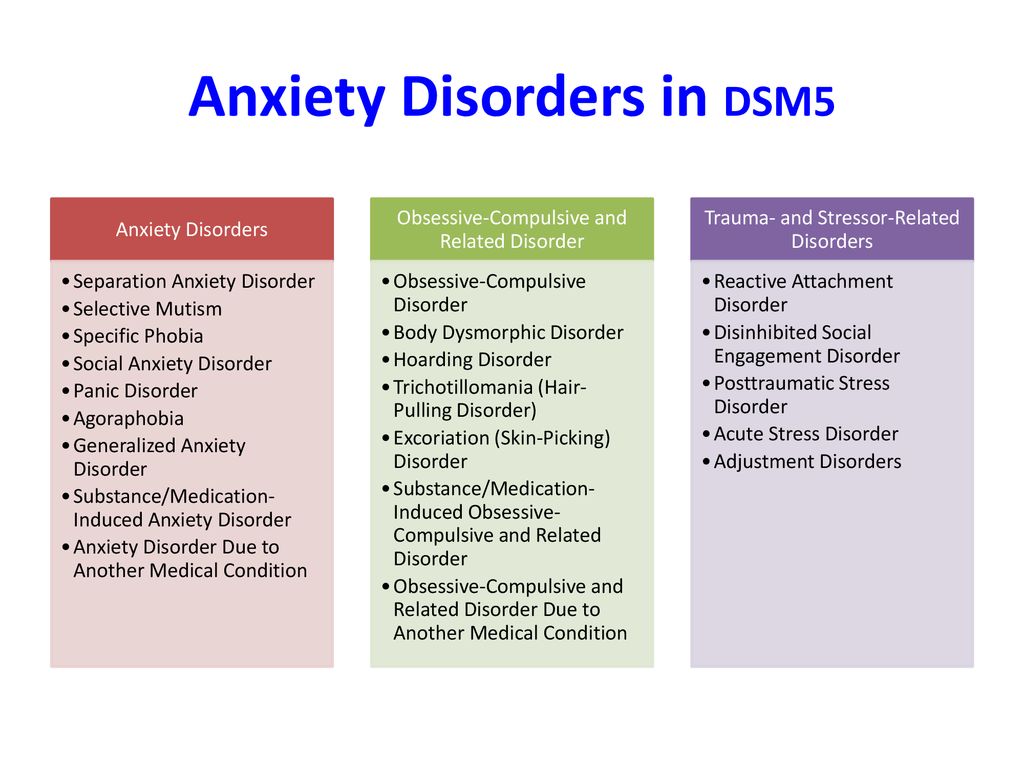 For chemicals, abuse and dependence are combined under the name Substance Use Disorder. "Craving" appears as a criterion, and problems with the justice authorities have been removed. There was a new code for tobacco related disorders, while caffeine was already in the DSM-IV TR. There is a measure of severity, as well as a mention of ""under controlled circumstances"" or ""as maintenance treatment"" (for methadone). nine0003
For chemicals, abuse and dependence are combined under the name Substance Use Disorder. "Craving" appears as a criterion, and problems with the justice authorities have been removed. There was a new code for tobacco related disorders, while caffeine was already in the DSM-IV TR. There is a measure of severity, as well as a mention of ""under controlled circumstances"" or ""as maintenance treatment"" (for methadone). nine0003 ISSN 2588-0519 (Print)
ISSN 2618-8473 (Online)
Major depressive disorders (clinical depression)
Depression is distinct from everyday problems of normal emotional responses and short-term mood swings. Prolonged moderate to severe depression can become a serious illness. This results in patients suffering greatly and doing poorly at work, at school and have problems in their families. At its worst, depression can lead to suicide. nine0003
This results in patients suffering greatly and doing poorly at work, at school and have problems in their families. At its worst, depression can lead to suicide. nine0003
Depression is a common illness worldwide, affecting more than 264 million people. Major depressive disorder is one of the most common forms of mental illness, affecting approximately one in six men and one in four women in their lives.
Major depressive disorder (MDD) is a severe condition characterized by low mood, decreased interests, poor cognitive function, and autonomic symptoms such as disturbed sleep or eating. MDD can develop in one in six adults during their lifetime and affects about twice as many women as men. nine0003
Major symptoms of depressive disorder
Symptoms of major depressive disorder (MDD) may include:
- depression almost every day
- loss of interest in activities you once enjoyed
- changes in appetite or weight
- sleep problems
- feeling lazy or restless
- low energy
- feelings of hopelessness or worthlessness
- trouble concentrating
- frequent thoughts of death or suicide
Depressive relapses:
This is a highly relapsing condition: at least 50% of people recovering from a first episode of depression have at least one additional episode in their lifetime, and about 80% of people have a history of two recurrent episodes.
Episodes typically recur within five years of the first episode, and the average person with a history of depression will have five to nine depressive episodes in their lifetime. nine0003
Symptoms of recurrent depression:
- difficulty concentrating
- disturbed sleep
- reduced energy levels
- permanent light alarm
Major depression in adults:
Depression is a common adult disorder that often leads to poor quality of life and impaired role functioning. Depression is also associated with high rates of suicidal behavior and death. When depression occurs in the context of a medical illness, it is associated with increased healthcare costs, longer hospital stays, poor collaboration in treatment, etc.
Causes of depression in adults may be related to the difficulty of changing roles:
- low education and low income
- early pregnancy and childbirth
- divorces
- unstable operation
- highly competitive and intense work
Major symptoms of depression in adults include:
- Mostly sad or depressed mood
- Loss of interest or pleasure and avoidance of social gatherings
- Decreased energy and frequent fatigue
- Decreased concentration and attention
- Decreased self-esteem and self-confidence
- Thoughts on guilt and unworthiness
- A gloomy and pessimistic view of the future
- Thoughts or actions of harming oneself or suicidal thoughts
- Sleep disturbance or insomnia
- Great or reduced appetite
DSM-5 Criteria for Major Depressive Disorder
According to the DSM-5, the following criteria must be met for a diagnosis of major depression:
At least five of the following symptoms must have been present for at least two weeks and reflect a change in previous functionality.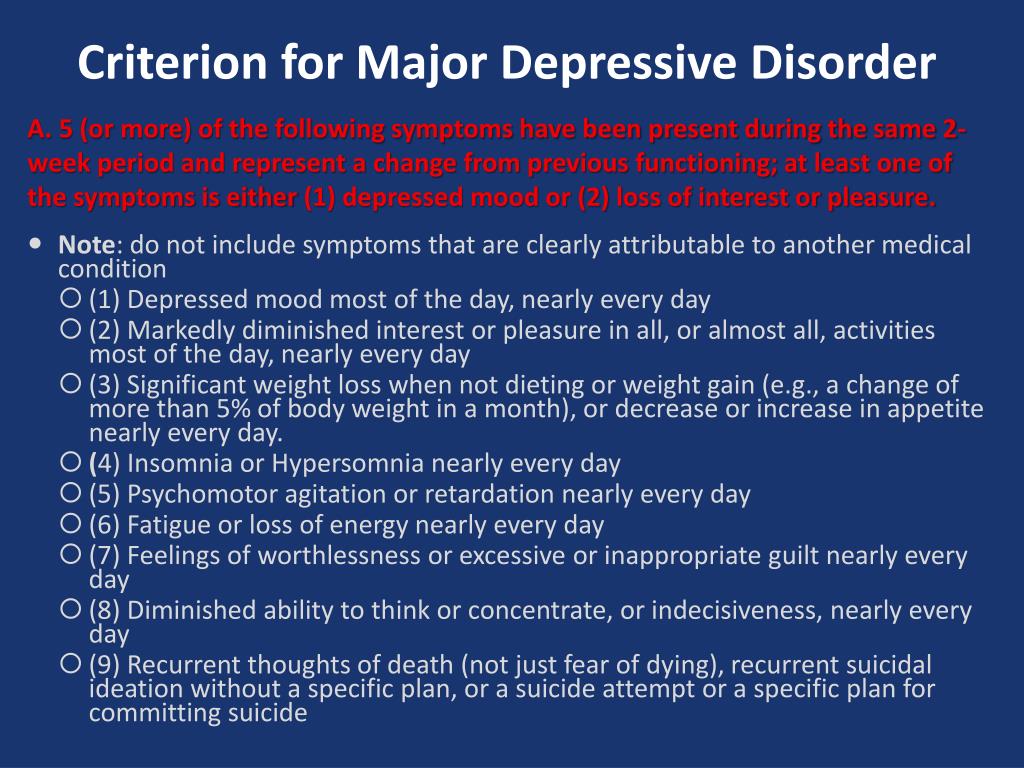 In addition, at least one of the symptoms is a low mood or loss of interest or pleasure.
In addition, at least one of the symptoms is a low mood or loss of interest or pleasure.
- The person is depressed most of the day, almost every day, as noted by himself or others. nine0015
- He or she is not interested in all or most activities most of the day, almost every day.
- Every day a person gains or loses a large amount of weight or has a decreased or increased appetite.
- Almost every day he or she suffers from insomnia or hypersomnia.
- Every day a person develops psychomotor disturbances that are visible to others and can also be reported.
- Almost every day he or she feels exhausted or tired. nine0015
- Almost every day a person has thoughts of worthlessness or guilt.
- Every day a person's ability to think, concentrate, or make judgments deteriorates.
- He or she has recurrent suicidal thoughts, suicidal thoughts (without a definite plan), a suicide attempt, or a definite plan to commit suicide.
- Symptoms listed above cause clinical distress or interfere with daily activities. nine0015
- The episode of depression is not associated with the physiological effect of the drug or other disease.
- The onset of the episode is not better explained by specific or unspecified schizophrenia spectrum illness or other psychotic disorders.
- The person has never had a manic or hypomanic episode.
The diagnostic code for major depressive disorder is based on the frequency of recurrent episodes, the severity of the episodes, the presence of psychotic characteristics, and the state of remission. Below are the varieties of depression:
Severity of depression:
- Minor
- Moderate
- Heavy
- Psychotic
- In partial remission
- In complete remission
- Undefined
Epidemiology
Major depressive illness is a common mental illness. Its lifetime prevalence ranges from 5 to 17 percent. The incidence in women is about twice as high as in men. This is due to hormonal variations, the consequences of childbearing, different psychological pressures in men and women, and a behavioral model of learned helplessness. Although the median age of onset is around 40 years old, new studies show an increase in the incidence among younger populations due to the use of alcohol and other psychoactive substances. nine0003
The incidence in women is about twice as high as in men. This is due to hormonal variations, the consequences of childbearing, different psychological pressures in men and women, and a behavioral model of learned helplessness. Although the median age of onset is around 40 years old, new studies show an increase in the incidence among younger populations due to the use of alcohol and other psychoactive substances. nine0003
MDD is more common in divorced, separated, or bereaved individuals who do not have meaningful interpersonal interactions. There is no difference in the prevalence of MDD between races or socioeconomic status. People with MDD often have comorbidities such as substance abuse, panic disorder, social anxiety disorder, and obsessive-compulsive disorder.
The presence of these comorbidities in people with MDD increases the risk of suicide. Depression is more common in older people with underlying medical problems. Depression is more common in rural areas than in cities. nine0003
nine0003
Pathophysiology of major depressive disorder
The genesis of major depressive disorder is believed to be multifaceted, with biological, genetic, environmental and psychological factors at play. It used to be thought that MDD was caused mainly by abnormalities in neurotransmitters, especially serotonin, norepinephrine, and dopamine.
This has been demonstrated by the use of several antidepressants in the treatment of depression, such as selective serotonin receptor inhibitors, serotonin-norepinephrine receptor inhibitors, and dopamine-norepinephrine receptor inhibitors. Serotonin metabolites have been found to decrease in people who have had suicidal thoughts. However, recent hypotheses suggest that this is largely due to more complex neuroregulatory systems and brain circuits, leading to subsequent disruption of the neurotransmitter systems. nine0003
GABA, an inhibitory neurotransmitter, as well as glutamate and glycine, important excitatory neurotransmitters, have been shown to play a role in the genesis of depression. Depressed people have reduced plasma, cerebrospinal fluid, and brain levels of GABA. GABA is believed to act as an antidepressant by blocking the ascending monoamine pathways, including the mesocortical and mesolimbic systems.
Depressed people have reduced plasma, cerebrospinal fluid, and brain levels of GABA. GABA is believed to act as an antidepressant by blocking the ascending monoamine pathways, including the mesocortical and mesolimbic systems.
The antidepressant properties of drugs that oppose NMDA receptors have been investigated. Thyroid and growth hormone imbalances have also been linked to mood disorders. Numerous adversity and trauma in childhood have been linked to the development of depression later in life. nine0003
Severe early stress can cause dramatic changes in neuroendocrine and behavioral responses, leading to anatomical abnormalities in the cerebral cortex and severe depression later in life. Structural functional tomography of the brain in people with depression revealed greater hyperintensity in the subcortical regions and a decrease in the metabolism of the anterior brain regions on the left.
Family, adoption and twin studies have shown that genes play a role in the risk of depression. According to genetic studies, twins with MDD have a very high level of concordance, especially monozygotic twins. Life experience and personal qualities also have an impact. nine0003
According to genetic studies, twins with MDD have a very high level of concordance, especially monozygotic twins. Life experience and personal qualities also have an impact. nine0003
According to the theory of learned helplessness, the onset of depression is associated with the experience of uncontrollable events. Depression, according to cognitive theory, results from cognitive errors in those who are predisposed to depression.
Somatic illnesses associated with depression
Somatic sensations are especially common in depression and other mental illnesses. Although somatic symptoms are common in depressed individuals, they are of much lesser importance than major depressive symptoms in the diagnosis of depression. nine0003
The clinical stages of sad mood are characterized by both painful and non-painful bodily symptoms.
Major depressive disorder diagnosis
Major depressive disorder is a clinical diagnosis; this is mainly determined by the patient's medical history and assessment of mental status.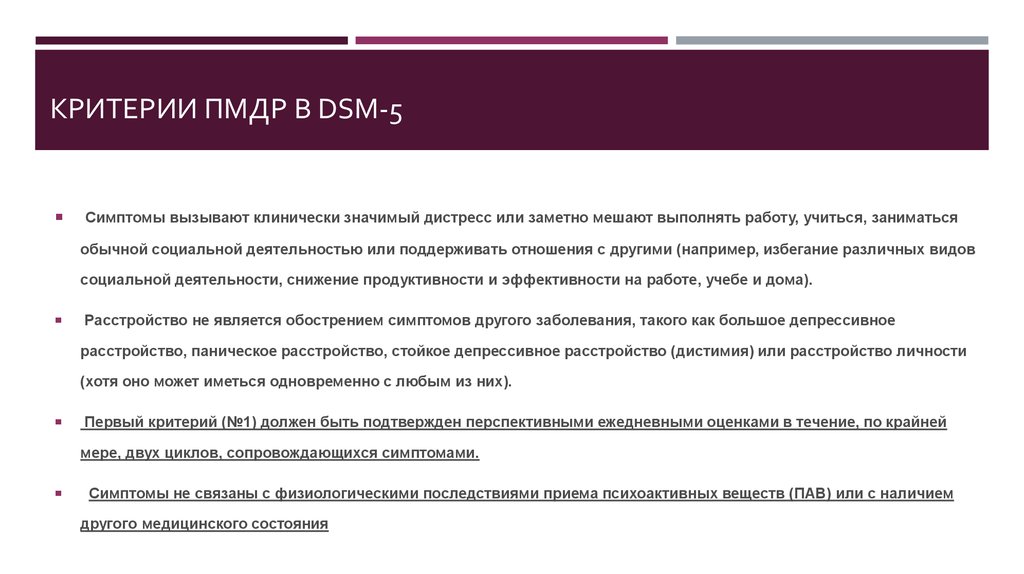 Along with symptomatology, the clinical interview should include medical history, family history, social history, and history of drug use. Related information from the patient's family/friends is an important component of the psychiatric evaluation. nine0003
Along with symptomatology, the clinical interview should include medical history, family history, social history, and history of drug use. Related information from the patient's family/friends is an important component of the psychiatric evaluation. nine0003
Although there are no objective tests to diagnose depression, routine laboratory tests such as CBC with a differential diagnosis, a comprehensive metabolic panel, thyroid-stimulating hormone, free T4, vitamin D, urinalysis, and toxicology screening are done to rule out organic or medical diseases. causes of depression.
People with depression often see their primary care physicians for medical problems related to their depression rather than seeking a mental health professional. In nearly half of the cases, patients deny experiencing depressive symptoms and are often referred to therapy by family members or sent by employers to be tested for social isolation and decreased activity. At each visit, it is critical to assess the patient for thoughts of suicide or murder. nine0003
nine0003
Being in a bad mood or feeling tense is common for all of us. When these feelings persist, you may suffer from depression or anxiety—or both. The self-assessment quizzes contain relevant questions to help you assess your current situation and develop a strategy to help you feel better sooner.
When you are going through a difficult moment, it is natural to feel depressed for a while; feelings like melancholy and loss help define who we are. However, if you feel sad or uncomfortable most of the time for an extended period of time, you may be suffering from depression. nine0003
Take a self-test to see if you are showing any warning signs of depression. This won't give you a diagnosis, but it will help you determine what to do next.
Major depressive disorder with psychotic features
Psychotic depression, also known as major depressive disorder with psychotic features, is a serious medical or mental illness that requires prompt treatment and constant monitoring by a physician or mental health professional.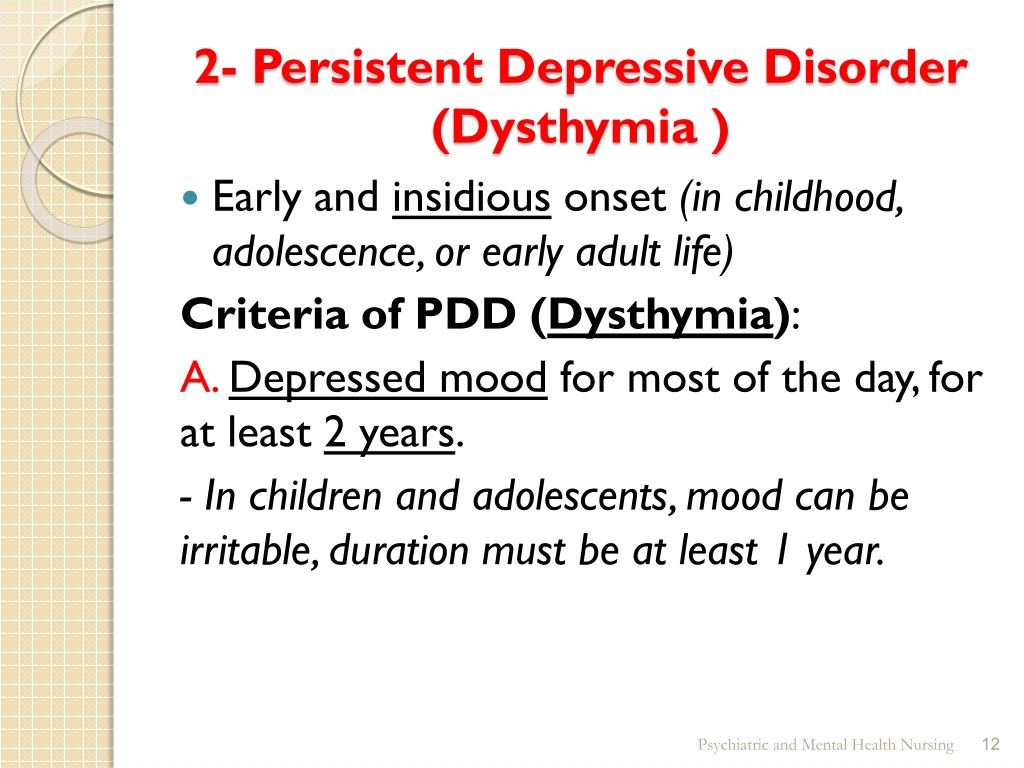 nine0003
nine0003
Major depression is a common mental condition that can have a detrimental effect on many aspects of a person's life. It affects mood and behavior as well as various bodily processes such as eating and sleeping. People who are severely depressed often lose interest in things they used to love and have difficulty doing daily activities. Sometimes they may even feel that life is not worth living.
Bipolar disorder (BD)
Depression in patients with bipolar disorder (BD) is a significant clinical problem. Since schizophrenia dominates even in the treatment of BD, depression is associated not only with schizophrenia, but also with BD and comorbid medical disorders with a high risk of suicide.
Diagnosis of bipolar disorder (BD) and risk factors:
Approximately 12-17% of cases of bipolar disorder are not recognized until the mood "transforms" into hypomania or mania, either spontaneously or under the influence of substances uplifting mood. nine0003
nine0003
Factors suggesting a diagnosis of BD:
- Family mania, psychosis, "nervous breakdown" or psychiatric hospitalization
- Early onset, often with depressive symptoms
- Cyclothymic mood
- Multiple relapses (eg 4 episodes of depression in 10 years)
- Depression with characteristic agitation, anger, insomnia, irritability, talkativeness.
- Other features are "mixed" or hypomanic or psychotic symptoms. nine0015
- Clinically "worsens", especially with mixed properties, during antidepressant treatment.
- Suicidal thoughts and actions
- Alcohol or drug abuse
Major depressive disorder in children and adolescents:
Major depressive disorder (MDD) can have a significant impact onset during childhood and adolescence. Associated with this are poor school performance, interpersonal problems later in life, early parenthood, and an increased risk of other psychiatric and substance use disorders.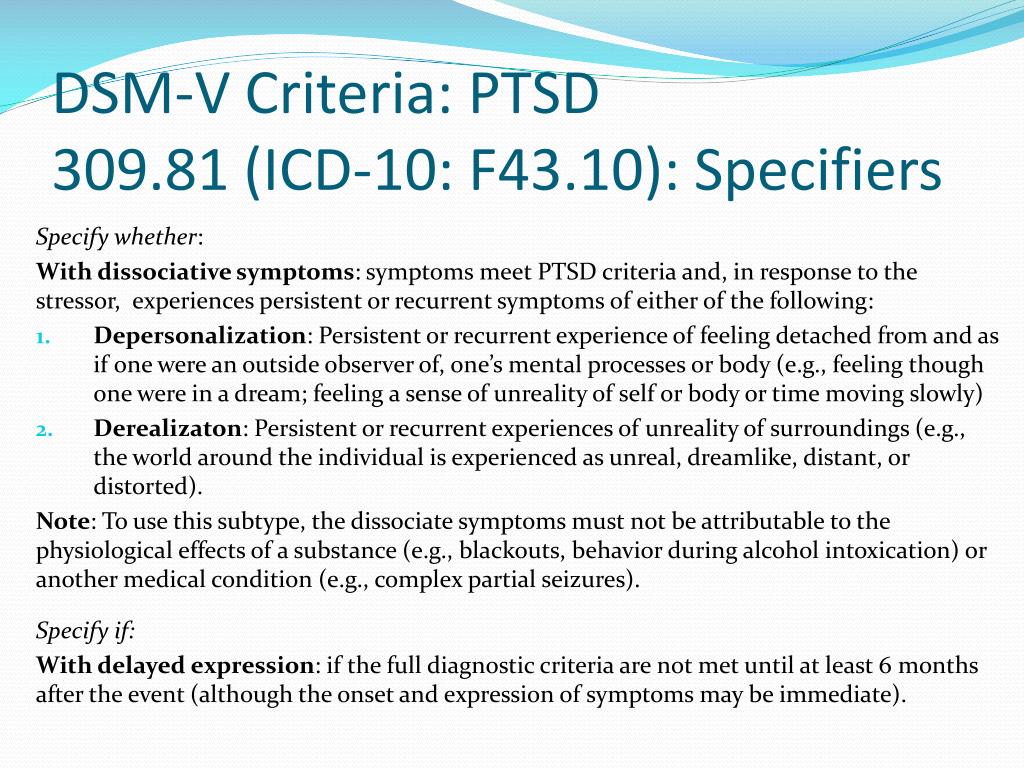 Diagnosing MDD in childhood is difficult. Children with MDD are often underdiagnosed and undertreated, and only 50% of adolescents are diagnosed before reaching adulthood. nine0003
Diagnosing MDD in childhood is difficult. Children with MDD are often underdiagnosed and undertreated, and only 50% of adolescents are diagnosed before reaching adulthood. nine0003
Symptoms of depression in children aged 3-8 years include:
- unsubstantiated claims.
- irritability
- less signs of depression
- anxiety
- behavioral changes
As the child becomes adolescence and adult, the presentation of symptoms meets the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria:
- Irritability. nine0015
- Expected weight gain.
- Lethargy or inner restlessness.
- May be delusional and not limited to feelings of guilt.
Postpartum depression
Postpartum depression affects one in seven women (PPD). While most women recover quickly from childhood blues, PPD lasts much longer and has a significant impact on women's ability to return to normal activities.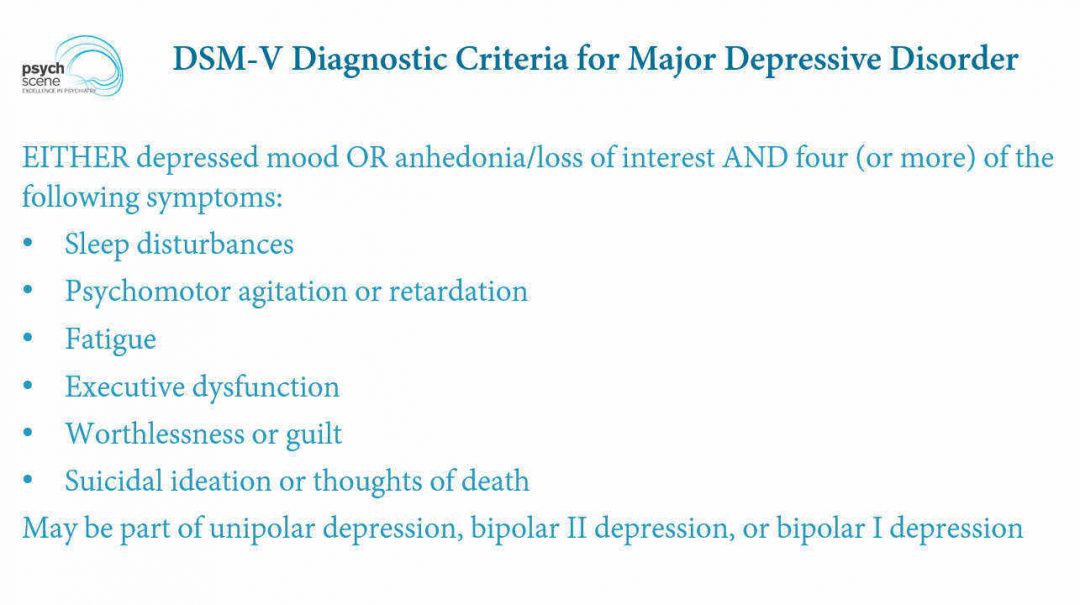 nine0003
nine0003
PDD affects the mother and her relationship with the child. PRD impairs maternal brain response and behavior. Postpartum depression most often occurs within 6 weeks after delivery. PDD affects 6.5 to 20% of women. It is more common in teenage girls, mothers who have given birth prematurely, and women living in cities.
In one study, African American and Hispanic mothers reported onset of symptoms within 2 weeks of birth, while white mothers reported onset of symptoms later. nine0003
Premenstrual dysphoric disorder
Premenstrual symptoms are a group of psychological, behavioral and physical symptoms that cyclically occur before menstruation and subsequently resolve after menstruation in women of reproductive age. Most women experience relatively mild pain and the symptoms do not interfere with their personal, social, or professional lives; however, 5% to 8% of women experience moderate or severe symptoms that can cause significant distress and functional impairment.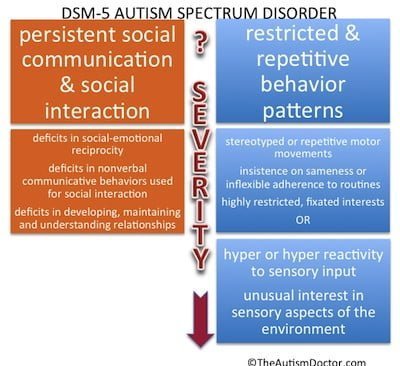 nine0003
nine0003
All women of reproductive age, from menarche to menopause, may have premenstrual symptoms. Premenstrual symptoms are a common problem for women of reproductive age. In the United States, 70 to 90 percent of women of reproductive age report at least some premenstrual pain.
Approximately one third of these women have symptoms severe enough to warrant a diagnosis of PMS. PMDD, the most severe type of premenstrual symptom complex, occurs in 3-8% of these women. nine0003
Treatment of major depressive disorder
Treatment of major depressive disorder (MDD) in adults:
Treatment options for major depressive disorder include medication, psychological, interventional and lifestyle changes. Medications and/or psychotherapy are used initially to treat MDD.
Combination treatment, including both drugs and psychotherapy, has been shown to be more effective than either treatment alone. Electroconvulsive therapy has been shown to be more effective than any other treatment for severe major depression.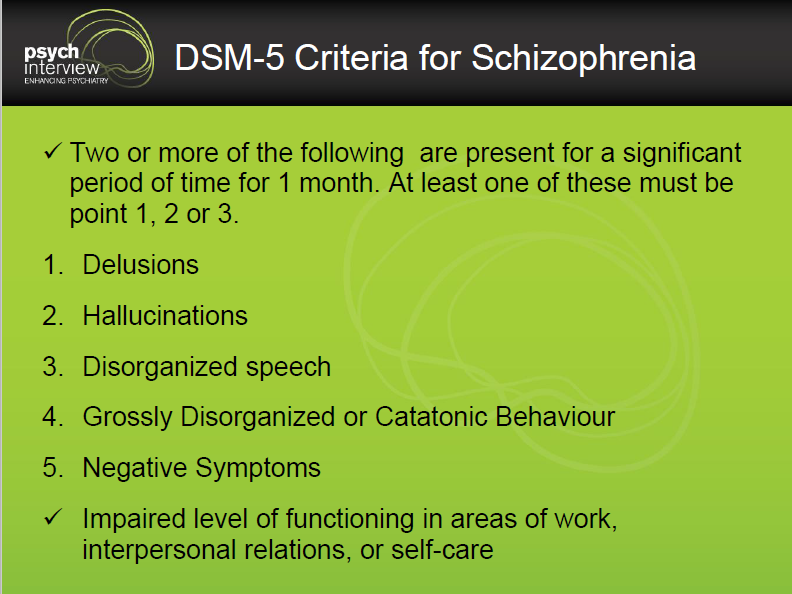 nine0003
nine0003
Patient psychotherapy:
Depression education and treatment can be provided to all patients. When appropriate, education may be provided to eligible family members.
Information about available treatment options will help patients make informed decisions, anticipate side effects, and follow prescribed treatment. Another important aspect of education was informing patients and concerned family members about the delayed duration of antidepressant onset of action. nine0003
Pharmacotherapy and acute treatment:
Antidepressants may be used as the primary treatment for patients with moderate or severe depression.
Clinical features that may indicate that the drug is a preferred therapeutic agent include a history of previous positive response to antidepressants, severity of symptoms, significant sleep disturbance and appetite disturbance.
Patients with severe depression with psychotic features will require antidepressant and antipsychotic and/or electroconvulsive therapy (ECT).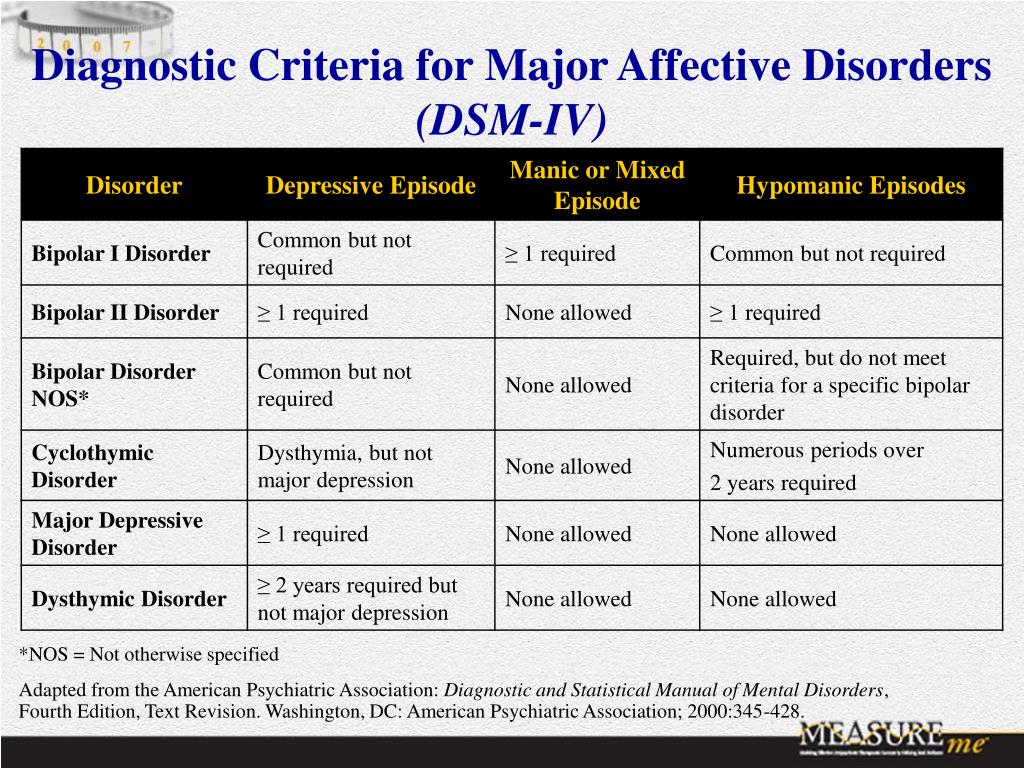 nine0003
nine0003
All antidepressants are effective, although their side effects vary. The following drugs have been approved by the FDA for the treatment of MDD:
- Fluoxetine, sertraline, citalopram, escitalopram, paroxetine, and fluvoxamine are examples of selective serotonin reuptake inhibitors (SSRIs). They are commonly used as first line therapy and are the most commonly prescribed antidepressants.
- Venlafaxine, duloxetine, desvenlafaxine, levomilnacipran and milnacipran are examples of serotonin and norepinephrine reuptake inhibitors (SNRIs). They are often used to treat depressed people who also have pain problems. nine0015
- Trazodone, vilazodone and vortioxetine are serotonin modulators.
- Bupropion and mirtazapine are examples of atypical antidepressants. When patients experience sexual side effects from SSRIs or SNRIs, they are often recommended as monotherapy or as adjunctive drugs.
- Amitriptyline, imipramine, clomipramine, doxepin, nortriptyline and desipramine are tricyclic antidepressants (TCAs).
- Tranylcypromine, phenelzine, selegiline, and isocarboxazid are examples of monoamine oxidase inhibitors (MAOIs). Due to the high prevalence of side effects and death in overdose, MAOIs and TCAs are not commonly used. nine0015
- Other drugs that can be used to increase the effectiveness of antidepressants include mood stabilizers and antipsychotics.
The role of yoga and meditation in managing depression:
Originating in ancient India, yoga is recognized as a form of alternative medicine using mind-body practice. Yoga philosophy is based on 8 elements that are best described as the ethical principles of a meaningful and purposeful life. Yoga can help with depression through the following mechanisms:
- Muscle relaxation resulting in less pain
- Creating Balanced Energy
- Decreased breathing and heart rate
- Lowering blood pressure and cortisol levels
- Increase blood flow
- Reducing stress and anxiety through tranquility
- Improve pre-existing ailments such as arthritis, cancer, mental illness and more.
Treatment of Major Depressive Disorder (MDD) in Children and Adolescents
Psychotherapy is important for both patients and their families, so everyone is aware of the plan and goals of treatment. When the patient receives information, the severity of symptoms decreases. Mental education may include knowledge about the signs and symptoms of depression, the clinical course of the illness, the risk of exacerbation, treatment options, and parental advice on how to interact with depressed young people.
According to research by Sandra Mullen, psychotherapy, along with medication, is often recommended for the treatment of major depressive disorder (MDD) in children and adolescents diagnosed with depression, suicidal ideation, and transient hypomania/mania. nine0003
Treatment of bipolar depression
Bipolar depression remains a clinical problem. Treatment options are limited, especially in the treatment of the acute phase of bipolar depression.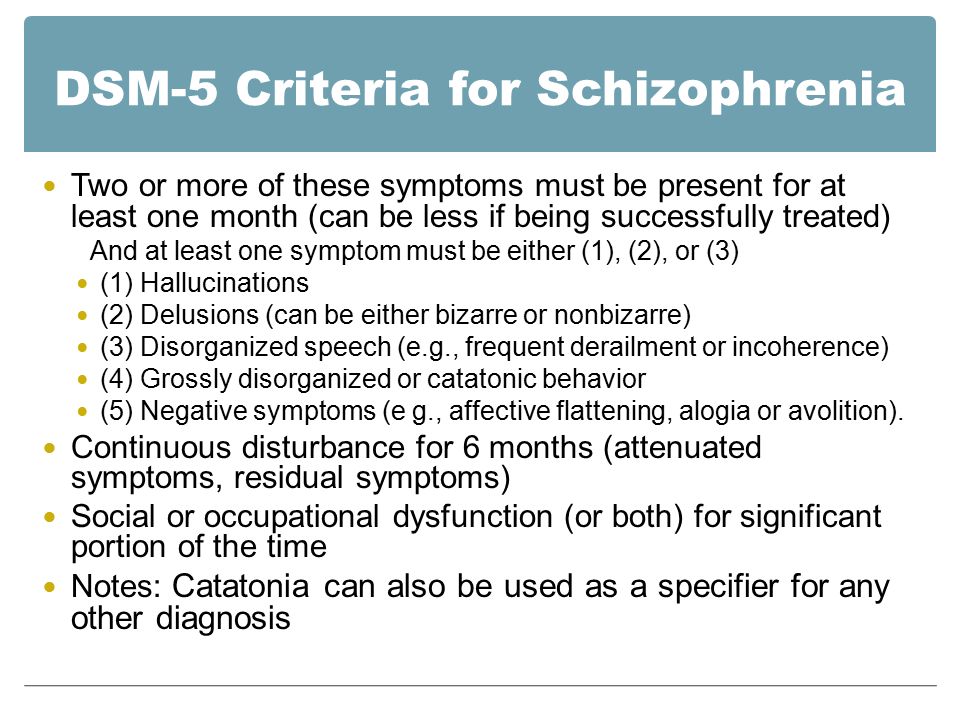 There are currently only three approved drugs: OFC, quetiapine (immediate or extended release) and lurasidone (lithium monotherapy or adjuvant therapy or valproate). All three agents have similar efficacy profiles. They differ in duration. nine0003
There are currently only three approved drugs: OFC, quetiapine (immediate or extended release) and lurasidone (lithium monotherapy or adjuvant therapy or valproate). All three agents have similar efficacy profiles. They differ in duration. nine0003
Non-approved agents and treatments
Non-pharmacological drugs such as lamotrigine, antidepressants, modafinil, pramipexole, ketamine, and electroconvulsive therapy (ECT) are often prescribed for the treatment of acute bipolar depression.
Treatment of recurrent depression:
Some patients may experience recurrent episodes of depression throughout their lives unless supportive care is used to prevent relapse. Treatment should include psychotherapy and pharmacotherapy, and the dose should generally not be reduced after remission has been achieved. nine0003
Differential
Critical to rule out depressive disorder due to another medical condition, depressive disorder due to substance/drug, dysthymia, cyclothymia, bereavement, adjustment disorder with depressed mood, bipolar disorder, schizoaffective disorder, schizophrenia, anxiety disorders and eating disorders when assessed for DMD.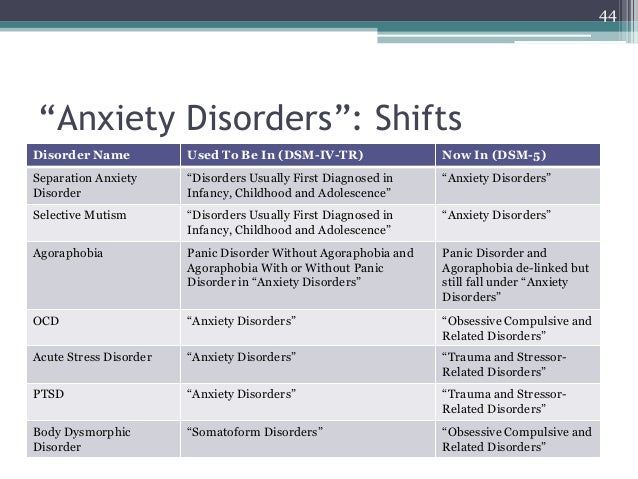 Depressive symptoms can develop as a result of the following factors:
Depressive symptoms can develop as a result of the following factors:
- Neurological causes such as cerebrovascular accident, multiple sclerosis, epilepsy, Parkinson's disease and Alzheimer's disease.
- Endocrine diseases such as diabetes, thyroid disease and adrenal disease.
- Metabolic disorders such as hypercalcemia, hyponatremia
- Drugs/substances causing dependence: steroids, antihypertensives, anticonvulsants, antibiotics, sedatives, sleeping pills, alcohol, stimulant withdrawal. nine0015
- Nutrient deficiencies such as vitamin D, B12, B6, iron or folic acid deficiency
- Infectious diseases such as HIV and syphilis
- Malignant neoplasms
Prognosis
Episodes of depression in untreated major depressive disorder may last 6 to 12 months. Approximately two-thirds of people with MDD think about suicide, and 10 to 15% commit suicide. MDD is a chronic relapsing disease; the recurrence rate after the first episode is about 50%, 70% after the second episode and 90% after the third episode.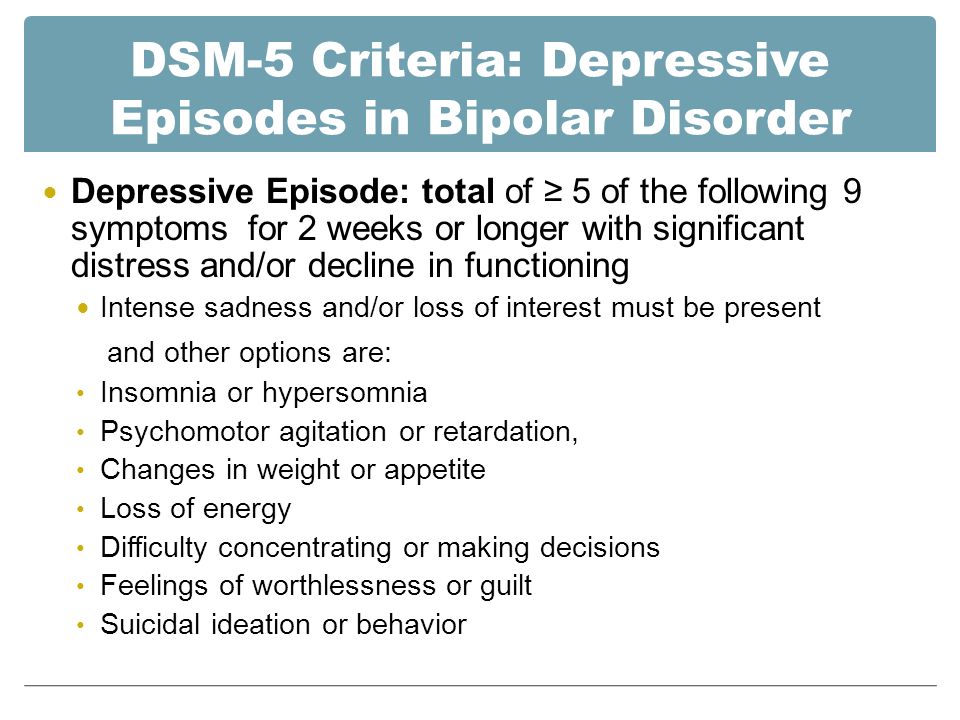 Approximately 5-10% of people with MDD develop bipolar disorder.
Approximately 5-10% of people with MDD develop bipolar disorder.
Patients with mild episodes, no psychotic symptoms, improved adherence, a reliable support system, and adequate premorbid functioning have a positive prognosis for MDD. In the presence of a concomitant mental disorder, personality disorder, multiple hospitalizations and advanced age, the prognosis is poor.
Complications
MDD is one of the leading causes of disability in the world. This not only causes severe functional impairment, but also negatively affects interpersonal relationships, reducing the quality of life. Individuals with MDD are at significant risk of developing comorbid anxiety and drug use disorders, which increase the risk of suicide.
Diabetes, hypertension, chronic obstructive pulmonary disease and coronary heart disease may be aggravated by depression. People who are depressed are more likely to engage in self-destructive behavior as a coping method. Left untreated, MDD can be quite debilitating.