Cognitive behavioral therapy for agoraphobia
Treatment - Agoraphobia - NHS
A stepped approach is usually recommended for treating agoraphobia and any underlying panic disorder.
The steps are as follows:
- Find out more about your condition, the lifestyle changes you can make, and self-help techniques to help relieve symptoms.
- Enrol yourself on a guided self-help programme.
- Undertake more intensive treatments, such as cognitive behavioural therapy (CBT), or see if your symptoms can be controlled using medicine.
Self-help techniques and lifestyle changes
Learning more about agoraphobia and its association with panic disorder and panic attacks may help you control your symptoms better.
For example, there are techniques you can use during a panic attack to bring your emotions under control.
Having more confidence in controlling your emotions may make you more confident coping with previously uncomfortable situations and environments.
- Stay where you are – try to resist the urge to run to a place of safety during a panic attack; if you're driving, pull over and park where it's safe to do so.
- Focus – it's important for you to focus on something non-threatening and visible, such as the time passing on your watch, or items in a supermarket; remind yourself the frightening thoughts and sensations are a sign of panic and will eventually pass.
- Breathe slowly and deeply – feelings of panic and anxiety can get worse if you breathe too quickly; try to focus on slow, deep breathing while counting slowly to 3 on each breath in and out.
- Challenge your fear – try to work out what it is you fear and challenge it; you can achieve this by constantly reminding yourself that what you fear is not real and will pass.
- Creative visualisation – during a panic attack, try to resist the urge to think negative thoughts, such as "disaster"; instead, think of a place or situation that makes you feel peaceful, relaxed or at ease: once you have this image in your mind, try to focus your attention on it.
- Do not fight an attack – trying to fight the symptoms of a panic attack can often make things worse; instead, reassure yourself by accepting that although it may seem embarrassing and your symptoms may be difficult to deal with, the attack is not life threatening.
Making some lifestyle changes can also help. For example, ensure you:
- take regular exercise – exercise can help relieve stress and tension and improve your mood
- have a healthy diet – a healthy, balanced diet and weight can help maintain overall health
- avoid using drugs and alcohol – they may provide short-term relief, but in the long term they can make symptoms worse
- avoid drinks containing caffeine, such as tea, coffee or cola – caffeine has a stimulant effect and can make your symptoms worse
Talking therapies
If your symptoms do not respond to self-help techniques and lifestyle changes, your GP may suggest trying a talking therapy.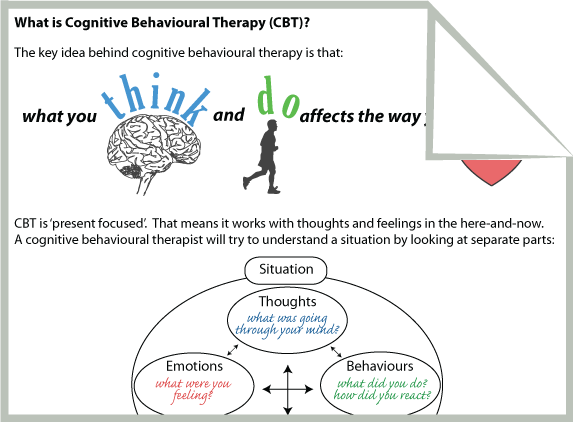
If you prefer, you can refer yourself directly for talking therapies, such as cognitive behavioural therapy (CBT), without seeing your GP.
Find an NHS talking therapies service
Read more about talking therapies on the NHS.
Guided self-help
With guided self-help you work through a CBT-based workbook or computer course with the support of a therapist.
The therapist works with you to understand your problems and make positive changes in your life.
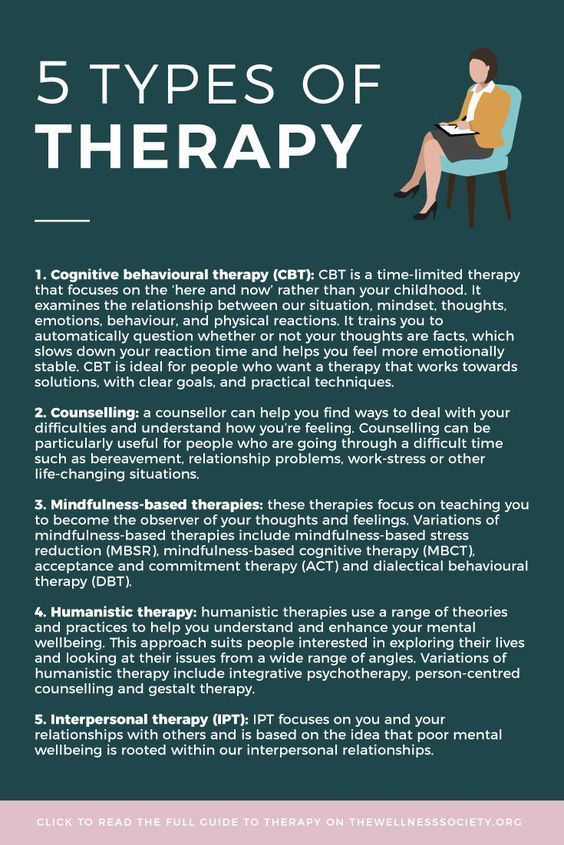
Cognitive behavioural therapy (CBT)
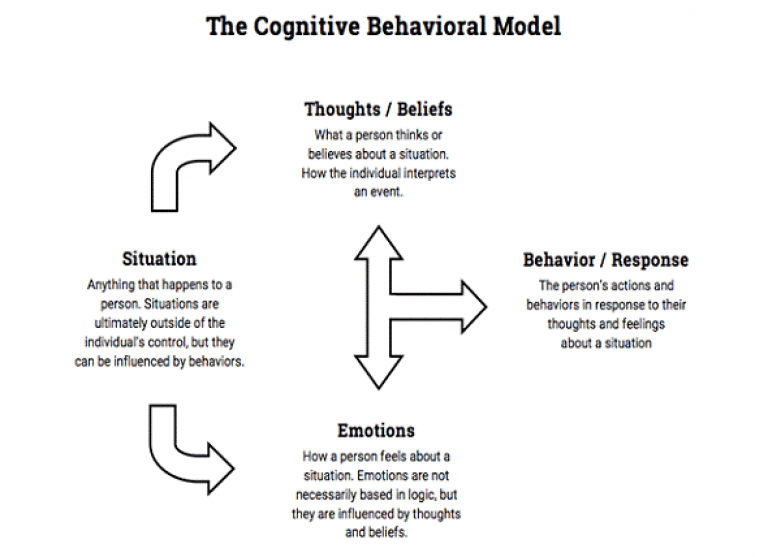
Cognitive behavioural therapy (CBT) is based on the idea that unhelpful and unrealistic thinking leads to negative behaviour.
CBT aims to break this cycle and find new ways of thinking that can help you behave more positively. For example, many people with agoraphobia have the unrealistic thought that if they have a panic attack it will kill them.
The CBT therapist will try to encourage a more positive way of thinking – for example, although having a panic attack may be unpleasant, it is not fatal and will pass.
This shift in thinking can lead to more positive behaviour in terms of a person being more willing to confront situations that previously scared them.
CBT is usually combined with exposure therapy. Your therapist will set relatively modest goals at the start of treatment, such as going to your local corner shop.
As you become more confident, more challenging goals can be set, such as going to a large supermarket or having a meal in a busy restaurant.
A course of CBT usually consists of 12 to 15 weekly sessions, with each session lasting about an hour.
Video: talking therapies for stress, anxiety and depression
Animated video explaining self-referral to talking therapies services for stress, anxiety or depression.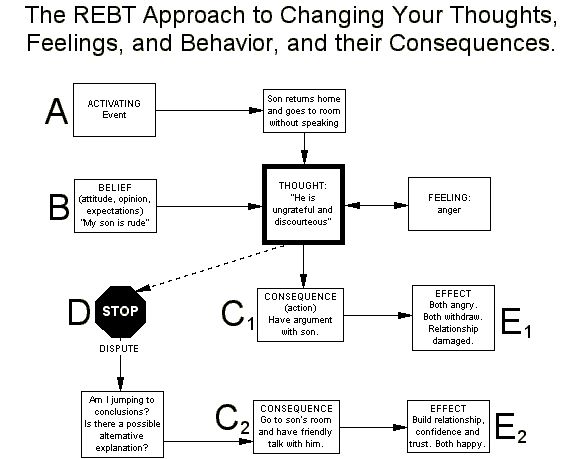
Media last reviewed: 14 March 2022
Media review due: 14 March 2025
Applied relaxation
Applied relaxation is based on the premise that people with agoraphobia and related panic disorder have lost their ability to relax. The aim of applied relaxation is therefore to teach you how to relax.
This is achieved using a series of exercises designed to teach you how to:
- spot the signs and feelings of tension
- relax your muscles to relieve tension
- use these techniques in stressful or everyday situations to prevent you feeling tense and panicky
As with CBT, a course of applied relaxation therapy consists of 12 to 15 weekly sessions, with each session lasting about an hour.
Medicine
Sometimes medicine can be used as a sole treatment for agoraphobia. In more severe cases, it can also be used in combination with CBT or applied relaxation therapy.
In more severe cases, it can also be used in combination with CBT or applied relaxation therapy.
Selective serotonin reuptake inhibitors (SSRIs)
If medicine is recommended for you, you'll usually be prescribed a course of selective serotonin reuptake inhibitors (SSRIs).
SSRIs were originally developed to treat depression, but they've also proved effective for helping treat other mood disorders, such as anxiety, feelings of panic, and obsessional thoughts.
An SSRI called sertraline is usually recommended for people with agoraphobia. Side effects associated with sertraline include:
- feeling sick
- loss of sex drive (libido)
- blurred vision
- diarrhoea or constipation
- feeling agitated or shaky
- excessive sweating
These side effects should improve over time, although some can occasionally persist.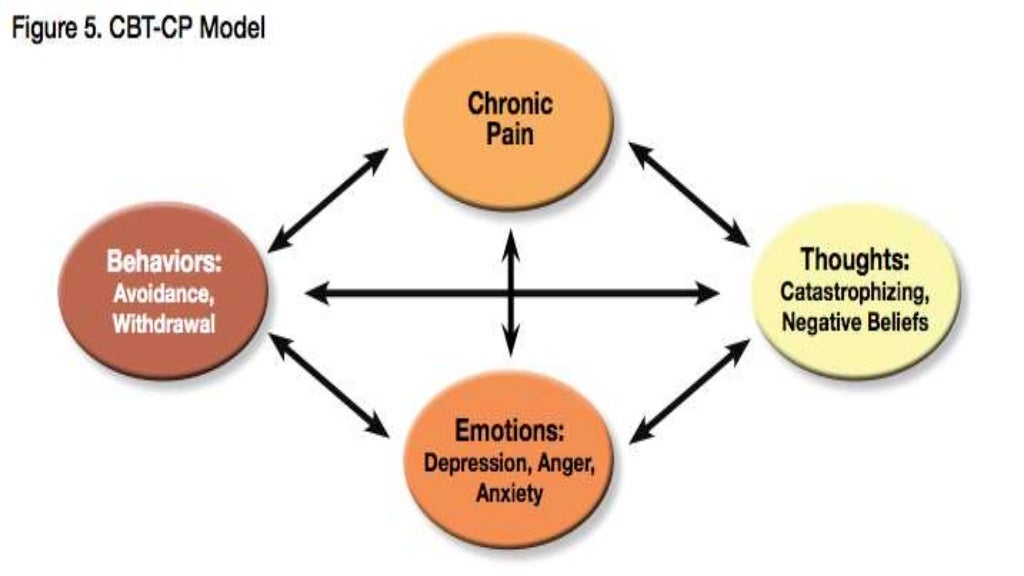
If sertraline fails to improve your symptoms, you may be prescribed an alternative SSRI or a similar type of medicine known as serotonin-norepinephrine reuptake inhibitors (SNRIs).
The length of time you'll have to take an SSRI or SNRI for will vary depending on your response to treatment. Some people may have to take SSRIs for 6 to 12 months or more.
When you and your GP decide it's appropriate for you to stop taking SSRIs, you'll be weaned off them by slowly reducing your dosage. You should never stop taking your medicine unless your GP specifically advises you to.
Pregabalin
If you're unable to take SSRIs or SNRIs for medical reasons or you experience troublesome side effects, another medicine called pregabalin may be recommended. Dizziness and drowsiness are common side effects of pregabalin.
Read more about pregabalin.
Support groups
Charities like Mind and Anxiety Care UK are useful resources for information and advice about how to manage anxiety and phobias. They can also put you in touch with other people who've had similar experiences.
Agoraphobia - CBT Psychology
Have you been afraid to leave your home because of worries that you would panic, everyone would notice, and you wouldn’t be able to escape? For people with agoraphobia, this is a regular struggle. While it makes them feel safe, it is a lonely and restrictive way to live. This disorder literally traps people inside.
What is Agoraphobia?People with Agoraphobia have an extreme and unrealistic fear of difficult or embarrassing situations they cannot escape or get help. In these situations, they are worried about developing panic-like symptoms, such as feeling trapped, scared, anxious, or helpless.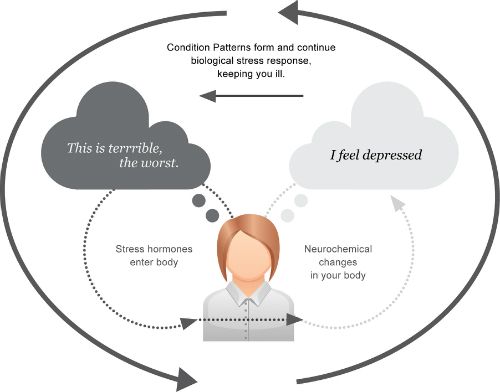 As a result, people with agoraphobia often avoid these situations. This can make life very lonely and restricting. For example, someone with agoraphobia may stop visiting their friends, travel, or go to the store. In addition, a person with agoraphobia may rely on family members to run errands for them and accompany them outside which can have a negative effect on relationships. Eventually, the fear may become so severe that the individual may confine themselves to their neighbourhood or home for most of the day.
As a result, people with agoraphobia often avoid these situations. This can make life very lonely and restricting. For example, someone with agoraphobia may stop visiting their friends, travel, or go to the store. In addition, a person with agoraphobia may rely on family members to run errands for them and accompany them outside which can have a negative effect on relationships. Eventually, the fear may become so severe that the individual may confine themselves to their neighbourhood or home for most of the day.
Someone with agoraphobia has likely experienced at least one panic attack in their lives. These symptoms of panic sometimes occur in other anxiety disorders. It is these attacks that a person with agoraphobia fears will happen in certain situations. The symptoms include:
- Shortness of breath
- Racing heart
- Sweating or hot flashes
- Chest pain
- Dizziness
- Nausea
- Chills or trembling
- Numbness
- Feelings of unreality
Consequently, agoraphobia can lead an individual to fear and avoid specific situations, like:
- Using public transportation (for example, riding a bus or traveling on an airplane)
- Being in open spaces (for instance, parks or shopping malls)
- Enclosed spaces (such as elevators, cars, or movie theatres)
- Spaces where there are crowds
- Standing in lines
- Any spaces where escape may be difficult
- ….
 Eventually, being anywhere outside the home (especially alone) for a long time
Eventually, being anywhere outside the home (especially alone) for a long time
In these situations, the panic or anxiety response is triggered. However, this stress or discomfort is usually out of proportion to the actual level of danger in the situation. Importantly, someone with agoraphobia may feel helpless or dependent on others.
Why do People Develop Agoraphobia?Like most anxiety disorders, the exact cause of agoraphobia is not known. Rather, there are many factors that can make someone more at risk of developing the disorder. For instance, someone with another condition such as social anxiety disorder, generalized anxiety disorder, depression, or another phobia may be more likely to develop agoraphobia than the general population. Someone with a family history of agoraphobia may also be more at risk. For example, someone who has a history of trauma or recently experienced a death may be more prone to developing this condition. Agoraphobia typically develops in young adulthood, and it’s more common among women.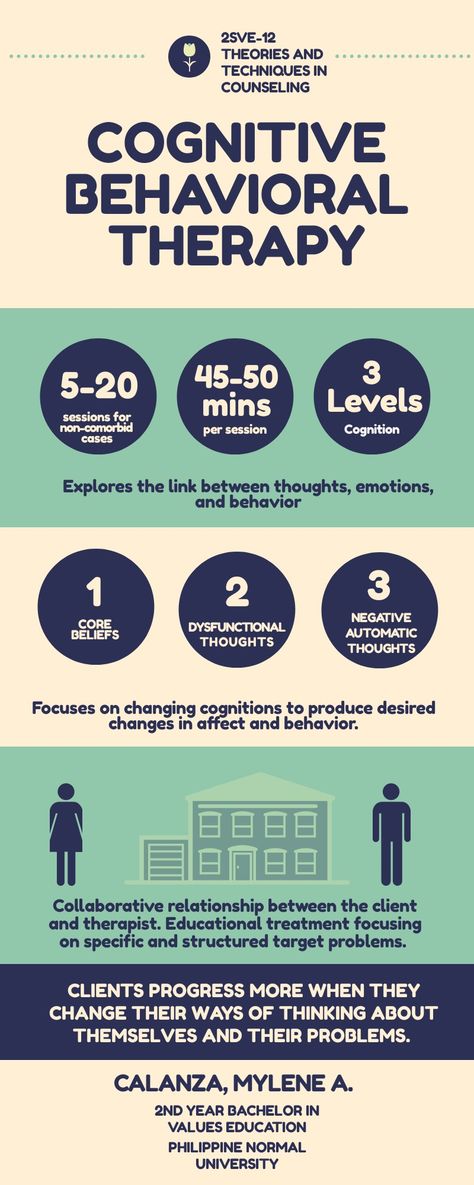
People struggling with agoraphobia can implement some lifestyle changes to better manage their symptoms. These changes include practicing relaxation techniques to reduce anxiety, eating a healthy diet, getting regular exercise and sleep, and limiting drug and alcohol intake, including caffeine. However, lifestyle changes alone are often not enough to treat agoraphobia.
Cognitive Behavioural Therapy is the most practical and effective treatment for agoraphobia and has a low relapse rate. This therapy is short term, typically 8 to 12 weeks. A CBT therapist provides psychoeducation to help the client understand their distorted beliefs and feelings. In addition, the therapist teaches the client skills to manage stressful situations by replacing negative thoughts with more realistic ones, while also learning relaxation and breathing techniques to better cope with their anxiety. Part of CBT therapy is the “homework” clients complete between sessions to further their therapy.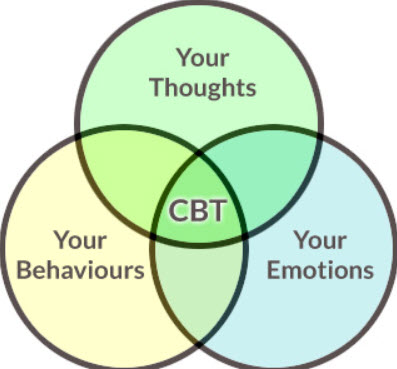
A CBT therapist will incorporate elements of exposure therapy, to help the client slowly expose themselves to situations they fear. This type of exposure can help the fears reduce over time, as clients come to realize their feared outcomes do not really happen the way they feared and they can start to change their avoidance and replace it with taking small steps toward their goal. The power of CBT for Agoraphobia is that clients can re-gain control over their lives.
If you want help to break free of this daily struggle, a psychologist can help you using evidence-based treatments.If you are interested in therapy for Agoraphobia and reside in Ontario, you can reach our intake coordinators at 905.597.4404 or fill out the form below and you will be contacted within 24 business hours. Teletherapy is available for sessions over the phone or a video call to help you move forward with your life.
Panic attacks, panic disorder and agoraphobia
Life is sometimes unpredictable. Therefore, it will most likely be difficult to say with complete certainty that you can spend your whole life being in complete peace and not having anxiety. Anxiety from time to time is normal. But there are times when a person begins to worry too much or often. Anxiety spectrum disorders are different. Panic attacks are one of the possible manifestations of anxiety. According to 2017 data, anxiety spectrum disorders are the most common among mental disorders [1]. nine70 million people in the world have mental illness, 3.76% of them have an anxiety spectrum disorder [2]. Often people seek help from specialists in somatic profiles, thinking that they have physical health problems.
Therefore, it will most likely be difficult to say with complete certainty that you can spend your whole life being in complete peace and not having anxiety. Anxiety from time to time is normal. But there are times when a person begins to worry too much or often. Anxiety spectrum disorders are different. Panic attacks are one of the possible manifestations of anxiety. According to 2017 data, anxiety spectrum disorders are the most common among mental disorders [1]. nine70 million people in the world have mental illness, 3.76% of them have an anxiety spectrum disorder [2]. Often people seek help from specialists in somatic profiles, thinking that they have physical health problems.
In the protocols for the treatment of panic attacks, there are several treatment options that can also be combined with each other [3,4]. Drug therapy may consist of antidepressants, anti-anxiety drugs, or beta-blockers. The selection of drug therapy is carried out by a psychiatrist. The first choice psychotherapy is cognitive behavioral therapy [5]. nine0003
nine0003
What are panic attacks, panic disorder and agoraphobia?
A panic attack is a sudden and well-defined episode of discomfort and/or intense fear, accompanied by various physical symptoms, and occurs within a maximum of ten minutes. Panic attacks are isolated cases, while panic disorder is at least two unexpected attacks of panic attacks within a certain period. Panic attacks and/or panic disorder may be accompanied by agoraphobia. Since the attack itself is accompanied by the most unpleasant feelings, at the time of a panic attack it is almost impossible to shift your attention from internal sensations to something else. Since usually people do not feel similar symptoms during their life, they cannot understand what is happening to them. nine0003
Therefore, this can be assessed as the approach of a possible catastrophe and accompanied by thoughts of a stroke / heart attack, death or going insane. When the symptoms that are described appear, the first thing everyone thinks about is problems with somatic health. Only after going through a series of doctors and eliminating somatic problems do people get to a mental health specialist. Panic attacks are situational and unpredictable, nocturnal or even "mini". An interesting fact is that about 30% of people during their lifetime have panic attacks, but only 2.7% develop panic disorder [6]. nine0003
Only after going through a series of doctors and eliminating somatic problems do people get to a mental health specialist. Panic attacks are situational and unpredictable, nocturnal or even "mini". An interesting fact is that about 30% of people during their lifetime have panic attacks, but only 2.7% develop panic disorder [6]. nine0003
Agoraphobia has several definitions. A more common definition is that agoraphobia is the fear of open spaces and crowds. Another, more specific, definition of agoraphobia is anxiety due to being in places or situations in which it might be difficult to get out if a person suddenly becomes ill.
What are the symptoms of a panic attack, agoraphobia and panic disorder?
Panic attack symptoms
- Sensation of reinforced or rapid heartbeat
- trembling or chill
- The feeling of breathing or suffocation
- Slicks
- Fear of suffocation
- pain or discomfort in the chest
- Trip
- Distribution, sensation of disgrace lose control or go crazy
- Paresthesias
- Flushes of cold or heat
- Fear of dying
Symptoms of panic disorder
- At least two unexpected attacks of panic attacks
- At least one month after one of the attacks at least one of the following criteria:
- Anxiety due to a possible repetition
- about the negative consequences of the attack
- Marked behavioral changes associated with the experience of the attack
- Panic attacks not caused by a medical illness or psychoactive substances
- Panic attacks are independent of the context of another anxiety disorder
Agoraphobia symptoms or panic-like symptoms) help may not be available
What are the treatments for panic attacks, panic disorder and agoraphobia?
There are several approaches to the treatment of panic attacks, panic disorder and agoraphobia.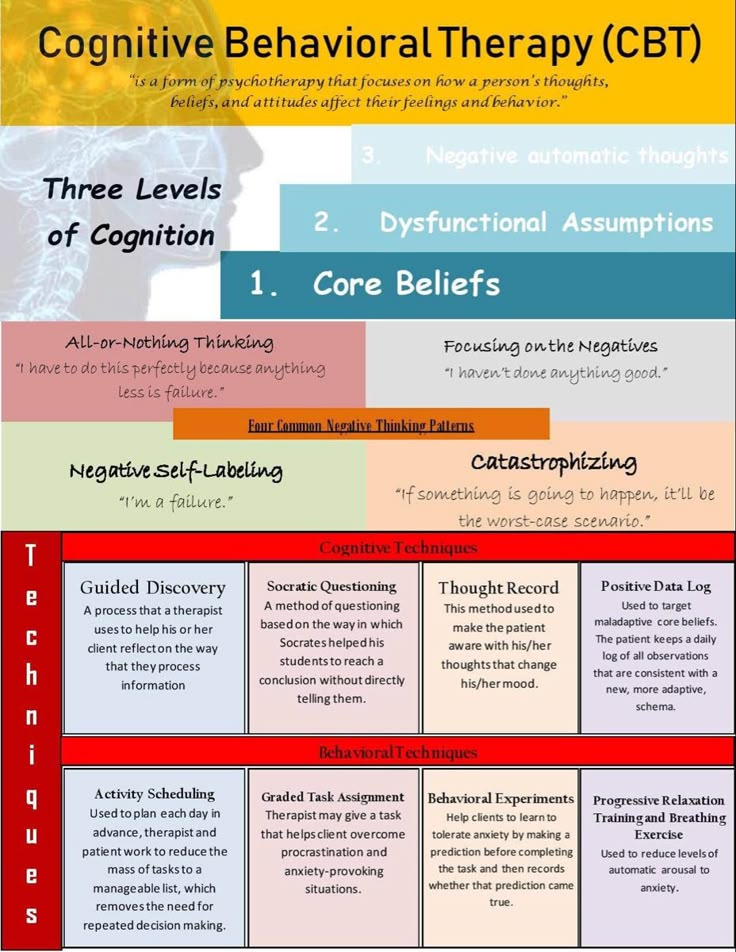
The first option is treatment that is prescribed by a psychiatrist. The most common drugs prescribed for these conditions are antidepressants of certain groups. They reduce the severity of symptoms of anxiety and panic, and the overall number of panic attacks. nine0003
But do not forget that panic attacks, panic disorder and agoraphobia also have psychological components, which cognitive-behavioral therapy can perfectly cope with [7,8,9].
How does CBT work?
Since, during panic attacks, there are certain features of how a person feels and how a person thinks about his condition at that moment, an algorithm of actions for panic attacks, panic disorder and agoraphobia was developed. nine0003
- Correction of the meanings given to the symptoms - at this stage, an opinion / belief is detected and changed (often it is something like “I am dying, I have a heart attack, a stroke”). These beliefs are found, evaluated, tested and changed. And it's quite real ☺
- Overcoming avoidance - at this stage, a person again begins to meet with what he avoided, already having the tools to cope and knowledge of his condition.
- Work with anxiety - here is a general work with anxiety and worries, because often it is simply necessary to further maintain the result. nine0030
- Restoration of activity - a person returns to the previous rhythm of life, or builds a new rhythm in which he is comfortable.
- Relapse Prevention - Reinforcing Therapy
Those who have panic attacks, panic disorder and/or agoraphobia know how frustrating and painful it can be. Life changes under the influence of factors over which people have no influence. A feeling of fatigue and hopelessness can take over if left untreated. nine0003
Don't lose hope, though. For many years now, cognitive behavioral therapy, and if necessary, drug treatment, has been adept at meeting these challenges.
Links:
- https://ourworldindata.org/mental-health
- https://doi.org/10.1002/da.22572
- https://www.nimh.nih.gov/health/topics /anxiety-disorders/index.shtml
- https://www.
 nice.org.uk/guidance/qs53
nice.org.uk/guidance/qs53 - https://doi.org/10.1002/da.22572
- https://pubmed.ncbi.nlm.nih.gov/30199184/
- Westen D, Morrison K. A multidimensional meta-analysis of treatments for depression, panic, and generalized anxiety disorder: an empirical examination of the status of empirically supported therapies. J Consult Clin Psychol . 2001;69:875–99.
- Gould RA, Otto MW, Pollack MH. A meta-analysis of treatment outcome for panic disorder. Clin Psychol Rev. . 1995;15:819–44.
- Clum GA, Clum GA, Surls R. A meta-analysis of treatments for panic disorder. nine0134 J Consult Clin Psychol . 1993;61:317–26.–x
Psychotherapy in the treatment of panic disorder with or without agoraphobia
Why is this review important?
Many people suffer from panic disorders. Panic disorder can occur alone or in combination with agoraphobia. People with panic disorder have occasional panic attacks. During a panic attack, people experience a sudden feeling of intense fear, accompanied by the following symptoms: palpitations, chest pain, sweating, shaking, dizziness, redness, upset stomach, weakness/fainting, and shortness of breath. People with agoraphobia have a strong fear of developing a panic attack in situations where exit is difficult or uncomfortable. This fear causes them to avoid such situations. nine0003
People with agoraphobia have a strong fear of developing a panic attack in situations where exit is difficult or uncomfortable. This fear causes them to avoid such situations. nine0003
There are many types of talking therapy ["talking cure"] that are used to treat panic disorder with or without agoraphobia. However, it is not clear whether any particular type of talking therapy is more effective than others in treating panic disorder with or without agoraphobia. In this review, we compared the effectiveness of different types of talking therapy.
Who will be interested in this review?
People with panic disorder with or without agoraphobia. nine0003
Friends and relatives of people with panic disorder with or without agoraphobia.
General practitioners, psychiatrists and psychologists.
Adult psychiatrists.
What questions does this review answer?
Are the included psychotherapies more effective and better tolerated than others in rapidly reducing panic disorder/agoraphobia symptoms?
Can any of the included psychotherapies guarantee better results one year after completion? nine0003
What studies were included in this review?
We searched medical databases up to 16 March 2015 for all studies (randomized controlled trials) of talking therapy for panic disorder with or without agoraphobia. To be included in this review, studies had to include people with an established diagnosis of panic disorder with or without agoraphobia.
To be included in this review, studies had to include people with an established diagnosis of panic disorder with or without agoraphobia.
We included 60 studies in this review. Of the included studies, 54 (with 3021 participants) were used for quantitative analysis. The review authors rated the quality of the studies as generally low to very low. nine0003
What does the evidence from this review say?
Review results show that talk therapy is generally more effective than no treatment. There was insufficient evidence to support any one type of talking therapy versus others for the treatment of panic disorder with or without agoraphobia in adults. However, there was some low-quality evidence in favor of cognitive behavioral therapy (CBT), psychodynamic therapy, and supportive psychotherapy, compared with other types of talking therapy, in terms of short-term remission and short-term symptom reduction. However, results regarding supportive psychotherapy should be treated with caution, as there is insufficient evidence for this type of treatment. On the other hand, in addition to evidence of efficacy, psychodynamic therapy has also shown promising results in terms of tolerability: to assess how well people tolerated talking therapy, we assessed the dropout rate of participants from studies in the short term. We found that psychodynamic therapy and the third wave of CBT had fewer dropouts, suggesting that people tolerate these treatments better than others. nine0003
On the other hand, in addition to evidence of efficacy, psychodynamic therapy has also shown promising results in terms of tolerability: to assess how well people tolerated talking therapy, we assessed the dropout rate of participants from studies in the short term. We found that psychodynamic therapy and the third wave of CBT had fewer dropouts, suggesting that people tolerate these treatments better than others. nine0003
What should be done next?
Further high quality studies are needed to fully compare the effectiveness of different types of talking therapy. In particular, more new research is needed that compares certain types of talking therapy, CBT, psychodynamic therapy, and supportive psychotherapy in the treatment of panic disorder with or without agoraphobia.
Translation notes:
Translation: Mikhail Evgenievich Kukushkin. Editing: Yudina Ekaterina Viktorovna. Project coordination for translation into Russian: Cochrane Russia - Cochrane Russia (branch of the Northern Cochrane Center on the basis of Kazan Federal University).