Bipolar disorder in children under 5
Pediatric Bipolar Disorder - CHADD
The existence of a mood disorder in adults involving severe mood swings from states of deep depression to states of elation has been recognized now for over a century. This disorder is commonly referred to as manic-depression but is now formally referred to as bipolar disorder, referring to the two “poles” of depression and mania. Until recently, however, youth were rarely diagnosed with this disorder. Bipolar disorder has also become a controversial area within the field of children’s mental health. There is little disagreement about whether it exists. The disagreement is about the symptoms of bipolar disorder in youth and how they differ from those in adults.
First, some definitions
Bipolar disorder involves episodes of both major depression and mania. (To clarify, major depression is another, separate mood disorder involving these same symptoms of depression but without the occurrence of symptoms of mania). The diagnostic manual used by mental health professionals is based on the diagnosis of bipolar disorder in adults. The following lists consist of behaviors observed by parents of children diagnosed with bipolar disorder.
Behaviors connected to major depressive episodes:
- marked decrease in interest in or pleasure from life, sometimes expressed by boredom
- agitation and irritability
- sleeping too much or inability to sleep
- significant change in appetite
- change in observed activity level (usually slowed down or dragging)
- loss of energy
- inability to concentrate
- frequent sadness or crying
- feelings of worthlessness or guilt
- thoughts of death or suicide or self-destructive behavior
Behaviors connected to mania:
- elevated, expansive or irritable mood
- inflated self esteem or grandiosity (an unrealistic sense of one’s capabilities)
- significantly decreased need for sleep
- much more talkative or pressured speech (speech so rapid that the words bump into and overrun each other)
- racing thoughts or flight of ideas (completely disconnected thoughts)
- distractibility
- excessive involvement in multiple projects and activities
- highly risky pursuit of pleasurable activities (for example, activities involving drugs, alcohol or sex)
The combination of episodes of mania and major depressive episodes is what constitutes classic bipolar disorder. However, more than one type of bipolar disorder exists.
However, more than one type of bipolar disorder exists.
The controversy
As mentioned earlier, mental health practitioners disagree about the symptoms of bipolar disorder in youth and how they differ from those in adults. In adolescents, where the presentation of the disorder more closely resembles that seen in adults, there is much less controversy.
More controversy exists in children when there appears to be a more chronic course, including more irritability and unstable moods, including severe temper outbursts. In short, where does a child with ADHD, oppositional behaviors, and a fair degree of crankiness/moodiness end, and where does a child with bipolar disorder begin.
While no one has the definitive answers to these questions, there are competing schools of thought on this issue. Some experts feel that children with severe irritability, emotional instability, and severe temper outbursts are, in fact, suffering from bipolar disorder as it appears in childhood and should be treated accordingly. Other experts feel this approach will lead to the overdiagnosis of children who in fact suffer from disorders other than bipolar disorder. These experts argue for a narrower definition of bipolar disorder which includes episodic mood swings, elevated or expansive mood—not just irritable mood—and grandiosity or inappropriate euphoria (extreme joyfulness).
Other experts feel this approach will lead to the overdiagnosis of children who in fact suffer from disorders other than bipolar disorder. These experts argue for a narrower definition of bipolar disorder which includes episodic mood swings, elevated or expansive mood—not just irritable mood—and grandiosity or inappropriate euphoria (extreme joyfulness).
These experts clearly recognize that this definition excludes a number of children with episodes of mood instability, explosive rage episodes, extreme irritability and agitation. There is no disagreement that children with these symptoms are impaired. However, experts differ on whether or not such children should be diagnosed with bipolar disorder. Experts also differ on what would be the most appropriate and effective treatment for them.
There are also other factors that can seriously complicate the diagnosis of bipolar disorder in children. A history of severe emotional trauma such as physical or sexual abuse can lead to mood swings, emotional outbursts, hallucinations, and extremely severe behavioral problems, including sexualized behaviors that can resemble bipolar disorder.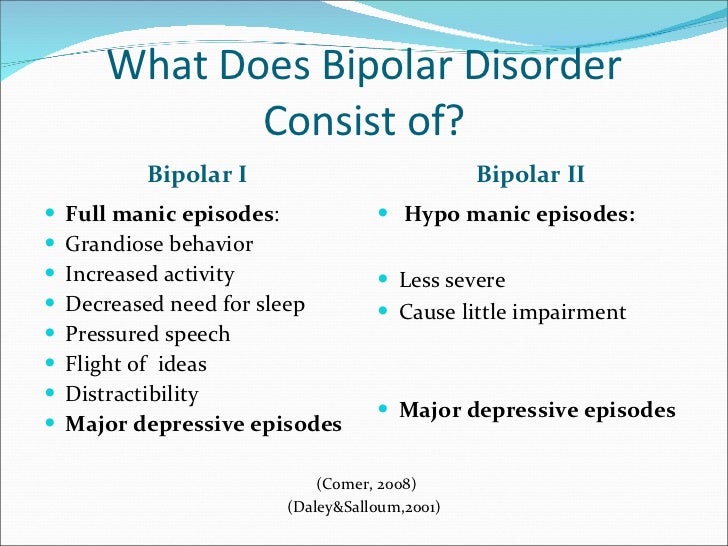 Improving our understanding of all of these issues depends on further research into these disorders as they appear in children and adolescents. Fortunately, some of this research is currently underway and holds the promise of better answers to these important questions in the future.
Improving our understanding of all of these issues depends on further research into these disorders as they appear in children and adolescents. Fortunately, some of this research is currently underway and holds the promise of better answers to these important questions in the future.
Bipolar disorder in children and adolescents
In adults, bipolar disorder commonly involves separate episodes of major depression, alternating with separate episodes of mania. In children mixed states (a mix of mania and depression) and rapid cycling (mood swings) may be much more common. This can make the diagnosis of bipolar disorder much more challenging in these age groups.
Many clinicians have observed that the symptoms of bipolar disorder appear to change as children develop, though these observations have not been confirmed by long-term studies. In younger children chronic irritability and mood instability without classic mood swings may predominate. These symptoms most closely resemble a mixed state of the disorder. In older children and adolescents, episodes including euphoria, grandiosity and paranoia may predominate. In all age groups hyperactivity, distractibility and pressured speech are seen. In general, the older the individual, the more the symptoms may resemble those seen in adults.
In older children and adolescents, episodes including euphoria, grandiosity and paranoia may predominate. In all age groups hyperactivity, distractibility and pressured speech are seen. In general, the older the individual, the more the symptoms may resemble those seen in adults.
Bipolar disorder and ADHD
As any parent of a child with ADHD has probably already noted, there is a significant overlap in the symptoms of mania, and to a lesser extent depression, and the symptoms of ADHD. ADHD, mania and depression may all involve inability to concentrate and problems with distractibility. Mania and ADHD may both involve hyperactivity and impulsivity. Though the symptom overlap is significant there are several factors that can help to distinguish these disorders.
ADHD in children usually does not involve mood symptoms such as depression and euphoria to the extent seen in bipolar disorder. ADHD symptoms usually first appear early in childhood while the onset of bipolar disorder appears to occur later in childhood or adolescence (4).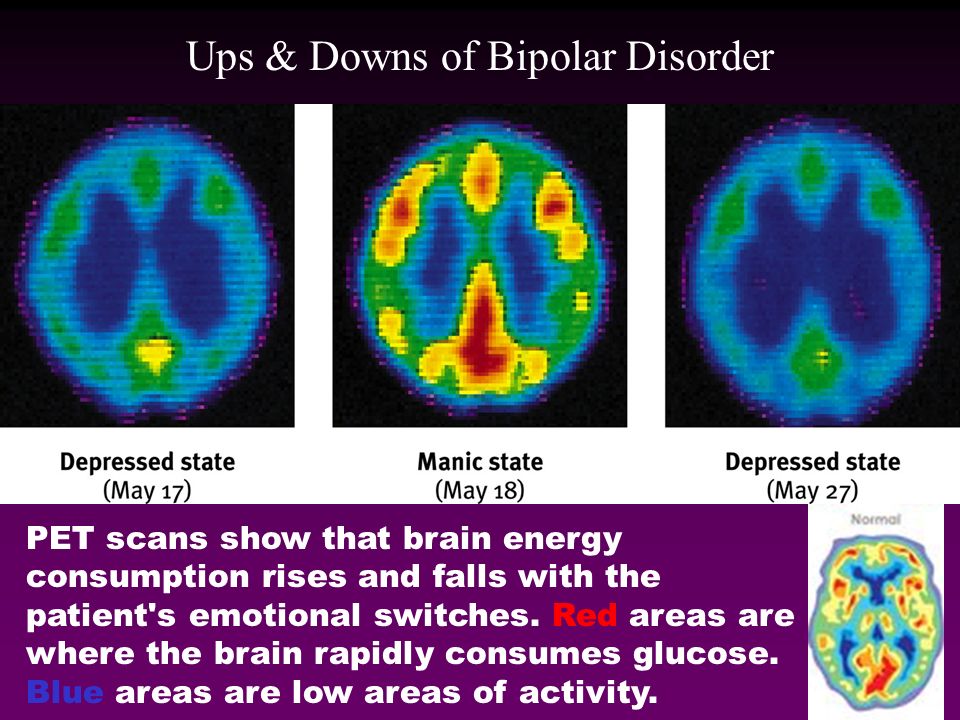 ADHD also usually involves normal sleep, at least once a child has settled down in bed and is ready for sleep. Mania, in contrast, involves decreased need for sleep with the individual still “raring to go” the next day despite little sleep. The family history can be helpful, as both disorders appear to run in families.
ADHD also usually involves normal sleep, at least once a child has settled down in bed and is ready for sleep. Mania, in contrast, involves decreased need for sleep with the individual still “raring to go” the next day despite little sleep. The family history can be helpful, as both disorders appear to run in families.
Depression and bipolar disorder
People who suffer from depression, including those who suffer from major depressive disorder, may also eventually exhibit symptoms of bipolar disorder. It is harder to tell the difference between depression and bipolar disorder in children than in adults. Children with depression more often appear irritable than sad. This presents another overlap with the irritability seen in bipolar disorder. Children and adolescents are also by their nature prone to some degree of unstable mood. Determining where this type of moodiness ends and bipolar disorder begins in a depressed young person can present a challenge. Looking for the presence of other symptoms of mania or elevated mood, including the presence of euphoria or grandiosity at some point, is important in making this diagnostic distinction.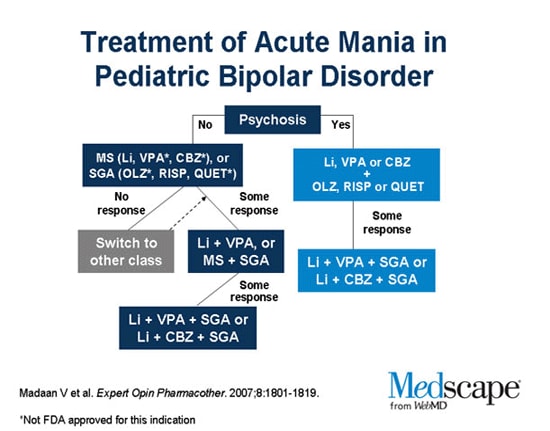
Further complicating the picture is the fact that both adults and younger people who initially exhibit symptoms only of depression may later develop bipolar disorder. The risk of depression turning into bipolar disorder is estimated at 10 percent or less in adults but appears to be as high as 20–40 percent in children and adolescents. Several risk factors for the eventual development of bipolar disorder in addition to early onset of depression have been identified, including psychosis, sudden onset, severely slowed or retarded movement, antidepressant-induced mania or elevated mood, and family history of bipolar disorder.
Treatment
Bipolar disorder is a serious disorder that can cause significant problems in school, the family, and the community. Untreated bipolar disorder can lead to hospitalization, drug abuse, accidents, or suicide. Parents who suspect that their child has bipolar disorder should find a child psychiatrist or psychologist who can evaluate the child.
The comprehensive treatment of bipolar disorder, like all other mental illnesses in children and adolescents, involves a multi-modal approach. Of course the first step in treatment is a comprehensive diagnostic evaluation performed by a child psychiatrist or psychologist with experience in the diagnosis of bipolar disorder in children and adolescents. Once the diagnosis is established ongoing treatment can begin. Medications form the foundation of this treatment. These medications have been found effective in adults and are currently being tested in children. At this point medication treatment of bipolar disorder involves the use of a mood stabilizer, which helps to prevent symptoms of mania while also hopefully improving symptoms of depression. In cases where depression remains a problem, the physician may consider prescribing an antidepressant as well as a mood stabilizer. Antidepressants in bipolar patients must be used cautiously, however, as they may cause a manic state.
Some clinicians are reluctant to prescribe stimulant medication for children who meet criteria for ADHD but who also have, or may have, bipolar disorder, because of a concern that bipolar symptoms might become worse.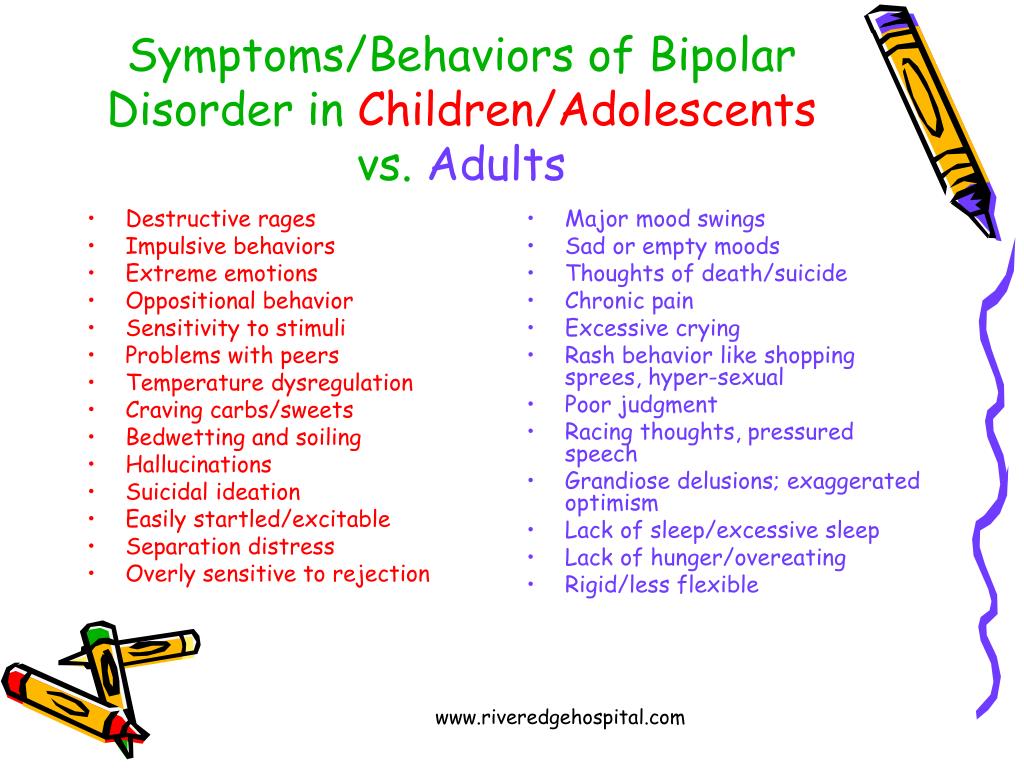 Currently, there is not evidence that this is the case, and research suggests that in general, children who have both ADHD and bipolar disorder can benefit from stimulant medication. However, it is important to be extremely careful in monitoring these children’s response to medication.
Currently, there is not evidence that this is the case, and research suggests that in general, children who have both ADHD and bipolar disorder can benefit from stimulant medication. However, it is important to be extremely careful in monitoring these children’s response to medication.
Other treatments are also very important in the management of this illness. They include measures to try to ensure regular sleep, which helps to keep mood stable. Therapy that educates the child about the importance of taking medication is also important. This is especially true for adolescents where any chronic illness can make it more difficult to achieve independence. Additionally, the family will benefit from comprehensive education and support as they help their child to deal with this very challenging illness. Academic interventions may also be needed (see Education). Finally, coexisting illnesses (other illnesses also present) including ADHD need to be treated.
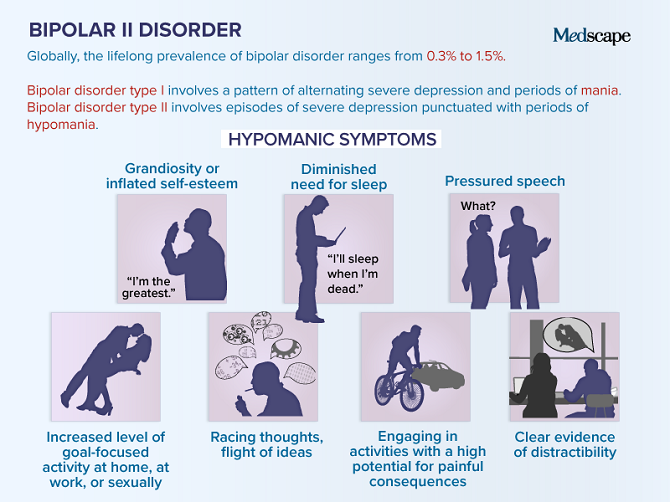
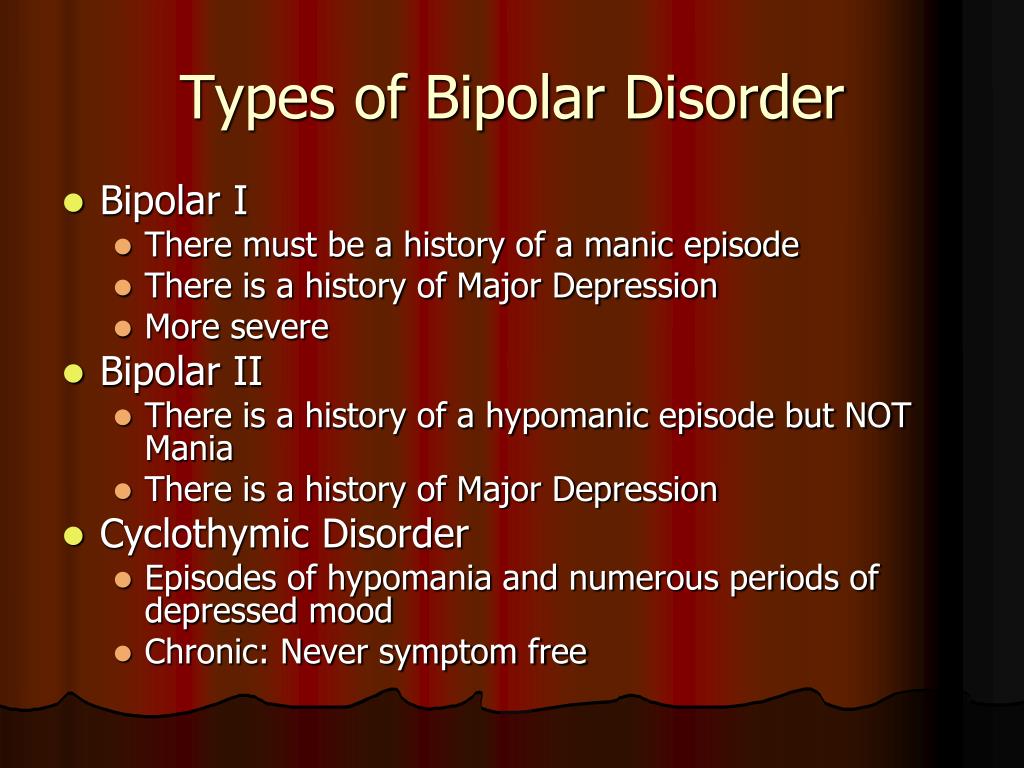
The “classic” combination of mania and major depressive episodes is now referred to as Bipolar I Disorder.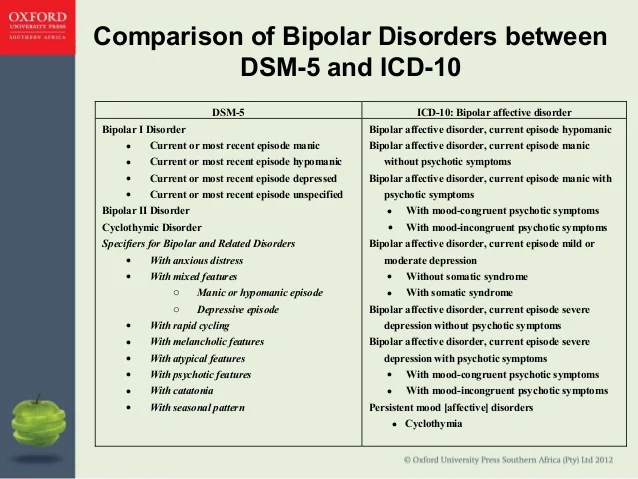 Major depressive episodes combined with a less severe expression of manic symptoms (called hypomania) is referred to as Bipolar II Disorder. Hypomania combined with a less pronounced and more longstanding form of depression (known as Dysthymia) is referred to as Cyclothymia. Symptoms of mania and a major depressive episode may also occur in combination simultaneously, this is called a Mixed State of Bipolar disorder. Finally, though episodes of mania and major depression classically occur in well-defined episodes, some people suffer from rapid swings between the two mood states that is referred to as Rapid Cycling. Bipolar I Disorder, Bipolar II Disorder, Cyclothymia, Mixed States and Rapid Cycling States are all considered to be bipolar spectrum disorders.
Major depressive episodes combined with a less severe expression of manic symptoms (called hypomania) is referred to as Bipolar II Disorder. Hypomania combined with a less pronounced and more longstanding form of depression (known as Dysthymia) is referred to as Cyclothymia. Symptoms of mania and a major depressive episode may also occur in combination simultaneously, this is called a Mixed State of Bipolar disorder. Finally, though episodes of mania and major depression classically occur in well-defined episodes, some people suffer from rapid swings between the two mood states that is referred to as Rapid Cycling. Bipolar I Disorder, Bipolar II Disorder, Cyclothymia, Mixed States and Rapid Cycling States are all considered to be bipolar spectrum disorders.
References
- Weller, E.B.; Weller, R.A.;and Fristad, M.A. (1995). “Bipolar disorder in children: misdiagnosis, underdiagnosis and future directions,” Journal of the American Academy of Child and Adolescent Psychiatry34:709–714, 1995.
- Weller, E.B.; Weller, R.A.; Danielyan, A.K. (2004) “Mood disorders in prepubertal children.” In Wiener, J.M., Dulcan, M.D. (editors). Textbook of child and adolescent psychiatry. Washington, D,C.: American Psychiatric Publishing: 418.
- Akiskal, H.S. (1995). “Developmental pathways to bipolarity: are juvenile onset depressions pre-bipolar “Journal of the American Academy of Child and Adolescent Psychiatry . 34:754–763.
- Strober, M.; and Carlson, G. (1982). “Bipolar illness in adolescents with major depression: clinical, genetic and psychopharmacologic predictors in a three-to-four year prospective follow-up investigation,” Archives of General Psychiatry 39:549–555, 1982.
- Carlson, G.A.; Loney, J.; Salisbury, H.; Kramer, J.R.; Arthur, C. (2000). “Stimulant treatment in young boys with symptoms suggesting childhood mania: A report from a longitudinal study.” Journal of Child and Adolescent Psychopharmacology 10(3): 175–184.
Bipolar Disorder in Children: Symptoms, Diagnosis & Treatment
Overview
What is bipolar disorder?
Bipolar disorder (formerly known as manic-depressive illness or manic depression) is a lifelong mood disorder and mental health condition that causes intense shifts in mood, energy levels, thinking patterns and behavior. These shifts can last for hours, days, weeks or months and interrupt your ability to carry out day-to-day tasks.
Most people are diagnosed with bipolar disorder in adolescence or adulthood, but the symptoms can appear earlier in childhood.
There are a few types of bipolar disorder, most of which involve experiencing manic and depressive episodes. However, people with bipolar disorder don’t always experience either manic episodes or depressive episodes. They also experience euthymia, which is a relatively stable mood state in which they are their usual self.
Mania is a condition in which you have a period of abnormally elevated, extreme changes in your mood, emotions, energy level and activity level. People with certain types of bipolar disorder can experience hypomania, which is a less severe form of mania.
People with certain types of bipolar disorder can experience hypomania, which is a less severe form of mania.
During a depressive episode, you experience a low or depressed mood and/or loss of interest in most activities, as well as many other symptoms of depression.
How does bipolar disorder affect children?
Bipolar disorder is different in children and teenagers than in adults. Adults with bipolar disorder often have clear episodes of mania or depression that last a week or longer. In children and teens, the phases may be less clear, and changes from one episode to the other may happen faster. For example, a child may exhibit periods of giddiness and silliness, anger outbursts, and unprovoked crying all in one day.
Bipolar disorder is different from the typical mood swings and ups and downs every child and teenager goes through. The mood changes in bipolar disorder are more extreme, often unprovoked, and also involve:
- Changes in sleep patterns.
- Changes in energy level.
- Issues with focus and the ability to think clearly.
- Bipolar disorder symptoms can make it hard for your child to perform well in school or to get along with friends and family members. Some children and teens with bipolar disorder may try to hurt themselves or attempt suicide.
How common is bipolar disorder in children?
Studies show that about 4% of people under the age of 18, including children as young as 5, have bipolar disorder.
To put this in perspective, here are the rates of the most common mental health conditions that affect children:
- 9.8% of children have attention-deficit/hyperactivity disorder (ADHD).
- 9.4% of children have an anxiety disorder.
- 4.4% of children have depression.
Symptoms and Causes
What are the symptoms of bipolar disorder in children?
To understand bipolar disorder, it's helpful to know how mental health providers talk about severe mood swings. Mood swings are often termed "mood episodes. " Manic episodes describe periods when a child feels overly excited and confident, and they have a lot of energy. These feelings can quickly give way to confusion, irritability and possibly rage.
" Manic episodes describe periods when a child feels overly excited and confident, and they have a lot of energy. These feelings can quickly give way to confusion, irritability and possibly rage.
Depressive episodes describe periods when a child feels very sad (depressed) and has low energy.
Children may not have clear-cut episodes. Instead, they may have "mixed" episodes and exhibit both manic and depressive symptoms. Some children may show "rapid cycling" where they shift quickly between mania or hypomania and depression — sometimes even within the same day.
Depressive, manic or mixed episodes, by definition, are a change in behavior that differs from your child’s baseline state (euthymia).
Signs and symptoms of manic episodes in children
Children with bipolar disorder are more likely to be irritable and prone to destructive outbursts during manic episodes than to be happy or euphoric like adults with bipolar disorder typically are.
During a manic episode, your child may:
- Be overly happy, hopeful and excited, which is often inconsistent with external events.
- Have bursts of energy and be very active.
- Have frequent tantrums or seem more irritable than usual.
- Be unusually silly compared to others their age.
- Be defiant and destructive and not follow rules as they usually do.
- Go for days with little or no sleep without feeling or acting tired.
- Be more impatient and restless than usual.
- Talk very fast, not allowing others to talk.
- Be distracted, have trouble concentrating and jump between different ideas.
- Believe they have many unrealistic or grandiose skills and powers and can do things other people can't do (such as believe that they’re in charge instead of adults).
- Seem overly interested or involved in pleasurable but risky activities, such as unprotected sex and drinking alcohol.
- Do risky or reckless things that show poor judgment.
Signs and symptoms of depressive episodes in children
During a depressive episode, your child may:
- Feel frequent and unprovoked sadness.
- Be uninterested in things they used to enjoy.
- Cry often.
- Be irritable.
- Have trouble falling asleep, wake up very early or sleep too much.
- Have low energy.
- Lose interest in friends or classmates and isolate themselves from social interaction.
- Be extremely sensitive to rejection or failure.
- Have trouble concentrating or remembering things.
- Have poor performance in school.
- Eat too little or too much.
- Say negative things about themselves.
- Talk or think about death and suicide.
- They may also mention or complain of physical symptoms, including:
- Headaches.
- Stomachaches.
- Muscle aches.
- Tiredness.
Teens may be less likely than adults to admit that they’re sad and depressed. If your child shows signs of suicidal thinking, call your child’s healthcare provider.
If you think your child is in crisis and needs immediate help, call 911 or the National Suicide Prevention Lifeline at 1‑800‑273‑TALK (8255). It’s confidential, free and available 24/7.
It’s confidential, free and available 24/7.
What causes bipolar disorder in children?
Scientists don’t yet know the exact cause of bipolar disorder.
But they believe there’s a strong genetic (inherited) component. More than two-thirds of people with bipolar disorder have at least one close biological relative with the condition. However, just because you have a biological relative with bipolar disorder, it doesn’t necessarily mean that you’ll also develop it.
Research also shows that trauma and stressful life events— such as the death of a family member or abuse — may increase the chances of developing bipolar disorder in people with a genetic risk of having the condition.
Some children with bipolar disorder may have physical changes in their brain, which may mean that some parts of their brain are more active or less active than in other children.
Scientists are currently performing research to determine the relationship that these factors have in bipolar disorder, how they may help prevent its onset and what role they may play in its treatment.
Diagnosis and Tests
How is bipolar disorder diagnosed in children?
To be diagnosed with bipolar disorder, your child must have experienced at least one episode of mania or hypomania (with or without a depressive episode).
To diagnose bipolar disorder, your child’s healthcare provider may use many tools, including:
- A physical examination.
- A thorough medical history, which will include asking about your child’s symptoms, lifetime history, experiences and family history.
- Medical tests, such as blood tests, to rule out other conditions that could be causing your child’s symptoms.
- A mental health evaluation. Your child’s provider may perform the evaluation, or they may refer your child to a mental health specialist, such as a psychologist or psychiatrist, to get one.
Providers can often diagnose bipolar disorder in children more accurately when they ask the children, their teachers and their caregivers to fill out questionnaires that ask about mood, energy levels and other factors.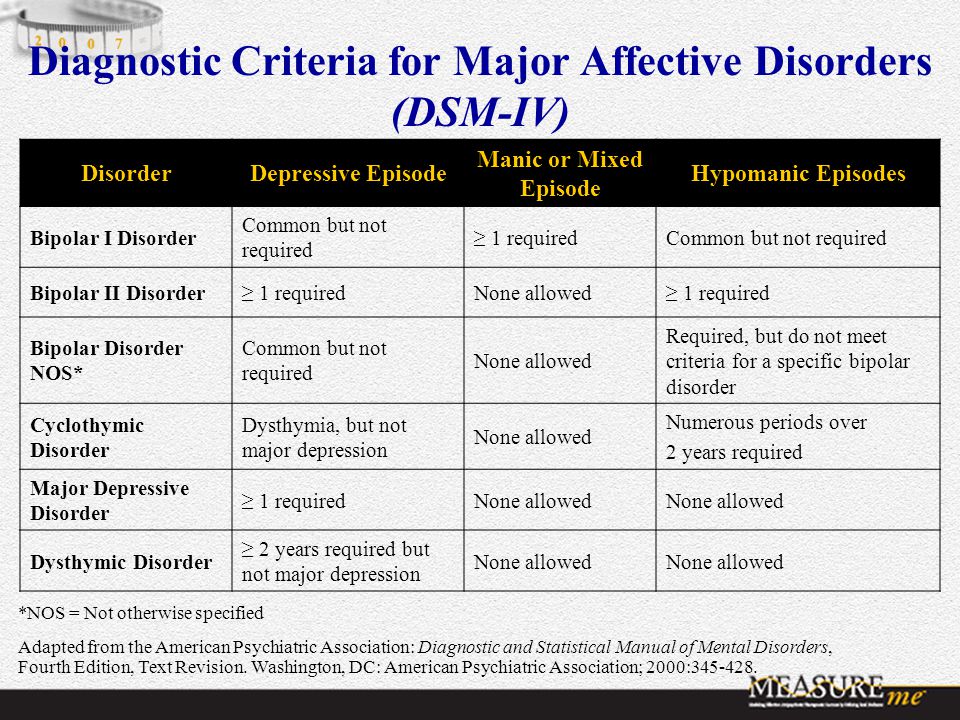
Signs and symptoms of bipolar disorder may overlap with symptoms of other disorders that are common in children and teens, including:
- Attention-deficit/hyperactivity disorder (ADHD).
- Disruptive mood regulation disorder.
- Oppositional defiant disorder.
- Conduct disorder.
- Major depression.
- Anxiety disorders.
- Because of this, diagnosing bipolar disorder in children can be complicated and requires a careful and thorough evaluation by a trained, experienced mental health professional.
Management and Treatment
How is bipolar disorder treated in children?
Over the past decade, mental health experts across psychology and psychiatry have helped refine the assessment and treatment of bipolar disorder among children and teens.
An effective treatment plan usually includes a combination of the following therapies:
- Psychotherapy (talk therapy).
- Medications.
- Helpful lifestyle habits, such as exercise, meditation and consistent routines.
- Other therapies.
Bipolar disorder is a lifelong condition, so treatment is a lifelong commitment. It can sometimes take several months to years before you, your child and their provider find a comprehensive treatment plan that works best for your child. Although this can be discouraging, it’s important for your child to continue treatment.
Psychotherapy for children with bipolar disorder
Psychotherapy, also called “talk therapy,” can be an effective part of the treatment plan for children with bipolar disorder.
Psychotherapy is a term for a variety of treatment techniques that aim to help your child identify and change troubling emotions, thoughts and behaviors. Working with a mental health professional, such as a psychologist or psychiatrist, can provide support, education and guidance to your child and your family.
Some types of therapy for bipolar disorder include:
- Psychoeducation: Psychoeducation is the way that mental health professionals teach people and their families about their mental health conditions.
- Family-focused therapy (FFT): This therapy is for people with bipolar disorder and their caregivers and family. During this treatment, together, your child and your family learn about bipolar disorder, communication improvement training and problem-solving skills training. It greatly helps family members to recognize symptoms of the condition and develop a plan for managing manic and depressive episodes.
- Chronotherapy: This therapy helps your child establish a steady and predictable sleep routine. Your child learns to go to bed at the same time and wake up at the same time every day.
- Interpersonal and social rhythm therapy (IPSRT): This therapy is designed to help your child improve their moods by understanding and working with their biological and social rhythms. IPSRT emphasizes techniques to improve medication adherence, manage stressful life events and reduce disruptions in social rhythms (day-to-day variability of habitual behaviors).
Medications for children with bipolar disorder
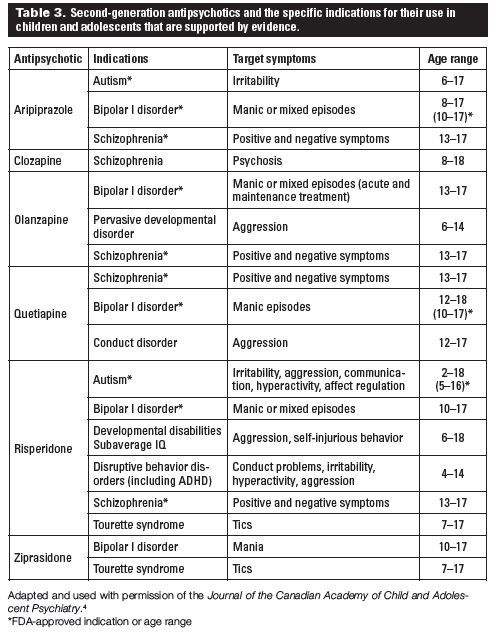
Mood stabilizers and antipsychotic (neuroleptic) drugs, which healthcare providers have used for decades to treat bipolar disorder in adults, are also effective in children with bipolar disorder.
Your child’s provider will work with you and them to select the best medicine. If your child also has attention-deficit/hyperactivity disorder (ADHD), their provider may prescribe medicines for it. But, in some cases, the medicines for ADHD can trigger manic symptoms or mood swings in children with bipolar disorder. Depression medications can also bring on bipolar symptoms in children.
Mood-stabilizing medications can help manage manic or hypomanic episodes. Types of mood stabilizers and their brand names include:
- Lithium (Eskalith®, Lithobid®, Lithonate®).
- Valproic acid (Depakene®).
- Divalproex sodium (Depakote®).
- Carbamazepine (Tegretol®, Equetro®).
- Lamotrigine (Lamictal®).
Providers often prescribe second-generation or “atypical” antipsychotics (neuroleptics) in combination with a mood stabilizer for people with bipolar disorder. These medications help with both manic and depressive episodes.
Only four of these drugs are FDA-approved to help treat bipolar depression, including:
- Cariprazine (Vraylar®).
- Lurasidone (Latuda®).
- Olanzapine-fluoxetine combination (Symbyax®).
- Quetiapine (Seroquel®).
What are the possible side effects of medications used to treat bipolar disorder in children?
Side effects of bipolar disorder medications are common and vary by medication.
It’s important to talk with your child’s healthcare provider about what you and your child can expect when taking certain medications. It’s also important to carefully assess your child for side effects and encourage them to tell you if they’re experiencing any. Report any negative side effects to their provider as soon as possible.
Your child should never stop taking their medication unless their provider tells them to do so. Abruptly stopping medication can cause severe side effects and trigger severe episodes.
The most common side effects of bipolar disorder medications include:
- Weight gain.
- Metabolic dysregulation, including abnormal lipid levels (dyslipidemia), high blood pressure (hypertension) and high blood sugar (hyperglycemia).
- Drowsiness.
- Akathisia — feelings of restlessness and agitation with a compelling need to move, rock or pace.
Lithium is one of the most common drugs used to treat bipolar disorder. Anything that lowers the level of sodium (salt) in your child’s body, such as switching to a low-sodium diet, heavy sweating, fever, vomiting or diarrhea may cause a toxic buildup of lithium in their body.
The following are signs of lithium toxicity (lithium overdose). Call your child’s provider immediately or go to the nearest emergency room if your child experiences:
- Blurred vision or double vision.

- Irregular pulse.
- Extremely fast or slow heartbeat.
- Difficulty breathing.
- Confusion and dizziness.
- Severe trembling or convulsions.
- Passing large amounts of pee.
- Uncontrolled eye movements.
- Unusual bruising or bleeding.
Prevention
Can bipolar disorder be prevented?
Unfortunately, there’s no known way to prevent bipolar disorder because scientists don’t know its exact cause.
But it’s important to know the signs and symptoms of bipolar disorder in children and to seek early intervention if your child is experiencing symptoms.
Outlook / Prognosis
What can I expect if my child has bipolar disorder?
Caring for a child or teenager with bipolar disorder can be stressful for parents, caregivers and families.
It’s important that you take care of yourself as well. Consider seeing a therapist or consult your healthcare provider about support groups. You may also want to consider family-focused therapy. During this type of therapy, together, your family learns about bipolar disorder, communication improvement training and problem-solving skills training.
During this type of therapy, together, your family learns about bipolar disorder, communication improvement training and problem-solving skills training.
Finding support and strategies for managing stress can help you, your child and your family.
What is the prognosis (outlook) for bipolar disorder in children?
The prognosis for bipolar disorder is often poor unless it’s properly treated.
If bipolar disorder goes untreated in children, it may make school, relationships and daily life very difficult. Children and teenagers with bipolar disorder are also at increased risk for:
- Delinquent behavior that results in incarceration.
- Misuse of alcohol and/or drugs.
- Suicide.
This is why it’s essential to seek medical care for your child if you think they may have bipolar disorder and to help them stay committed to treatment if they do have the condition.
Regular and continued use of medication can help reduce episodes of mania and depression.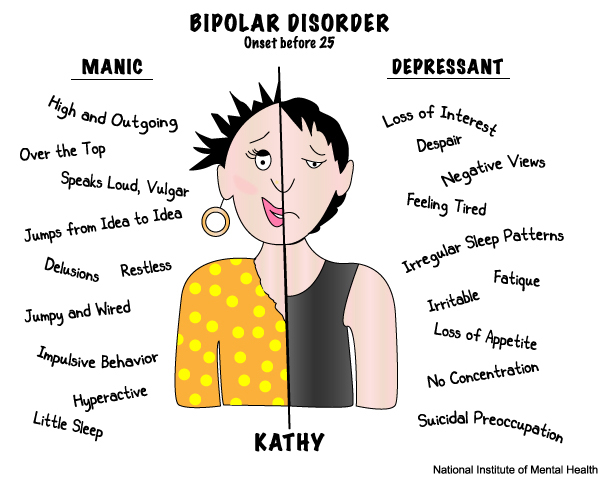 By knowing how to recognize the symptoms and triggers of these episodes, there’s a better chance for effective treatment and finding coping methods that may prevent long periods of illness, extended hospital stays and suicide.
By knowing how to recognize the symptoms and triggers of these episodes, there’s a better chance for effective treatment and finding coping methods that may prevent long periods of illness, extended hospital stays and suicide.
Living With
How can I help my child with bipolar disorder?
If your child or teen has bipolar disorder, here are some things you can do to help them:
- Support your child: Encourage them to talk about their thoughts and feelings and be a good listener. This helps your child realize that feelings and thoughts really do matter and that you always have and always will care for them.
- Be patient: Finding the proper treatment that works best for your child and seeing improvement in their symptoms takes time. Although this can be daunting, it’s important to stay committed to the process.
- Pay attention to your child’s moods: Be alert to any major changes in your child. Stay in touch with teachers, babysitters and other people in your child’s life to share information about their symptoms.
- Keep a symptom diary to track your child’s moods: This can help you and your child’s healthcare team better understand their triggers and determine the best treatment strategy.
- Maintain a consistent routine at home: Maintaining regular daily routines, especially sleep routines, have been shown to help stabilize the moods of people with bipolar disorder.
- Help your child learn to manage stress: Stress and anxiety can worsen mood symptoms in many people with bipolar disorder. It’s important to help your child manage their stress in a healthy way, such as with deep breathing exercises or relaxing activities.
- Help your child understand that treatment can make life better: Explain the benefits of treatment for bipolar disorder and make sure your child takes their prescribed medicines every day and attends their therapy sessions.
When should my child see their healthcare provider about bipolar disorder?
If your child or teenager has been diagnosed with bipolar disorder, they’ll need to see their healthcare team regularly throughout their life to make sure their treatment is working well. This team may include a:
This team may include a:
- Primary healthcare provider.
- Pediatric psychiatrist.
- Child psychologist or therapist.
- Pediatric neurologist.
When should I take my child to the ER?
If your child is experiencing any of the following situations, it’s essential to call 911 or get to the nearest emergency room:
- Thoughts of death or suicide.
- Thoughts or plans of hurting themselves or others.
- Experiencing hallucinations and delusions.
- Symptoms of lithium toxicity (overdose), such as severe nausea and vomiting, severe hand tremors, confusion and vision changes.
A note from Cleveland Clinic
It can be difficult and overwhelming to learn that your child has bipolar disorder. Know that the condition is treatable. Early identification, diagnosis and treatment can help your child reach their full potential. Be sure to reach out to family and friends for support. Your child’s healthcare provider is also available to answer any questions you may have.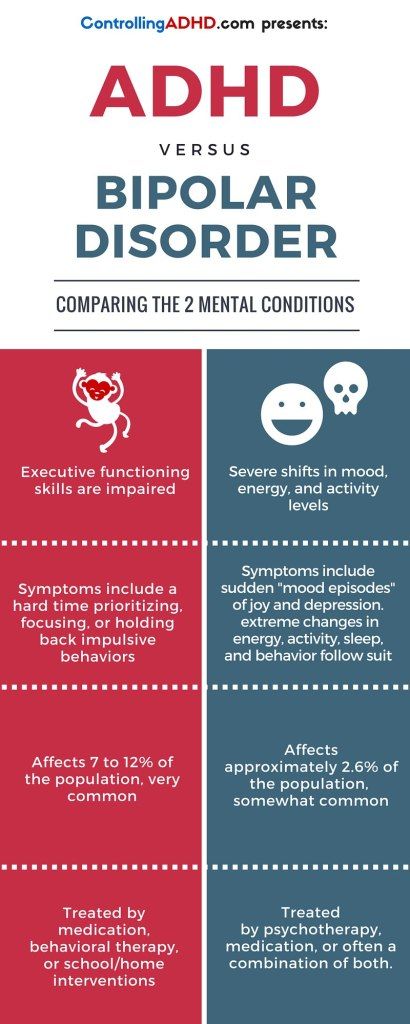
Bipolar affective disorder in children and adolescents - diagnosis and treatment at the Allianz Central Medical Health Center
2017-11-02
Mood swings happen to all people, and they are not at all uncommon in children and adolescents. These are the characteristics of growing up. However, it is necessary to separate the emotional lability inherent in adolescents from pathological manifestations, which are characterized, first of all, by abrupt changes not only in mood, but also in behavior, as well as energy levels, which clearly prevent the child or adolescent from functioning normally and maladjust him in everyday life. Such symptoms may be signs of bipolar affective disorder or, as this disease was previously called, manic-depressive psychosis. nine0003
Signs of bipolar affective disorder
Symptoms of bipolar disorder can be observed in children aged seven years and older, but in most cases, the onset of the disease coincides in time with a period of intense puberty.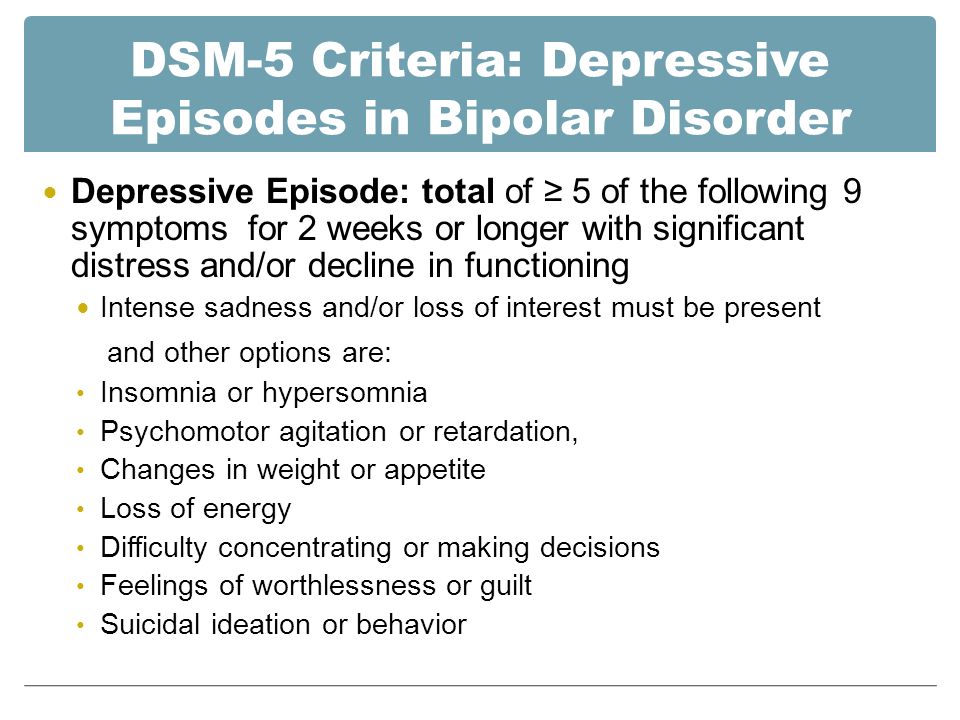 Particular attention should be paid to children and adolescents who are in a depressed state. In such cases, a thorough diagnosis is necessary to exclude bipolar disorder.
Particular attention should be paid to children and adolescents who are in a depressed state. In such cases, a thorough diagnosis is necessary to exclude bipolar disorder.
As a rule, young patients with bipolar affective disorder very quickly move from a phase of painfully elevated mood (mania or hypomania) to a pronounced decrease in the general emotional background (depression). Moreover, such differences contribute to the formation of general irritability during periods of normal state between these episodes. nine0003
Parents usually note the unpredictability of their children, but often attribute it to character traits and teenage behavior. The risk of developing bipolar disorder is increased in children suffering from hyperactivity, anxiety disorders and attention deficit.
When to call a specialist
Consultation with a psychiatrist-psychotherapist is necessary in the presence of the following symptoms, provided that they are of a permanent nature:
- Sudden mood swings from a state of euphoria to complete despondency or aggressiveness and irritability.
- Painfully high self-esteem.
- Changes and sudden changes in energy levels.
- Excessive, previously unusual activity.
- Change in speech habits: begins to talk a lot, speech is accelerated, sometimes slurred, quickly jumps from one topic to another, not taking into account the reaction of the interlocutor.
- Use of drugs or alcohol.
- Sexual activity.
- Depression, depressed mood, tearfulness.
- Closure, reduction of the circle of communication, narrowing of the circle of interests.
- Feeling of guilt, feeling of own uselessness and worthlessness.
- Suicidal thoughts or talk, self-destructive behavior.
It should be borne in mind that bipolar disorder responds well to correction. As a rule, the first diagnosis is made by a psychotherapist, to whom parents turn in case of alarming symptoms and painful changes in the behavior and habits of the child. In the future, it is also necessary to consult a psychiatrist and, in most cases, prescribe drug therapy. nine0003
nine0003
The help of a psychotherapist is required for a child or adolescent at all stages of treatment for bipolar disorder, but especially at the stage of rehabilitation.
The specialist will help the patient to adapt faster and select methods of therapy that reduce the risk of relapse.
Author: Specialist of the Alyans Mental Health Center
TsMZ "Alliance"
Bipolar disorder in adolescents - definition, causes, stages of development
According to the World Health Organization, bipolar disorder is in sixth place among the diseases that can provoke a disability in a patient. High incidence rates among adolescents lead to the need to find ways to solve this problem. The symptoms of bipolar disorder in adolescents are often explained by the characteristics of adolescence and are not considered as indicators of mental illness.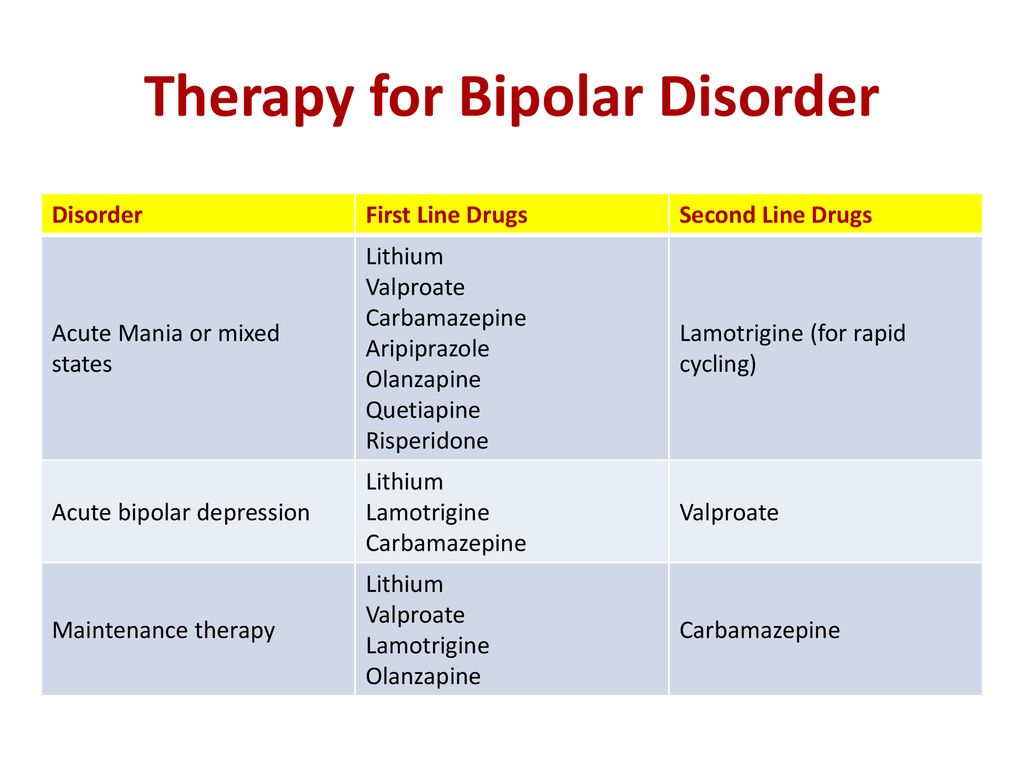 In this connection, the patient goes to the doctor when his condition worsens significantly, while the quality of life decreases. nine0003
In this connection, the patient goes to the doctor when his condition worsens significantly, while the quality of life decreases. nine0003
Disease definition
Bipolar disorder in adolescents is a disease characterized by alternating episodes of depression, mania, and an adequate state. These episodes can last from several weeks to several months.
In the ICD-10, bipolar affective disorder is coded F31 and is characterized as a disorder with two or more episodes in which the patient's activity level and mood are significantly impaired.
Bipolar personality disorder in adolescents was first described at the end of the 19th century by the German psychiatrist Emil Kraepelin, who defined it as manic-depressive psychosis. He considered the clinical picture of the disease and revealed a direct relationship between the increase in the number of depressive episodes and the age of the patient. The older a person is, the more often he experiences depression. nine0003
Young people from 15 to 25 years old are more susceptible to the disease. In children, the disease is rare, but in some cases it is at a younger age that the mechanism of mental changes is triggered. By gender, the ratio of cases is approximately equal.
In children, the disease is rare, but in some cases it is at a younger age that the mechanism of mental changes is triggered. By gender, the ratio of cases is approximately equal.
Bipolar disorder in children and adolescents usually begins with an episode of depression that lasts indefinitely. If the state enters the manic (hypomanic) phase, the adolescent experiences euphoria accompanied by feelings of happiness or irritability. The stronger the previous depressive phase, the more pronounced the mania. nine0003
Adolescent bipolar disorder is a disease that will periodically make itself felt in adulthood. But with the help of medical and psychotherapeutic methods, it is possible to achieve long periods of remission, contributing to a long, rich, fulfilling life for the patient.
Symptoms of bipolar disorder in adolescents
They are associated with the phases of the disease - depressive and manic. The disease can manifest itself in only one phase, or hypomanic manifestations can form. In some cases, the phases replace each other - then we are talking about a mixed type of disease. nine0003
In some cases, the phases replace each other - then we are talking about a mixed type of disease. nine0003
Despite the fact that the symptoms of bipolar disorder in adolescents from 14 to 17 years old have similar features, each case is individual. The number of phases, the frequency of their change and the duration differ in each case. Remission periods also take a different period of time and can last several years. At the end of the attack, mental health is restored and maintained until the next episode.
The main signs of bipolar disorder in adolescents are: nine0003
- Depressive episode of bipolar disorder. The main symptom of a depressive episode is pronounced depression, which occurs with the presence of psychoses and nervous disorders. The depressive state is characterized by a persistent clinical picture over a long period of time.
Symptoms of bipolar personality disorder in adolescents include the following conditions and phenomena:
- Sudden mood swings in the same tone (anxious and depressive thoughts are observed in the morning; by the evening the condition improves, but the anxiety does not leave the patient).
 nine0020
nine0020 - Loss of appetite and change in taste preferences (against the background of depression and anxiety, the patient refuses to eat or forgets to eat). Sometimes the opposite picture arises: appetite increases, temporary periods of sleep and wakefulness are disturbed, and the patient spends more time in a state of sleep.
- Physical sensation of feelings of melancholy and anxiety. Night sleep does not bring relief. The patient complains of being tired in the morning.
- Inhibited reaction to what is happening (the slowness of the flow of basic mental processes does not allow you to adequately respond to current affairs). nine0020
- Delusional thoughts and hallucinations may occur. There are feelings of guilt, fear of imminent danger.
A characteristic symptom of bipolar disorder in adolescent girls is an irregular menstrual cycle or no menstrual cycle at all. Girls experience a depressive episode more vividly, completely immersing themselves in frustration.
One of the serious symptoms of depression is the presence of suicidal thoughts, which lead to appropriate actions. When the risk of suicide increases, the patient is hospitalized in the hospital of the clinic. nine0003
Symptoms and signs of bipolar disorder in an adolescent manic episode vary in severity. It can be hypomania (mild mania) or mania with pronounced mental manifestations.
A manic episode manifests itself in the following states:
- The patient experiences an inexplicable feeling of joy, has fun and jokes for no reason. The elevated mood does not leave him for a long time. Excessive activity, megalomania, self-confidence and rightness push him to all sorts of "exploits". nine0020
- The desire to have time to do everything leads to a rush and the inability to focus on something specific. A teenager starts several things at the same time, but does not bring them to the end and forgets about what he did.
- Actions do not keep pace with the thoughts that arise at the speed of light in the head of the patient.
In the case of mild mania (hypomania), there is no pronounced social maladjustment, high spirits and activity do not interfere with existence and communication in society. nine0003
Mania is not always fun and joy. One of the variants of the manic syndrome is the manifestation of mania of anger. In this case, the patient experiences irritation, anger; picks on trifles to others; gets nervous if someone asks again or asks questions.
Symptoms of a mixed episode of bipolar affective disorder in adolescents include signs of bipolar disorder in adolescents 14, 15, 16 years of two episodes - depressive and manic. However, these episodes can last several weeks or hours. With a mixed type of disorder, the symptoms are most pronounced and lead to social maladaptation. nine0003
Relatives of potential mental health clinic patients are wondering how to tell if a teenager has bipolar disorder. Adolescence is the most difficult period in a person's life, because there are changes in the body, both physically and mentally. The first signs of bipolar disorder in adolescents are often attributed to the characteristics of adolescence, when emotional instability, mood swings, depression, youthful maximalism are not considered as borderline states of the psyche. nine0003
Adolescence is the most difficult period in a person's life, because there are changes in the body, both physically and mentally. The first signs of bipolar disorder in adolescents are often attributed to the characteristics of adolescence, when emotional instability, mood swings, depression, youthful maximalism are not considered as borderline states of the psyche. nine0003
Although already at 12 years old, adolescents can see signs of bipolar disorder. Features of adolescence leave their mark on the mood and attitude to life. But some moments in the behavior of a teenager should alert his inner circle.
Mental health professionals say that teens with bipolar disorder lose the ability to recognize the true emotions of others. Being in a state of depression, they perceive relatively neutral facial expressions in a negative way. They may feel that the other person is angry or afraid. Although in reality the interlocutor is calm and does not express any emotions. In addition, there are problems with memory, switching attention from one object to another. Symptoms of bipolar disorder in adolescents 18 years of age are pronounced, regardless of the episode in which the patient is. nine0003
Symptoms of bipolar disorder in adolescents 18 years of age are pronounced, regardless of the episode in which the patient is. nine0003
Causes of disease
Despite the keen interest in the phenomenon of bipolar disorder, experts do not have an exact explanation for the causes of bipolar disorder in adolescents. There is an opinion that the disease is inherited. Certain genes are believed to influence a person's predisposition to pathology, but they have not been identified at this time. The family history is taken into account. If this disorder is detected in one family member, this does not mean that the whole family is at risk. nine0003
Considering the cause-and-effect relationships in the formation of bipolar disorder in adolescents, experts pay attention to the associated risk factors: biological, emotional, social. Adolescents with other mental disorders are at risk: anxiety disorder, attention deficit hyperactivity disorder, a tendency to various kinds of addictions, etc.
Adolescents with other mental disorders are at risk: anxiety disorder, attention deficit hyperactivity disorder, a tendency to various kinds of addictions, etc.
Bipolar episodes can be initiated by any stressful situations, psychological trauma and addictions. However, in most cases, the disease is formed without any apparent causes and external triggers. nine0003
The pathogenesis of bipolar disorder in adolescents is not fully understood. The occurrence of the disease is due to a hereditary factor. It is believed that patients with bipolar disorder have abnormalities in the structure and functioning of the brain.
In the course of research, it was found that brain activity in depressive and manic phases differ. The occurrence of depressive states is associated with a violation of the functions of the system of inhibitory neurons of the brain, the "Sleep-wakefulness" cycle. The manic phase is associated with increased tone of the sympathetic nervous system, disruption of the pituitary gland and thyroid gland.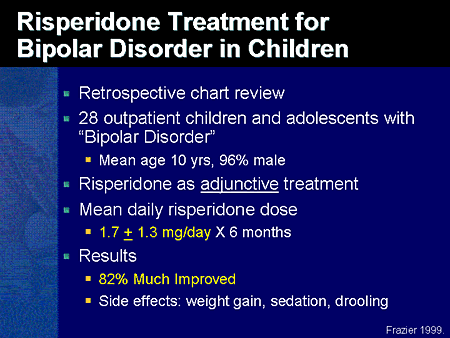 nine0003
nine0003
Developmental stages and classification of bipolar disorder
Episodes of bipolar disorder in adolescents have a characteristic clinical picture that develops over several stages.
A depressive episode includes 4 stages:
- Initial stage.
- The stage of increasing depression.
- stage of severe depression.
- Return to normal.
There are 5 stages in a manic (hypomanic) episode: nine0003
- Hypomania (growing depression).
- Mania (severe depression).
- phase peak.
- Relief of symptoms.
- Return to normal.
The classification of bipolar disorder in the ICD-10 bipolar affective disorder is indicated by the code F31.
Given the nature of the course of the disease, experts distinguish the following manifestation of the pathological process:
- bipolar course - the disease is characterized by a change in two phases (depressive and manic), between which there are periods of remission; nine0020
- continual course - there are no periods of remission between the phases of a depressive and manic disorder.
 One phase is immediately replaced by another.
One phase is immediately replaced by another. - monopolar course - the patient suffers from either manic or depressive manifestations. Most often, adolescents are overcome by depression, the symptoms of which are of a pronounced clinical nature.
Complications of the disease
Complications of adolescent bipolar disorder include an altered perception of reality, which leads to an intense increase in the frequency of suicidal thoughts and actions. Various kinds of addictions (drug, alcohol) that occur against the background of episodes of the disease exacerbate the symptoms. If there are concomitant diseases, the pathological process reaches critical indications. nine0003
The consequences of bipolar disorder in adolescents can significantly limit their normal functioning. The states of mania and depression affect the patient's relationship with others. Antisocial behavior is formed, as a result of which there are problems with the law. The patient can be dangerous both for himself and for other people.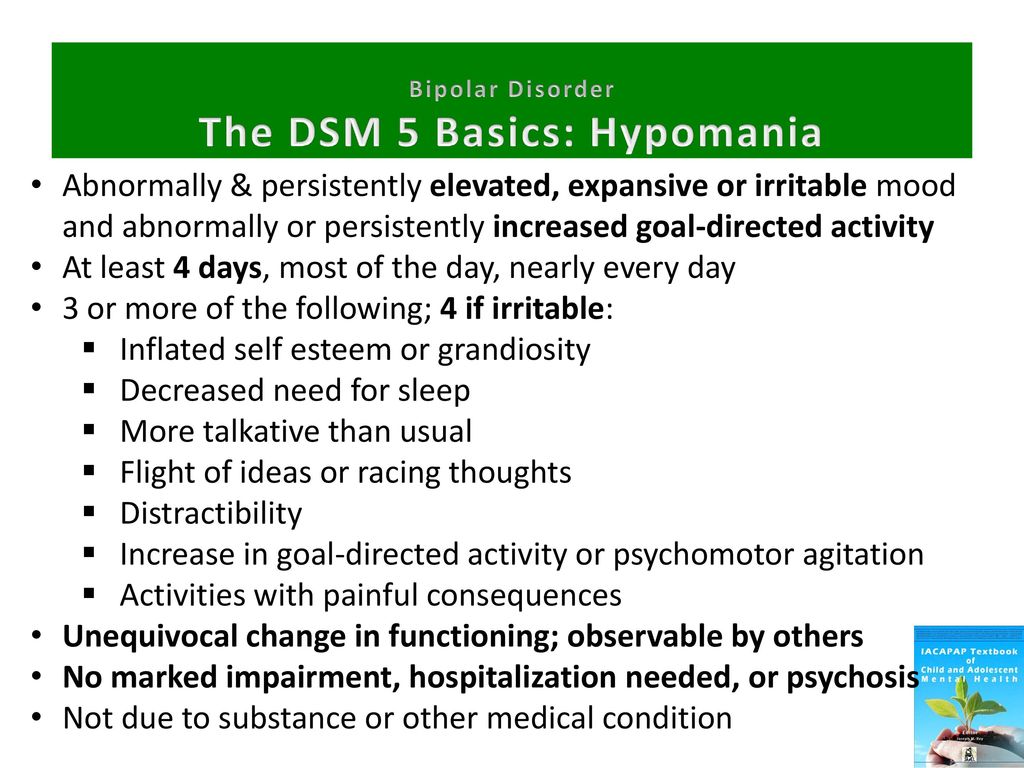
Extreme polar moods of the patient not only limit his life activity, but also interfere with the life of family members and close relatives. emotional instability, whether it be mania or depression, significantly change the daily lifestyle of the patient and his environment. The disease becomes a problem for the whole family, it affects the social, legal, material spheres of life. nine0003
Bipolar disorder does not go away on its own. If left untreated, the clinical picture worsens. Periods of emotional mood swings become longer and more severe.
In whatever episode of the disease a person is, his emotional state causes inconvenience to himself and others. Often relatives go to the doctor when a lot of time has passed since the first episode. Emotional instability, mood swings are usually attributed to the characteristics of adolescence. Prolonged lack of treatment leads to a worsening of the condition and an increase in the duration of depression and mania.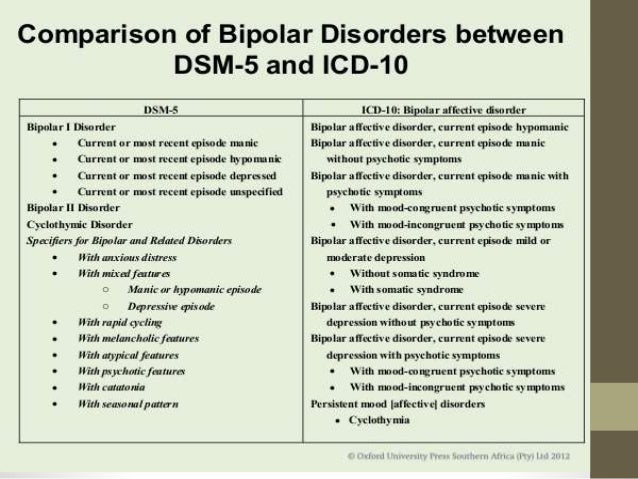 nine0003
nine0003
At the first signs of a pathological change in mood, which has a bipolar tonality, it is necessary to contact a specialist who treats mental disorders.
Diagnosis of bipolar disorder in adolescents
A feature of this disease is that there are no laboratory and instrumental diagnostic methods. How to determine bipolar disorder in adolescents if it is not possible to identify the pathology based on the results of tests and examinations? nine0003
When diagnosing bipolar disorder, special attention is paid to the symptoms of the disease. An informative diagnostic method is the collection of an anamnesis of the disease, in which the patient and his relatives or immediate environment participate.
Bipolar disorder must be differentiated from other pathological conditions: schizophrenia, anxiety and hyperkinetic disorders, addictions of various origins. In most cases, the diagnosis of the disease is difficult, since adolescents, due to age, are characterized by frequent mood swings and emotional instability. nine0003
nine0003
An accurate diagnosis can be made by a specialist in a specialized clinic dealing with the treatment of mental disorders. He knows how to diagnose bipolar disorder in a teenager, determine the type and stage of the disease.
Treatment of bipolar disorder in adolescents
The choice of treatments for bipolar disorder in adolescents depends on the severity of the clinical picture. It can be urgent (to relieve acute symptoms), ongoing (to consolidate the therapeutic effect) and supportive (to stabilize the patient's condition). nine0003
In the treatment of bipolar disorder in adolescents, medical and psychotherapeutic methods are used.
-
Medical treatment
-
Psychotherapy
Bipolar disorder in adolescents is an incurable disease. But with the help of drugs, success can be achieved in eliminating acute symptoms and restoring the social status of the patient.
Drug therapy in adolescents is similar to how bipolar disorder is treated in adults, but the young age of the patient must be taken into account. It is strictly forbidden to prescribe medicines on your own. Only a doctor who specializes in the treatment of mental disorders can pick them up. Depending on the progressive episode, the patient is prescribed different groups of drugs, such as antidepressants, tranquilizers, antipsychotics, mood stabilizers, anti-anxiety drugs. nine0003
It is strictly forbidden to prescribe medicines on your own. Only a doctor who specializes in the treatment of mental disorders can pick them up. Depending on the progressive episode, the patient is prescribed different groups of drugs, such as antidepressants, tranquilizers, antipsychotics, mood stabilizers, anti-anxiety drugs. nine0003
In psychotherapy, special methods have been developed to cope with the symptoms of the disease, as well as to prevent relapses:
- Cognitive-behavioral psychotherapy (based on the relationship between the patient and his parents to correct the patient's condition).
- Multi-family group psychoeducation along with individual family psychoeducation (determination of methods of drug treatment and strategies for solving emerging problems). nine0020
- Dialectical behavioral therapy (a series of classes to reduce anxiety, depression, the frequency of suicidal thoughts).
Psychotherapy is an effective method only if all the recommendations of specialists are followed. It is important to manage the symptoms of any episode of bipolar disorder, whether depressive or manic.
It is important to manage the symptoms of any episode of bipolar disorder, whether depressive or manic.
+7 (495) 121-48-31
Disease prevention
There is no specific prevention for bipolar disorder in adolescents. To minimize the occurrence of depressive, manic or mixed episodes, it is necessary to follow the doctor's recommendations. Supportive care to prevent symptoms is important. nine0003
To achieve long-term remissions, the participation of a specialist psychotherapist is necessary. The use of psychotherapeutic and psychosocial methods of treatment and rehabilitation, filling out self-control sheets to track the dynamics contribute to the improvement of the patient's condition.
Clinical recommendations for bipolar disorder in adolescents include not only adherence to medication and psychotherapeutic prescriptions. It is necessary to pay attention to the living conditions of a teenager, social factors that affect his emotional state. nine0003
References: