Bipolar job hopping
Bipolar Disorder & Job Insecurity
Post Views: 50,952
Views
Those of us with bipolar, we want to work. But both mania and depression threaten our employment. We know we are particularly vulnerable to job insecurity.
For every working person with bipolar disorder, job insecurity is a constant concern. The question is, “Will my bipolar symptoms cause me to lose my job.”
My experience is that we want to work. We want independence and the ability to support ourselves and our families. We want the satisfaction that work provides, and we want the respect that comes with having a living wage job.
We are vulnerable though. Even on the best medications, our bipolar disorder brings with it ups and downs. During the ups we take risks that aren’t necessarily good for our employers. We may be flippant and overly confident.
When we are depressed, our energy is sapped from us. Anxiety and the realization that we are not doing our job as well as we should make us feel vulnerable. We try and try to do our best, but at times our illness holds us back. In depression, no amount of cheerleading, self-help books, or inspirational sticky notes on our bathroom mirror can overcome the power of the illness.
Both mania and depression threaten our employment. When this happens we know we are vulnerable to job loss. For too many of us, this vulnerability comes to fruition by being let go, laid off, or downsized. Whatever the terminology, the result is the same.
When this happens we search for work as best we can. However, the impact on our lives of being unemployed creates self-doubt and strains our relationships. Husbands, wives, fathers and mothers, we struggle with the reality of a changing lifestyle.
So much of our self-worth is connected to working and supporting our families and ourselves. For many of us, our depression makes it incredibly challenging to get another job. We can’t project self-confidence.
At interviews we are flat. No matter how good our resume, inside we believe we don’t deserve the job, and if we get the job, we know we can’t perform at the level necessary to be successful.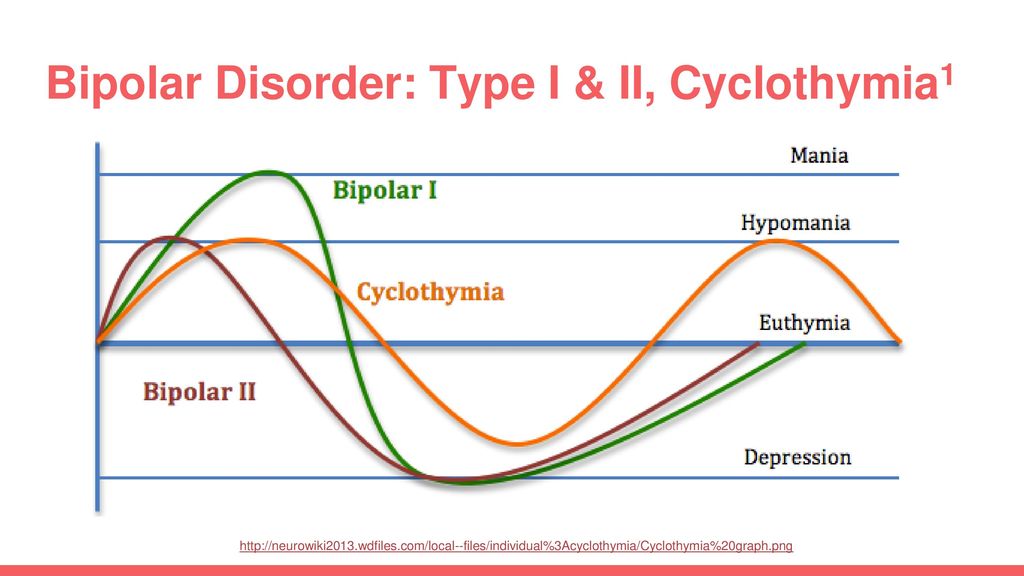 We believe that if we get the job, inevitably we will get let go again.
We believe that if we get the job, inevitably we will get let go again.
Too often people we love leave us. Our depression deepens. Our identity as a husband or wife, mother or father is shattered. We are lost and drifting. We lose our home. Friends disappear. We end up alone with our loss and the failure we feel.
How can we avoid this reality? Instead of suffering in silence, we have to talk about it with the people we love and with our therapist or family doctor. Expressing our fears helps us face them. Sharing the burden makes it more bearable.
I have lost many jobs due to my illness for both actions I took while manic and the inaction of depression. With the strength and support of my wife, counseling and medications, we have been able to rebuild our lives.
Today I know I can’t work full time so I work part-time. I know too much stress triggers anxiety and depression so I do low stress work. I have adjusted my lifestyle to this reality. This adjustment was very difficult and it took years to be ok with the changes.
This adjustment was very difficult and it took years to be ok with the changes.
As people with bipolar disorder, we have an inner strength that comes from living with so many challenges. Because of this inner strength we persevere.
Job insecurity is part of our world. It is a burden we carry. But we don’t have to carry this burden alone. Share it here, as a comment for others to read. This will reduce the burden and help people in our bphope community know they are not alone. Share your story and make a difference.
hope, work
About the author
Related
When Bipolar Disorder Makes You Change Jobs
I sit here, staring at a computer screen, without anything to do, at the job that has caused me so much turmoil this year.
This is job number 12 since I was diagnosed with bipolar disorder, six years ago. Oh, and I am on my way out. I don’t leave jobs because I can’t do my job, and I most definitely do not get fired from jobs. In fact, at this job I am considered “highly effective,” and yet I have an interview for illustrious job number 13 tomorrow. I leave because I move too quickly, work too fast and then have too much time to let everything else get in my head. This is where my disorder comes in. I start creating stories in my mind, thinking people are out to get me or they imply things that are not intended.
In fact, at this job I am considered “highly effective,” and yet I have an interview for illustrious job number 13 tomorrow. I leave because I move too quickly, work too fast and then have too much time to let everything else get in my head. This is where my disorder comes in. I start creating stories in my mind, thinking people are out to get me or they imply things that are not intended.
I have done this at every job since I was diagnosed. I impress in the interview, get the job, work harder and smarter than half of the staff, and then start the vicious cycle of finding something to focus on that will eventually cause my demise. I begin looking again and start the process all over again.
The thing is, I work hard. Really, really hard. I have gone into offices with no systems in place and have left them organized and clean. I have worked my way up from seasonal help to a supervisor. I am given special side projects. I am genuinely liked by those who hire me and they are sad to see me go. I know all of this, but my illness self-sabotages every time. If I am not creating things for my mind to believe, I am missing work because of an episode.
I know all of this, but my illness self-sabotages every time. If I am not creating things for my mind to believe, I am missing work because of an episode.
Because of my bipolar disorder, absences are an issue. No matter how efficient I am at work when I am there, missing a full day, or two, or three looks bad. I get it; when co-workers miss several days, I feel judgy myself. The thing is, these absences are legitimate sick days for my disorder; however, I have most likely not explained this to my boss for fear of repercussions. So, I miss work, use up every last minute of my sick time and sometimes leave without pay, acquire a pile of doctor’s notes, and I work hard to make up for it.
Oh, and let’s not forget work relationships. Work relationships are quite a challenge. I have often set the bar for working very high. I generally keep people at a distance because of my illness. If by chance, I do get close to someone, I will most likely share too much about myself, which will lead me into disclosing “sensitive information” about my disorder. These things could later be used against me. This happened at my current job. I was not doing well, in a depressive episode, and I got tired of questions and comments so I told someone. That one turned in to two, then three, then my entire office, my boss and her boss. At first, I was relieved; I was able to miss work for an intensive outpatient program (IOP) and come in after or work extra when I was able. Later on, though, it was unintentionally used against me. People, not understanding the disorder, would question my mood at any little shift they didn’t like. My workload had slowed and I asked and asked for more work, but no one gave me any. I was considered angry and hostile when I voiced my opinion or wouldn’t participate in unprofessional office behavior. After many angry, upset, crying days, along with several medicine changes, I began to look for a new job.
These things could later be used against me. This happened at my current job. I was not doing well, in a depressive episode, and I got tired of questions and comments so I told someone. That one turned in to two, then three, then my entire office, my boss and her boss. At first, I was relieved; I was able to miss work for an intensive outpatient program (IOP) and come in after or work extra when I was able. Later on, though, it was unintentionally used against me. People, not understanding the disorder, would question my mood at any little shift they didn’t like. My workload had slowed and I asked and asked for more work, but no one gave me any. I was considered angry and hostile when I voiced my opinion or wouldn’t participate in unprofessional office behavior. After many angry, upset, crying days, along with several medicine changes, I began to look for a new job.
So here we are, about to interview for job number 13 since diagnosis. What should I do at the next job? I have thought long and hard about this. Do I tell my new potential employer or do I keep it under lock and key — which one is the right choice? I honestly do not think there is a wrong decision. You have to do what is right in your situation at the time. My resumé may be complicated at best, an unfortunate side effect of job jumping, but think how much I have learned thus far. The only thing I do know is I will be as smart as I can be with my decision… or I will learn even more on job number 14.
Do I tell my new potential employer or do I keep it under lock and key — which one is the right choice? I honestly do not think there is a wrong decision. You have to do what is right in your situation at the time. My resumé may be complicated at best, an unfortunate side effect of job jumping, but think how much I have learned thus far. The only thing I do know is I will be as smart as I can be with my decision… or I will learn even more on job number 14.
— Penned by Penelope
The Mighty iPhone App is here!
Get it now.
Photo by Clarisa Guerra on Unsplash
Bipolar affective disorder and everything you need to know about it
More than 60 million people in the world suffer from bipolar affective disorder (BAD). The essence of the disease is that a person has alternating periods of altered mood throughout his life: from a state with a minus sign to a state with a plus sign. How and why is this happening?
Marina KINKULKINA, psychiatrist of the highest category, head of the department of psychiatry and narcology, director of the Institute of Electronic Medical Education, First Moscow State Medical University.![]() I. M. Sechenova, Corresponding Member of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences
I. M. Sechenova, Corresponding Member of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences
Moreover, it is often not just about sadness or fun, as is often the case with emotional people, but about extreme degrees of either despair or euphoria. The change in these moods can take place both gradually and suddenly, and often for no apparent reason. This disease is attributed to Byron and Hemingway, Virginia Woolf and Edgar Poe, Van Gogh, Schumann, Vivien Leigh and many others. There is an assumption that even “our everything” suffered from a mild degree of BAD (contemporaries often mentioned mood swings) A. S. Pushkin. Modern stars - Catherine Zeta-Jones and Mel Gibson - openly admit to having this mental disorder. And rapper Kanye West even put the inscription on the cover of his album: "I hate being bipolar, it's amazing." A very accurate description of the essence of this disease.
Genetics does not solve everything
BAD affects both men and women, but the weaker sex - more often. As for the age of onset of the disease, this disorder can also appear in a teenager (especially if there is an appropriate heredity), and in an adult, and even in an elderly person. Everything is individual. The main risk factor is genetics, but a specific gene that would be responsible for the development of bipolar disorder has not been identified. This is a polygenic disorder, and it makes no sense to take genetic tests to find out how great the risk of getting sick is, because scientists still do not have a consensus on what specific combination of genes can lead to a violation. But even if there is a genetic predisposition, it is not certain that the disease will develop. This was proven by studies on identical twins, one of which developed bipolar disorder over the years, while the other did not. Accordingly, there must be some other predisposing moments. Science knows about some of them: life at the limit of possibilities with constant hands-on work, stress and chronic lack of sleep, as well as night shift work, frequent flights with a significant change in hourly flights and, of course, the use of psychoactive substances contribute to the development of the disease.
As for the age of onset of the disease, this disorder can also appear in a teenager (especially if there is an appropriate heredity), and in an adult, and even in an elderly person. Everything is individual. The main risk factor is genetics, but a specific gene that would be responsible for the development of bipolar disorder has not been identified. This is a polygenic disorder, and it makes no sense to take genetic tests to find out how great the risk of getting sick is, because scientists still do not have a consensus on what specific combination of genes can lead to a violation. But even if there is a genetic predisposition, it is not certain that the disease will develop. This was proven by studies on identical twins, one of which developed bipolar disorder over the years, while the other did not. Accordingly, there must be some other predisposing moments. Science knows about some of them: life at the limit of possibilities with constant hands-on work, stress and chronic lack of sleep, as well as night shift work, frequent flights with a significant change in hourly flights and, of course, the use of psychoactive substances contribute to the development of the disease. Therefore, they should be avoided. Scientists have yet to learn about other factors.
Therefore, they should be avoided. Scientists have yet to learn about other factors.
But not boring?
The number of people suffering from bipolar disorder among the population, according to various estimates, varies from fractions of one percent to several percent. Recently, psychiatrists note, the proportion of affective disorders has increased significantly, which can be explained by improved diagnostics. At first glance, the BAR does not look like something scary and dangerous. To ignorant people, this disorder even seems attractive - sometimes sad, sometimes fun, in general, you won’t get bored. In addition, being different from everyone else is now fashionable. And then, there is an opinion that people with BAD have higher intelligence and creative abilities than the “gray masses”. But even if this is so, then none of those who suffer from it will definitely call BAD a pleasant thing. It is especially difficult for those patients who do not seek medical help on time. Without treatment, both phases of bipolar disorder can last for months (although sometimes the disorder occurs with frequently alternating phases). Moreover, it is impossible to say which of the periods of the disease is more difficult, manic or depressive.
Without treatment, both phases of bipolar disorder can last for months (although sometimes the disorder occurs with frequently alternating phases). Moreover, it is impossible to say which of the periods of the disease is more difficult, manic or depressive.
Bad when very bad
Those who have experienced real depression say that this is the worst thing that can happen in life. In this state, the whole world is seen in black, the mood is depressed, self-esteem drops, life loses its meaning. A person suffering from BAD in the depressive phase perceives his very existence as a chain of tragic mistakes, constantly blaming himself for all the troubles and sins, even those that do not even exist. In addition to mental suffering, physical ones also arise: a person even moves with difficulty, as if swimming against the current, it is difficult for him to perform the most familiar actions. In addition, he can feel tension throughout the body, experience various pain sensations. With an average degree of depression, people often complain of debilitating pain in the abdomen and other parts of the body. On this occasion, they turn to doctors, but the diagnosis cannot be made. And the daily pain continues to harass. Psychiatrists call this somatoform symptomatology. With severe depression, many have the so-called atrial depression. Patients complain of pain and heaviness in the chest, they say that "a stone lies on the heart." But even an in-depth examination does not reveal cardiac causes.
With an average degree of depression, people often complain of debilitating pain in the abdomen and other parts of the body. On this occasion, they turn to doctors, but the diagnosis cannot be made. And the daily pain continues to harass. Psychiatrists call this somatoform symptomatology. With severe depression, many have the so-called atrial depression. Patients complain of pain and heaviness in the chest, they say that "a stone lies on the heart." But even an in-depth examination does not reveal cardiac causes.
Often, with depression, patients (especially the elderly) complain of difficulty in thinking, memory impairment, they say that they have become stupid, they believe that they are developing dementia, they are afraid of “losing their mind”. In fact, affective disorders do not destroy the intellect. When treated with antidepressants, when the mood stabilizes, abilities are restored.
But the worst consequence of depression is suicide. Most suicide attempts are made in this state. Sometimes people in a very pronounced depression, believing that they have done something irreparable, and believing that the consequences of their actions can harm loved ones, decide on extended suicides, in which they settle scores not only with their lives, but also take their loved ones with them ( more often children).
Sometimes people in a very pronounced depression, believing that they have done something irreparable, and believing that the consequences of their actions can harm loved ones, decide on extended suicides, in which they settle scores not only with their lives, but also take their loved ones with them ( more often children).
Bad when too good
The manic stage of BAD is subjectively more pleasant. Patients are not just in a very good, but in a great mood: they love the whole world and themselves in it. The reflection in the mirror pleases, there is not the slightest doubt about one’s own talents and mind, there is more than enough strength and energy, a bonus is accelerated mental activity. Many in this stage sleep for an hour a day, but do not experience fatigue. Sometimes they don’t sleep for whole days - and at least they are cheerful, like an “energizer”. It seems to be great. But no. With mania, desires and new ideas arise too quickly, so a person grabs at each new business, but, as a rule, does not bring any to the end.![]() So productivity at this stage is no more than during depression. But it would be nice if that was the only thing.
So productivity at this stage is no more than during depression. But it would be nice if that was the only thing.
The main danger of mania is that a person has no criticism at this moment, and he can do things that he will later regret very much. For example, he can give away all his property to others (sometimes to unfamiliar people or scammers who specifically use this state of his). Or, say, take out loans to go on a trip to the other side of the world, and take a bunch of friends with him. Maybe even steal something - for example, to make an expensive gift. Many patients at these moments enter into hasty intimate relationships, mistaking a chance meeting for the love of their life (and completely “forgetting” that family and children are waiting at home). Finally, often with mania, people, experiencing euphoria, ignore their severe somatic symptoms, as a result, they do not go to the doctor for a long time, and thus trigger a serious illness (pneumonia, for example). In addition, not all patients in the manic phase are "darlings. " Often they show unreasonable aggression if, for example, others do not agree with their "brilliant" advice. As a result of such “angry mania”, conflicts and even situations arise that require the intervention of law enforcement agencies and the hospitalization of the patient without his consent in a psychiatric hospital.
" Often they show unreasonable aggression if, for example, others do not agree with their "brilliant" advice. As a result of such “angry mania”, conflicts and even situations arise that require the intervention of law enforcement agencies and the hospitalization of the patient without his consent in a psychiatric hospital.
Good intentions…
The worst thing that relatives and friends of a person with bipolar disorder can do is ignore his problem, devalue suffering, while blaming the patient himself and appealing to his conscience. For example, they can call on a depressed person to “pull himself together, not become limp”, say that he is “mad with fat”, etc. A patient at the stage of mania is most often accused of immorality, irresponsibility, frivolity, promiscuity in relationships, etc. However, doing so is like blaming a person with diabetes for not being able to eat sweet cake, or a patient with heart failure for not running a marathon. BAD is a disease like many others. And she needs to be treated. The sooner you start the right therapy, the sooner you can stabilize the patient's condition and the better the further prognosis will be.
And she needs to be treated. The sooner you start the right therapy, the sooner you can stabilize the patient's condition and the better the further prognosis will be.
Psychiatrists don't bite
Despite the fact that recently people (especially young people) have ceased to be afraid to turn to psychiatrists, not everyone still decides to go to the doctor. Indeed, on the Internet in the public domain, you can find hundreds of questionnaires to test yourself for any mental disorder. And then, after reading various tips, you can also “cure”. Doctors strongly advise against doing this. The smallest harm of self-treatment is that it will not help or lead to incomplete improvement, but it can also worsen the condition. For example, inadequate intake of antidepressants in bipolar disorder can lead from a depressive phase into a severe manic state, from which it will then be difficult to get out. Only a psychiatrist (and not a psychologist, neurologist or doctor of any other somatic profile) can identify bipolar disorder and choose the right treatment.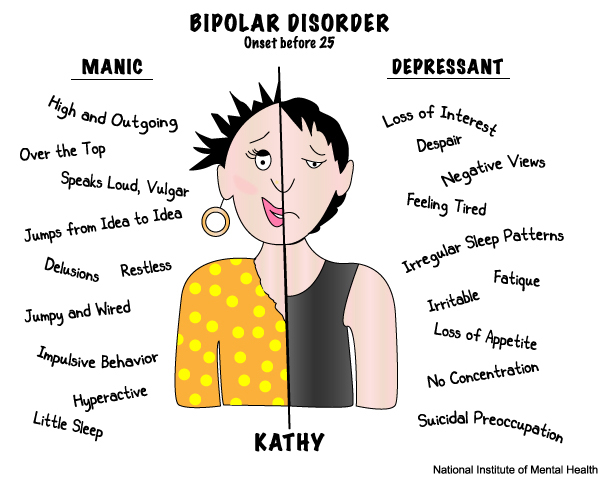 Treatment should be strictly individual, that is, the doctor selects it based on the characteristics of a particular patient and taking into account a specific moment in the course of the disease. The goal of therapy is not only to equalize the patient's mood, but also to prevent recurrence. In the treatment of bipolar disorder, the main role is played by drugs for stabilizing mood - mood stabilizers (lithium salts, some anticonvulsants (anticonvulsants) and antipsychotics of new generations). Modern drugs are much better tolerated than their predecessors, have fewer side effects, as they are designed for long-term use over many years. Against the background of their intake, women can even become pregnant and give birth. In depression, antidepressants are prescribed in exceptional cases, given the danger of changing the depressive stage to manic.
Treatment should be strictly individual, that is, the doctor selects it based on the characteristics of a particular patient and taking into account a specific moment in the course of the disease. The goal of therapy is not only to equalize the patient's mood, but also to prevent recurrence. In the treatment of bipolar disorder, the main role is played by drugs for stabilizing mood - mood stabilizers (lithium salts, some anticonvulsants (anticonvulsants) and antipsychotics of new generations). Modern drugs are much better tolerated than their predecessors, have fewer side effects, as they are designed for long-term use over many years. Against the background of their intake, women can even become pregnant and give birth. In depression, antidepressants are prescribed in exceptional cases, given the danger of changing the depressive stage to manic.
You won't be able to forget
The insidiousness of BAD is that this disease cannot be cured once and for all. But, alas, often, when the patient's mood can be balanced by medication and he begins to feel good (such a state - intermission - is completely indistinguishable from a state of complete health), he can stop taking the drugs. This is a big mistake that does not allow to achieve a stable result of treatment. Sometimes it is required to use medicines (necessarily under the supervision of a doctor) for several months, but more often for years (with periodic visits to the doctor). It is the long-term use of maintenance therapy individually selected by the doctor that allows patients to achieve a stable good condition and feel the joy of life for many years.
This is a big mistake that does not allow to achieve a stable result of treatment. Sometimes it is required to use medicines (necessarily under the supervision of a doctor) for several months, but more often for years (with periodic visits to the doctor). It is the long-term use of maintenance therapy individually selected by the doctor that allows patients to achieve a stable good condition and feel the joy of life for many years.
Link to publication: www.kiz.ru
Site embed code
More than 60 million people in the world suffer from bipolar affective disorder (BAD). The essence of the disease is that a person has alternating periods of altered mood throughout his life: from a state with a minus sign to a state with a plus sign. How and why is this happening?
Marina KINKULKINA, psychiatrist of the highest category, head of the department of psychiatry and narcology, director of the Institute of Electronic Medical Education, First Moscow State Medical University.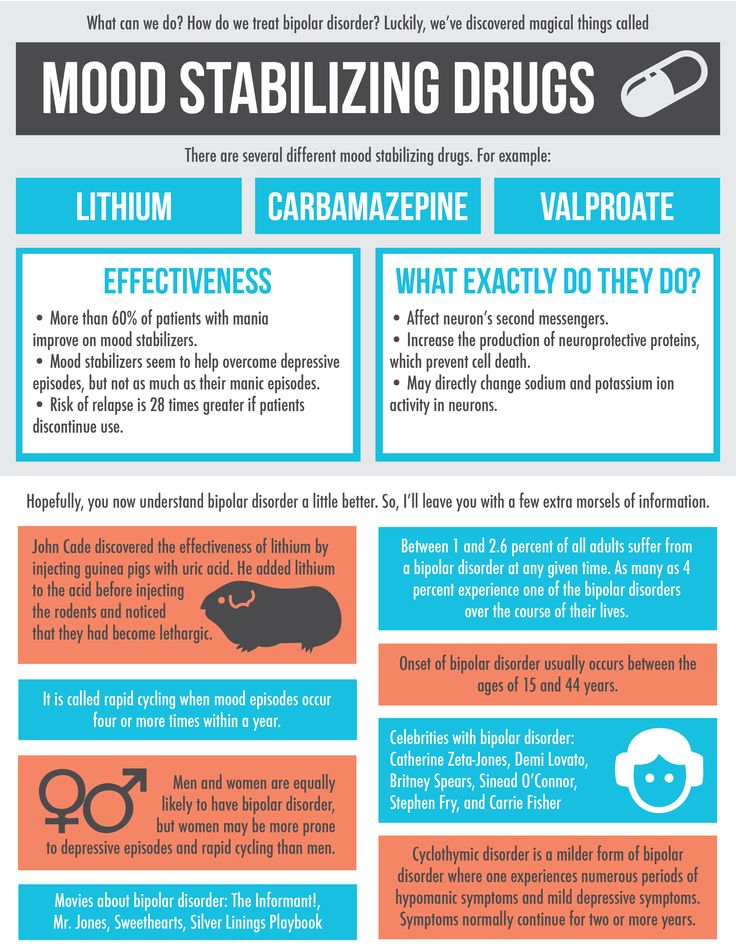 I. M. Sechenova, Corresponding Member of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences
I. M. Sechenova, Corresponding Member of the Russian Academy of Sciences, Professor, Doctor of Medical Sciences
Moreover, it is often not just about sadness or fun, as is often the case with emotional people, but about extreme degrees of either despair or euphoria. The change in these moods can take place both gradually and suddenly, and often for no apparent reason. This disease is attributed to Byron and Hemingway, Virginia Woolf and Edgar Poe, Van Gogh, Schumann, Vivien Leigh and many others. There is an assumption that even “our everything” suffered from a mild degree of BAD (contemporaries often mentioned mood swings) A. S. Pushkin. Modern stars - Catherine Zeta-Jones and Mel Gibson - openly admit to having this mental disorder. And rapper Kanye West even put the inscription on the cover of his album: "I hate being bipolar, it's amazing." A very accurate description of the essence of this disease.
Genetics does not solve everything
BAD affects both men and women, but the weaker sex - more often. As for the age of onset of the disease, this disorder can also appear in a teenager (especially if there is an appropriate heredity), and in an adult, and even in an elderly person. Everything is individual. The main risk factor is genetics, but a specific gene that would be responsible for the development of bipolar disorder has not been identified. This is a polygenic disorder, and it makes no sense to take genetic tests to find out how great the risk of getting sick is, because scientists still do not have a consensus on what specific combination of genes can lead to a violation. But even if there is a genetic predisposition, it is not certain that the disease will develop. This was proven by studies on identical twins, one of which developed bipolar disorder over the years, while the other did not. Accordingly, there must be some other predisposing moments. Science knows about some of them: life at the limit of possibilities with constant hands-on work, stress and chronic lack of sleep, as well as night shift work, frequent flights with a significant change in hourly flights and, of course, the use of psychoactive substances contribute to the development of the disease.
As for the age of onset of the disease, this disorder can also appear in a teenager (especially if there is an appropriate heredity), and in an adult, and even in an elderly person. Everything is individual. The main risk factor is genetics, but a specific gene that would be responsible for the development of bipolar disorder has not been identified. This is a polygenic disorder, and it makes no sense to take genetic tests to find out how great the risk of getting sick is, because scientists still do not have a consensus on what specific combination of genes can lead to a violation. But even if there is a genetic predisposition, it is not certain that the disease will develop. This was proven by studies on identical twins, one of which developed bipolar disorder over the years, while the other did not. Accordingly, there must be some other predisposing moments. Science knows about some of them: life at the limit of possibilities with constant hands-on work, stress and chronic lack of sleep, as well as night shift work, frequent flights with a significant change in hourly flights and, of course, the use of psychoactive substances contribute to the development of the disease. Therefore, they should be avoided. Scientists have yet to learn about other factors.
Therefore, they should be avoided. Scientists have yet to learn about other factors.
But not boring?
The number of people suffering from bipolar disorder among the population, according to various estimates, varies from fractions of one percent to several percent. Recently, psychiatrists note, the proportion of affective disorders has increased significantly, which can be explained by improved diagnostics. At first glance, the BAR does not look like something scary and dangerous. To ignorant people, this disorder even seems attractive - sometimes sad, sometimes fun, in general, you won’t get bored. In addition, being different from everyone else is now fashionable. And then, there is an opinion that people with BAD have higher intelligence and creative abilities than the “gray masses”. But even if this is so, then none of those who suffer from it will definitely call BAD a pleasant thing. It is especially difficult for those patients who do not seek medical help on time. Without treatment, both phases of bipolar disorder can last for months (although sometimes the disorder occurs with frequently alternating phases). Moreover, it is impossible to say which of the periods of the disease is more difficult, manic or depressive.
Without treatment, both phases of bipolar disorder can last for months (although sometimes the disorder occurs with frequently alternating phases). Moreover, it is impossible to say which of the periods of the disease is more difficult, manic or depressive.
Bad when very bad
Those who have experienced real depression say that this is the worst thing that can happen in life. In this state, the whole world is seen in black, the mood is depressed, self-esteem drops, life loses its meaning. A person suffering from BAD in the depressive phase perceives his very existence as a chain of tragic mistakes, constantly blaming himself for all the troubles and sins, even those that do not even exist. In addition to mental suffering, physical ones also arise: a person even moves with difficulty, as if swimming against the current, it is difficult for him to perform the most familiar actions. In addition, he can feel tension throughout the body, experience various pain sensations. With an average degree of depression, people often complain of debilitating pain in the abdomen and other parts of the body. On this occasion, they turn to doctors, but the diagnosis cannot be made. And the daily pain continues to harass. Psychiatrists call this somatoform symptomatology. With severe depression, many have the so-called atrial depression. Patients complain of pain and heaviness in the chest, they say that "a stone lies on the heart." But even an in-depth examination does not reveal cardiac causes.
With an average degree of depression, people often complain of debilitating pain in the abdomen and other parts of the body. On this occasion, they turn to doctors, but the diagnosis cannot be made. And the daily pain continues to harass. Psychiatrists call this somatoform symptomatology. With severe depression, many have the so-called atrial depression. Patients complain of pain and heaviness in the chest, they say that "a stone lies on the heart." But even an in-depth examination does not reveal cardiac causes.
Often, with depression, patients (especially the elderly) complain of difficulty in thinking, memory impairment, they say that they have become stupid, they believe that they are developing dementia, they are afraid of “losing their mind”. In fact, affective disorders do not destroy the intellect. When treated with antidepressants, when the mood stabilizes, abilities are restored.
But the worst consequence of depression is suicide. Most suicide attempts are made in this state. Sometimes people in a very pronounced depression, believing that they have done something irreparable, and believing that the consequences of their actions can harm loved ones, decide on extended suicides, in which they settle scores not only with their lives, but also take their loved ones with them ( more often children).
Sometimes people in a very pronounced depression, believing that they have done something irreparable, and believing that the consequences of their actions can harm loved ones, decide on extended suicides, in which they settle scores not only with their lives, but also take their loved ones with them ( more often children).
Bad when too good
The manic stage of BAD is subjectively more pleasant. Patients are not just in a very good, but in a great mood: they love the whole world and themselves in it. The reflection in the mirror pleases, there is not the slightest doubt about one’s own talents and mind, there is more than enough strength and energy, a bonus is accelerated mental activity. Many in this stage sleep for an hour a day, but do not experience fatigue. Sometimes they don’t sleep for whole days - and at least they are cheerful, like an “energizer”. It seems to be great. But no. With mania, desires and new ideas arise too quickly, so a person grabs at each new business, but, as a rule, does not bring any to the end. So productivity at this stage is no more than during depression. But it would be nice if that was the only thing.
So productivity at this stage is no more than during depression. But it would be nice if that was the only thing.
The main danger of mania is that a person has no criticism at this moment, and he can do things that he will later regret very much. For example, he can give away all his property to others (sometimes to unfamiliar people or scammers who specifically use this state of his). Or, say, take out loans to go on a trip to the other side of the world, and take a bunch of friends with him. Maybe even steal something - for example, to make an expensive gift. Many patients at these moments enter into hasty intimate relationships, mistaking a chance meeting for the love of their life (and completely “forgetting” that family and children are waiting at home). Finally, often with mania, people, experiencing euphoria, ignore their severe somatic symptoms, as a result, they do not go to the doctor for a long time, and thus trigger a serious illness (pneumonia, for example). In addition, not all patients in the manic phase are "darlings. " Often they show unreasonable aggression if, for example, others do not agree with their "brilliant" advice. As a result of such “angry mania”, conflicts and even situations arise that require the intervention of law enforcement agencies and the hospitalization of the patient without his consent in a psychiatric hospital.
" Often they show unreasonable aggression if, for example, others do not agree with their "brilliant" advice. As a result of such “angry mania”, conflicts and even situations arise that require the intervention of law enforcement agencies and the hospitalization of the patient without his consent in a psychiatric hospital.
Good intentions…
The worst thing that relatives and friends of a person with bipolar disorder can do is ignore his problem, devalue suffering, while blaming the patient himself and appealing to his conscience. For example, they can call on a depressed person to “pull himself together, not become limp”, say that he is “mad with fat”, etc. A patient at the stage of mania is most often accused of immorality, irresponsibility, frivolity, promiscuity in relationships, etc. However, doing so is like blaming a person with diabetes for not being able to eat sweet cake, or a patient with heart failure for not running a marathon. BAD is a disease like many others. And she needs to be treated. The sooner you start the right therapy, the sooner you can stabilize the patient's condition and the better the further prognosis will be.
And she needs to be treated. The sooner you start the right therapy, the sooner you can stabilize the patient's condition and the better the further prognosis will be.
Psychiatrists don't bite
Despite the fact that recently people (especially young people) have ceased to be afraid to turn to psychiatrists, not everyone still decides to go to the doctor. Indeed, on the Internet in the public domain, you can find hundreds of questionnaires to test yourself for any mental disorder. And then, after reading various tips, you can also “cure”. Doctors strongly advise against doing this. The smallest harm of self-treatment is that it will not help or lead to incomplete improvement, but it can also worsen the condition. For example, inadequate intake of antidepressants in bipolar disorder can lead from a depressive phase into a severe manic state, from which it will then be difficult to get out. Only a psychiatrist (and not a psychologist, neurologist or doctor of any other somatic profile) can identify bipolar disorder and choose the right treatment.![]() Treatment should be strictly individual, that is, the doctor selects it based on the characteristics of a particular patient and taking into account a specific moment in the course of the disease. The goal of therapy is not only to equalize the patient's mood, but also to prevent recurrence. In the treatment of bipolar disorder, the main role is played by drugs for stabilizing mood - mood stabilizers (lithium salts, some anticonvulsants (anticonvulsants) and antipsychotics of new generations). Modern drugs are much better tolerated than their predecessors, have fewer side effects, as they are designed for long-term use over many years. Against the background of their intake, women can even become pregnant and give birth. In depression, antidepressants are prescribed in exceptional cases, given the danger of changing the depressive stage to manic.
Treatment should be strictly individual, that is, the doctor selects it based on the characteristics of a particular patient and taking into account a specific moment in the course of the disease. The goal of therapy is not only to equalize the patient's mood, but also to prevent recurrence. In the treatment of bipolar disorder, the main role is played by drugs for stabilizing mood - mood stabilizers (lithium salts, some anticonvulsants (anticonvulsants) and antipsychotics of new generations). Modern drugs are much better tolerated than their predecessors, have fewer side effects, as they are designed for long-term use over many years. Against the background of their intake, women can even become pregnant and give birth. In depression, antidepressants are prescribed in exceptional cases, given the danger of changing the depressive stage to manic.
You won't be able to forget
The insidiousness of BAD is that this disease cannot be cured once and for all. But, alas, often, when the patient's mood can be balanced by medication and he begins to feel good (such a state - intermission - is completely indistinguishable from a state of complete health), he can stop taking the drugs. This is a big mistake that does not allow to achieve a stable result of treatment. Sometimes it is required to use medicines (necessarily under the supervision of a doctor) for several months, but more often for years (with periodic visits to the doctor). It is the long-term use of maintenance therapy individually selected by the doctor that allows patients to achieve a stable good condition and feel the joy of life for many years.
This is a big mistake that does not allow to achieve a stable result of treatment. Sometimes it is required to use medicines (necessarily under the supervision of a doctor) for several months, but more often for years (with periodic visits to the doctor). It is the long-term use of maintenance therapy individually selected by the doctor that allows patients to achieve a stable good condition and feel the joy of life for many years.
Bipolar affective disorder (BAD), its signs, types and methods of treatment
Manifestations of various emotions, a change in a person's mood, manifestations of both sadness and joy are normal and depend on many factors - from temperament and character to ongoing events that influence from the outside. However, when these changes are excessive, often unexpected and for no apparent reason, emotions get out of control, or a person remains in a radically positive or negative mood for a long time, it is very likely that bipolar disorder can be diagnosed. This disease was first described at the end of 19century, the famous German psychiatrist Emil Kripelin, calling it manic-depressive psychosis. Many world famous personalities such as Vincent van Gogh, Isaac Newton, Ludwig van Beethoven, Abraham Lincoln suffered from this disease. The pronounced form of this disease, which in the international classification of diseases is called bipolar affective disorder (BAD), is detected in 3% of the world's population.
This disease was first described at the end of 19century, the famous German psychiatrist Emil Kripelin, calling it manic-depressive psychosis. Many world famous personalities such as Vincent van Gogh, Isaac Newton, Ludwig van Beethoven, Abraham Lincoln suffered from this disease. The pronounced form of this disease, which in the international classification of diseases is called bipolar affective disorder (BAD), is detected in 3% of the world's population.
CONTENT OF ARTICLE
- 1. Bipolar Personality Disorder - Overview
- 2. Symptoms and signs
- 3. Types of bipolar disorder
- 4. Phases of Bipolar Disorder
- 5. Bipolar disorder in women
- 6. Treatment of Bipolar Personality Disorder
It is not uncommon for women to be treated with a combination of drug therapy and cognitive-behavioral or interpersonal therapy with a psychotherapist.
Bipolar personality disorder - general information
According to statistics, bipolar disorder affects people between the ages of 14 and 44. Unlike adults, children and adolescents experience more frequent mood swings from mania to depression, sometimes several times a day. 90% of young people make their debut precisely from the phase of depression or melancholy. Another feature of bipolar disorder is that, due to the low level of diagnosis, the patient can live with this disease for 5-10 years without knowing the cause of the painful symptoms.
Unlike adults, children and adolescents experience more frequent mood swings from mania to depression, sometimes several times a day. 90% of young people make their debut precisely from the phase of depression or melancholy. Another feature of bipolar disorder is that, due to the low level of diagnosis, the patient can live with this disease for 5-10 years without knowing the cause of the painful symptoms.
Most often, bipolar disorder is diagnosed in people whose immediate family members have had a similar problem. The causes of this disease are unknown, but stress, overstrain, and various diseases can provoke the manifestation of its symptoms. However, having fenced off a person from the influence of these factors, it is impossible to get rid of the problem, you need to seek help from a psychotherapist.
Bipolar disorder is a disease that cannot be completely cured. But with properly selected medication and psychotherapy, the quality of life is significantly improved and the periods between phases are lengthened.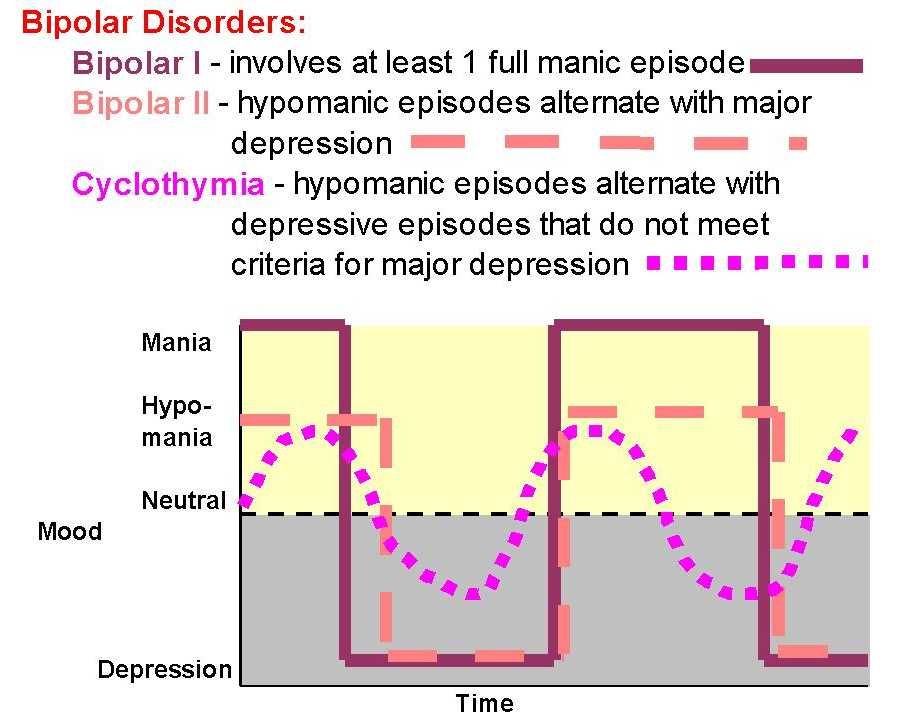 The person remains socialized and able to work.
The person remains socialized and able to work.
Symptoms and signs
From the name it is clear that we are talking about two different poles of affective manifestations, that is, mood manifestations. One of these conditions is depression. Depression in bipolar disorder is pronounced, with vivid symptoms. It can last up to a year and is manifested not only by low mood, lack of ability to enjoy and interest in ongoing events, but also by psychosis, when ideas of self-accusation arise, the patient feels inferior, unnecessary, poisoning the life of others. There are also nihilistic thoughts about suffering from some kind of severe illness, despite medical evidence to the contrary. There may be delusional thoughts, as well as suicidal thoughts and even attempts.
The other pole of bipolar disorder is a hypomanic state or hypomania, the characteristic features of which are an increased euphoric emotional background, the patient is constantly on the move, hyperactive, and is distinguished by very fast, associative speech. The patient is constantly cheerful, often hypersexual, almost always awake or sleeping 2-3 hours a day.
The patient is constantly cheerful, often hypersexual, almost always awake or sleeping 2-3 hours a day.
Hypomania is often followed by a manic bipolar state with psychotic manifestations. The patient develops convictions in his own greatness, he believes that he is capable of anything, feels that he has a special calling in this world or that he is a descendant of great people. In extended manic episodes of mania with psychotic manifestations, anger, irritability, and direct aggression often occur. This condition leads the patient into extremely unpleasant and sometimes dangerous situations.
In addition to the typical symptoms of the disease, there are a large number of comorbid mental disorders. Comorbid mental disorders are those that accompany the underlying disease. The most common disorder of this kind is anxiety, which is manifested, among other things, by nonspecific autonomic symptoms, including sweating, palpitations, tremors of the limbs, various disorders of the gastrointestinal tract, dizziness, headaches, suffocation, and many others. In the case when these symptoms occur suddenly, mainly in public places, they are called panic attacks.
In the case when these symptoms occur suddenly, mainly in public places, they are called panic attacks.
Types of bipolar disorder
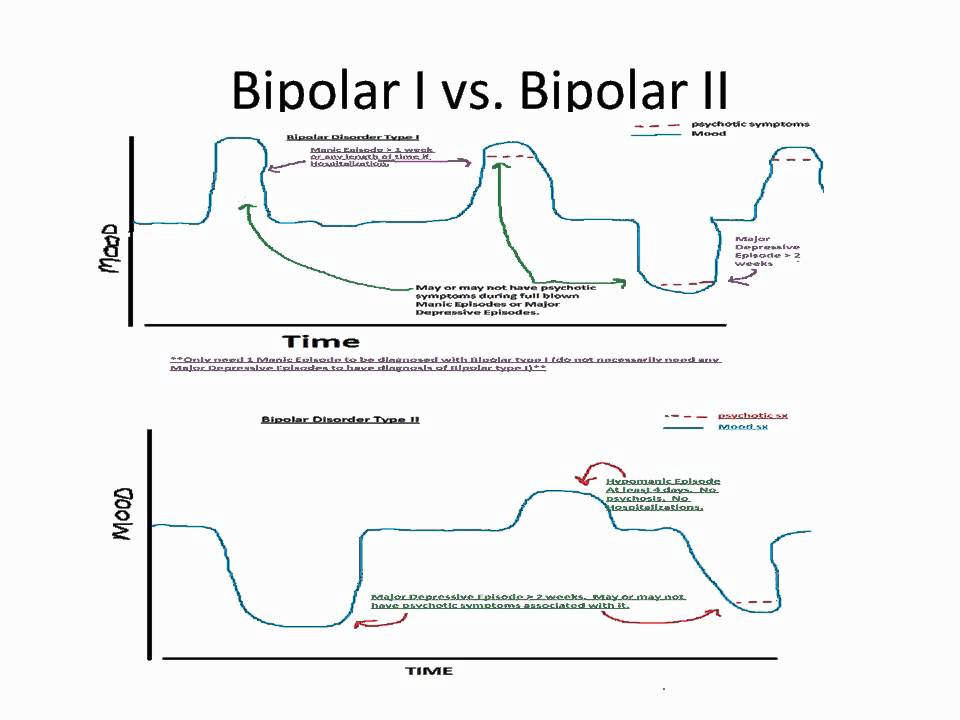
Bipolar disorder can be of Ι and ΙΙ types.
Bipolar I disorder is a condition in which the patient has persistent manias, i.e. overexcitation, enthusiastic inappropriate behavior, manic psychosis, as well as severe depressions. Symptoms of this type are more severe, so hospitalization is indicated in most cases.
Bipolar I disorder is characterized by short periods of hypomania followed by periods of deep depression. Hypomania is a pre-manic state with less active manifestations. Hypomania lasts a very short period of time - from several days to several hours, so sometimes patients do not even notice them and do not inform the doctor about it. Only careful, painstaking work with the patient makes it possible to identify hypomania, make the correct diagnosis and prescribe treatment.
Phases of bipolar disorder
There are several phases of bipolar personality disorder:
- Depressive (unipolar depression).
 People experience a depressed mood, despair and despondency, complain of a lack of energy and mental concentration, they can either eat too much or too little and sleep.
People experience a depressed mood, despair and despondency, complain of a lack of energy and mental concentration, they can either eat too much or too little and sleep.
Depersonalization and derealization may occur at the peak of bipolar depressive disorder. The boundaries of their own "I" and the world around them become blurred, patients experience difficulties in perceiving what is happening. Familiar places seem new, the colors of the surrounding world change, the patient constantly experiences a feeling of "déjà vu". Sounds become muffled, even if someone is talking very close, it seems to the patient that the voice is coming from afar.
- Manic (hypomanic). In this state, patients are full of energy, overly happy or optimistic, euphoric, and have extremely high self-esteem. At first glance, these are positive signs, but when a person experiences large-scale manic episodes, these symptoms and such an emotional state can reach dangerous extremes.
 A patient in this phase may indiscriminately spend huge amounts of money or behave carelessly, not realizing the full danger. In conversation, people may choke on words, speak at a high speed, or jump from one thought to another. These episodes may also be accompanied by delusions of grandeur or the adoption of serious decisions without thinking about the further consequences.
A patient in this phase may indiscriminately spend huge amounts of money or behave carelessly, not realizing the full danger. In conversation, people may choke on words, speak at a high speed, or jump from one thought to another. These episodes may also be accompanied by delusions of grandeur or the adoption of serious decisions without thinking about the further consequences.
In the development of the manic phase, the following stages of development can be distinguished:
- Hypomania - increased arousal, emotional upsurge.
- Mania - all signs are more pronounced, aggression, irritability, irascibility and rage are possible.
- Phase peak. The patient constantly experiences nervous excitement, he cannot relax. All his emotions are "heated" to the limit, coordination of movements is disturbed, thoughts are illogical and abrupt, in speech he constantly jumps from one sentence to another.
- Relief of symptoms. The patient gradually calms down.
 Movement disorders are on the decline. The speed of thinking and increased emotional mood remain unchanged.
Movement disorders are on the decline. The speed of thinking and increased emotional mood remain unchanged. - Return to normal.
- Mixed. Sometimes people have complaints that are characteristic of both depression and mania at the same time. They may also experience frequent phasing—4 or more episodes in one year.
In the intervals between depressive and manic phases in bipolar disorder, there is a light period during which the general background of mood becomes relatively stable, the person continues to adequately respond to certain events, the emotional sphere is under his control. This is the main criterion for remission of bipolar disease.
Bipolar disorder in women
According to statistics, bipolar Ι disorder occurs with the same frequency in men and women, and type ΙΙ disease is more often diagnosed in women. It is also known that the female course of the disease is characterized by rapid cycles and mixed episodes.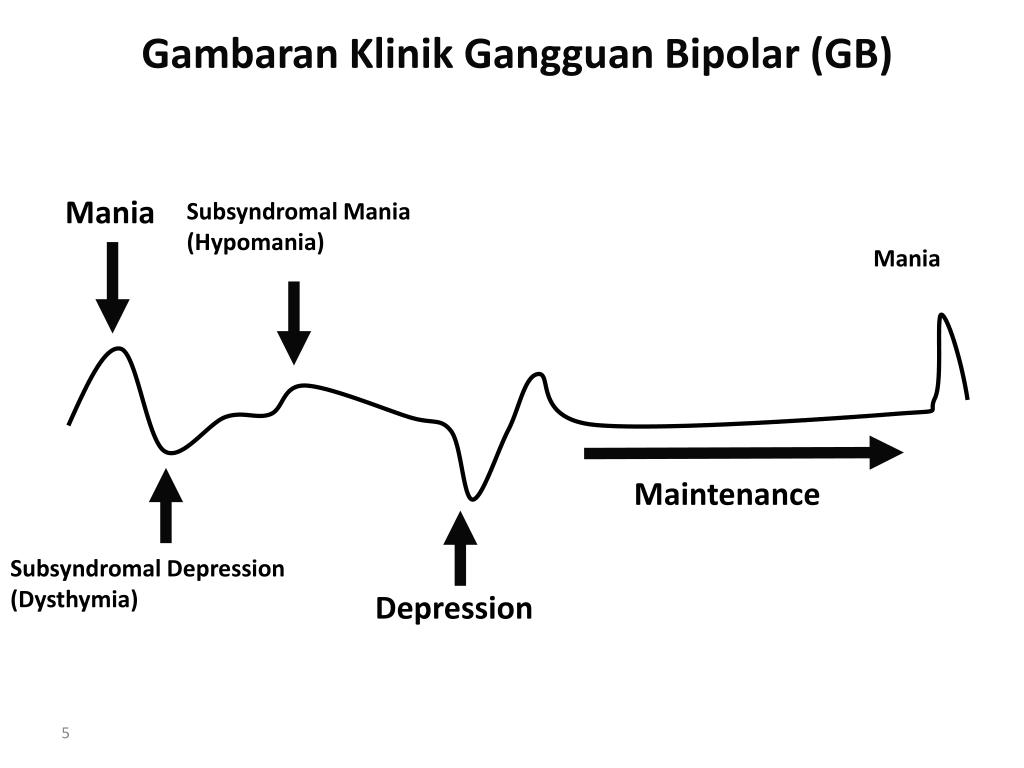 Comorbidities often include eating disorders, borderline personality disorder, alcohol or drug addiction, and psychotropic drug abuse. Women are more susceptible to such somatic diseases as migraine (intense headaches), thyroid pathologies, diabetes, and obesity.
Comorbidities often include eating disorders, borderline personality disorder, alcohol or drug addiction, and psychotropic drug abuse. Women are more susceptible to such somatic diseases as migraine (intense headaches), thyroid pathologies, diabetes, and obesity.
For women, a special technique is being developed to alleviate this disorder, since from adolescence to menopause there are specific changes in hormonal levels that must be taken into account. In addition, psychotropic substances, which are supposed to stabilize the condition, can adversely affect the intrauterine development of the fetus if the woman is in position. It is noted that in the first trimester of pregnancy this disorder is milder, but after childbirth they often have to deal with postpartum depression. Thus, at each stage of the development of the female body, a competent doctor must review and adjust the treatment regimen. Often in the treatment of women, a complex method is used that combines drug therapy and cognitive-behavioral or interpersonal therapy with a psychotherapist.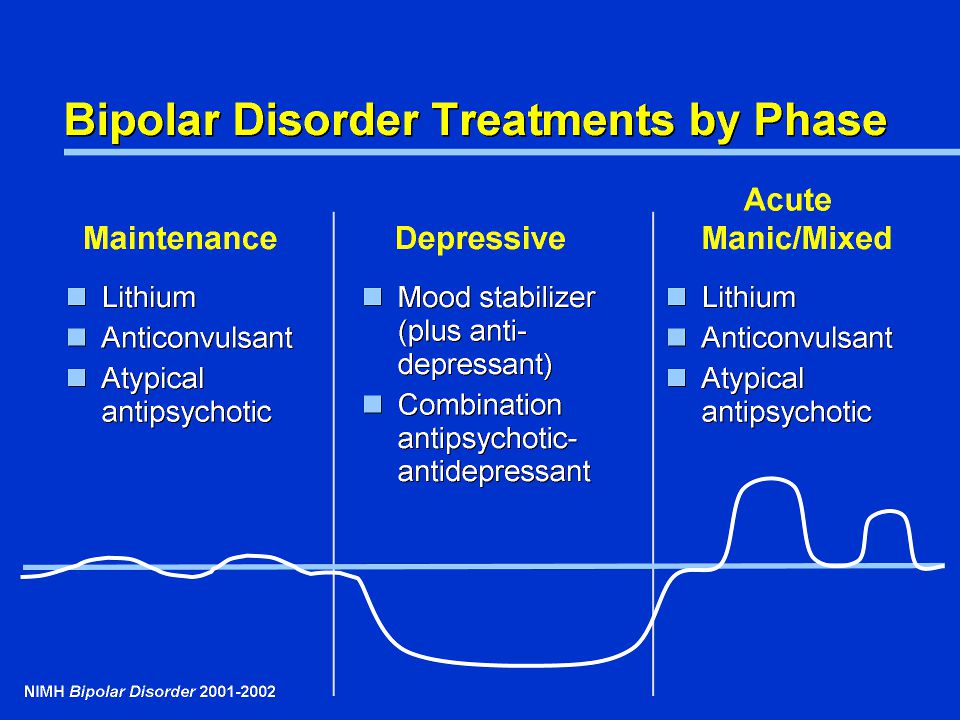 This approach gives the fastest results.
This approach gives the fastest results.
Treatment for bipolar disorder
Attempts to get rid of bipolar disorder on your own do not bring the desired result and, ultimately, lead to an aggravation of the situation, including the development of drug or alcohol dependence. In the diagnosis of the disease, keeping a mood diary can help, where the patient records all his thoughts, emotions, feelings, changes in mood. Such records will help the doctor to assess the mental state in detail and make the correct diagnosis. If you suspect bipolar disorder, you should consult a doctor, and the sooner a person realizes that he has a disease and comes to the clinic for help, the sooner professional help will be provided to him and painful symptoms will be replaced by a stable condition. It is impossible to get rid of the disease on your own, since a person cannot fully adequately assess not only his actions, but also the alternation of the phases of the disease.
Bipolar disorder is one of the few mental disorders in which medication is indicated in 100% of cases, and psychotherapy is an auxiliary tool.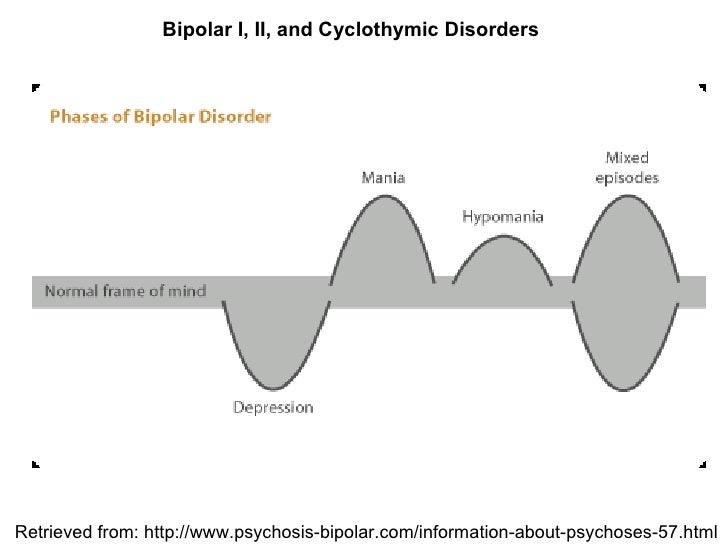 This disease is incurable, but its diagnosis and treatment is extremely important. Treatment can reduce the number of episodes, their severity and intensity, as well as prevent negative life events, help prevent relationship breakups, job loss, and even suicidal attempts. Thus, the quality of life of a patient with bipolar disorder who is undergoing treatment will be several times higher than that of a person who neglects treatment. If the patient loses touch with reality and harms himself and others, he is subject to hospitalization, outpatient treatment in this case is not permissible.
This disease is incurable, but its diagnosis and treatment is extremely important. Treatment can reduce the number of episodes, their severity and intensity, as well as prevent negative life events, help prevent relationship breakups, job loss, and even suicidal attempts. Thus, the quality of life of a patient with bipolar disorder who is undergoing treatment will be several times higher than that of a person who neglects treatment. If the patient loses touch with reality and harms himself and others, he is subject to hospitalization, outpatient treatment in this case is not permissible.
If you have a disease, it is recommended to exclude coffee, strong tea, alcoholic and energy drinks from your diet in order not to provoke an overexcited state. If possible, you should stop smoking and in no case should you take even soft drugs. It is also very important to establish a sleep pattern, sleep at least 8 hours a day and try to go to bed at about the same time. You should learn to recognize mood swings and notice the early manifestations of new episodes.![]()