Angry panic attack
Anger attacks in patients with depression
. 1999;60 Suppl 15:21-4.
M Fava 1 , J F Rosenbaum
Affiliations
Affiliation
- 1 Outpatient Psychiatry Division, Massachusetts General Hospital, and Harvard Medical School, Boston 02114, USA.
- PMID: 10418810
M Fava et al. J Clin Psychiatry. 1999.
. 1999;60 Suppl 15:21-4.
Authors
M Fava 1 , J F Rosenbaum
Affiliation
- 1 Outpatient Psychiatry Division, Massachusetts General Hospital, and Harvard Medical School, Boston 02114, USA.
- PMID: 10418810
Abstract
Anger attacks are sudden intense spells of anger that resemble panic attacks but lack the predominant affects of fear and anxiety associated with panic attacks. They typically occur in situations in which an individual feels emotionally trapped and experiences outbursts of anger that are later described by the patient as being uncharacteristic and inappropriate to the situation at hand. Anger attacks consist of both behavioral and autonomic features, and various criteria and an Anger Attacks Questionnaire have been designed to identify the presence of these attacks. The prevalence of anger attacks in depressed patients is approximately 30% to 40%, and the attacks have disappeared in 53% to 71% of depressed patients treated with fluoxetine, sertraline, or imipramine. This article discusses the development of the concept of anger attacks, the presence of anger attacks in depression and other psychiatric disorders, and the current treatment of anger attacks.
This article discusses the development of the concept of anger attacks, the presence of anger attacks in depression and other psychiatric disorders, and the current treatment of anger attacks.
Similar articles
-
[Anger outbursts in unipolar depressive disorders].
Fava M. Fava M. Encephale. 1997 Jun;23 Spec No 3:39-42. Encephale. 1997. PMID: 9333559 Review. French.
-
Depression with anger attacks.
Fava M. Fava M. J Clin Psychiatry. 1998;59 Suppl 18:18-22. J Clin Psychiatry. 1998. PMID: 9840194 Review.
-
Anger attacks in depression.
Fava M, Rosenbaum JF.
 Fava M, et al. Depress Anxiety. 1998;8 Suppl 1:59-63. Depress Anxiety. 1998. PMID: 9809215 Review.
Fava M, et al. Depress Anxiety. 1998;8 Suppl 1:59-63. Depress Anxiety. 1998. PMID: 9809215 Review. -
A preliminary study on the efficacy of sertraline and imipramine on anger attacks in atypical depression and dysthymia.
Fava M, Nierenberg AA, Quitkin FM, Zisook S, Pearlstein T, Stone A, Rosenbaum JF. Fava M, et al. Psychopharmacol Bull. 1997;33(1):101-3. Psychopharmacol Bull. 1997. PMID: 9133758 Clinical Trial.
-
Anger attacks in depressed outpatients and their response to fluoxetine.
Fava M, Rosenbaum JF, McCarthy M, Pava J, Steingard R, Bless E. Fava M, et al. Psychopharmacol Bull. 1991;27(3):275-9. Psychopharmacol Bull. 1991. PMID: 1775598 Clinical Trial.
See all similar articles
Cited by
-
Validation of the Rage Attack Questionnaire-Revised (RAQ-R) in a Mixed Psychiatric Population.

Palm L, Haas M, Pisarenko A, Jakubovski E, Müller-Vahl KR. Palm L, et al. Front Psychiatry. 2021 Aug 18;12:724802. doi: 10.3389/fpsyt.2021.724802. eCollection 2021. Front Psychiatry. 2021. PMID: 34531770 Free PMC article.
-
How and Why Are Irritability and Depression Linked?
Vidal-Ribas P, Stringaris A. Vidal-Ribas P, et al. Child Adolesc Psychiatr Clin N Am. 2021 Apr;30(2):401-414. doi: 10.1016/j.chc.2020.10.009. Child Adolesc Psychiatr Clin N Am. 2021. PMID: 33743947 Free PMC article. Review.
-
Social impairment in relation to clinical symptoms in youth at high risk for bipolar disorder.
Weintraub MJ, Keenan-Miller D, Schneck CD, Forgey Borlik M, Suddath RL, Marvin SE, Singh MK, Chang KD, Miklowitz DJ.
 Weintraub MJ, et al. Early Interv Psychiatry. 2022 Jan;16(1):17-25. doi: 10.1111/eip.13124. Epub 2021 Feb 8. Early Interv Psychiatry. 2022. PMID: 33559355 Free PMC article.
Weintraub MJ, et al. Early Interv Psychiatry. 2022 Jan;16(1):17-25. doi: 10.1111/eip.13124. Epub 2021 Feb 8. Early Interv Psychiatry. 2022. PMID: 33559355 Free PMC article. -
Anger-Related Characteristics According to Chronotypes in Bipolar or Depressive Disorders.
Kang TU, Moon E, Choi Y, Suh H, Park JM, Lee BD, Lee YM, Jeong HJ, Kim SY, Lee K, Lim HJ, Yoon M. Kang TU, et al. Psychiatry Investig. 2020 Sep;17(9):880-888. doi: 10.30773/pi.2019.0326. Epub 2020 Sep 9. Psychiatry Investig. 2020. PMID: 32894930 Free PMC article.
-
Forgiving Adolescents: Far From Depression, Close to Well-Being.
Barcaccia B, Pallini S, Pozza A, Milioni M, Baiocco R, Mancini F, Vecchio GM. Barcaccia B, et al. Front Psychol.
 2019 Jul 24;10:1725. doi: 10.3389/fpsyg.2019.01725. eCollection 2019. Front Psychol. 2019. PMID: 31396140 Free PMC article.
2019 Jul 24;10:1725. doi: 10.3389/fpsyg.2019.01725. eCollection 2019. Front Psychol. 2019. PMID: 31396140 Free PMC article.
See all "Cited by" articles
MeSH terms
Substances
Rage Attacks | Cedars-Sinai
ABOUT DIAGNOSIS TREATMENT
Overview
Rage attacks are sudden, out-of-control bursts of anger. These explosive outbursts can start without warning. They may also seem to be out of proportion to what triggered the episode.
Rage attacks are different than tantrums. Tantrums are goal-oriented with the intent of getting an observer to do what the person wants. Rage attacks are more about the release of pent up tension than about achieving a specific goal.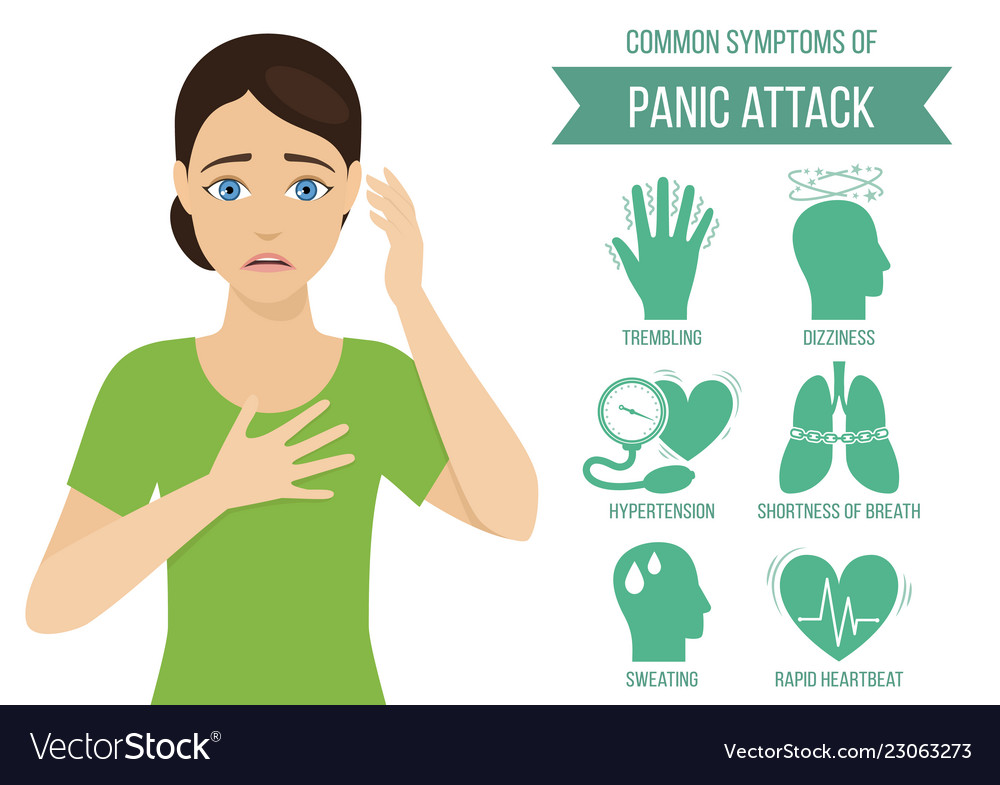
In the past, rage attacks were thought to be related to epilepsy or Tourette syndrome. This is now understood to be false.
Symptoms
Rage attacks may seem to begin without warning. However, little signs may be seen, including:
- Increased stressed
- Increased agitation
- Anxiety
When a rage attack happens, symptoms may include:
- Yelling or shouting
- Intense anger
- Physical aggression
Causes and Risk Factors
Rage attacks are sometimes incorrectly linked with epilepsy or Tourette syndrome. In very rare cases, limbic seizures can be linked to out-of-control behavior. However, this is uncommon.
The cause of rage attacks is unknown.
Some children or teenagers may have rage attacks only at home and not at school. Others may have the attacks at school.
Rage attacks can be triggered by stressors such as:
- Social pressure
- School work
Diagnosis
If the patient has symptoms similar to a seizure, the doctor will often test the patient for epilepsy. The most useful test in confirming epilepsy is an electroencephalogram (EEG). This test records electrical activity in the brain. It can show abnormal spikes or waves in electrical activity patterns. Different types of epilepsy can be identified with these patterns.
The most useful test in confirming epilepsy is an electroencephalogram (EEG). This test records electrical activity in the brain. It can show abnormal spikes or waves in electrical activity patterns. Different types of epilepsy can be identified with these patterns.
A patient with rage attacks that are unrelated to epilepsy will not show unusual electrical activity in the brain on the EEG.
Magnetic resonance imaging (MRI) and computed tomography (CT) scans may be used to look for epilepsy as well. However, these tests are not very helpful for rage attacks.
If the doctor suspects rage attacks, the patient will be referred to a psychologist for further diagnosis and treatment.
Treatment
Psychotherapy is the most common treatment for rage attacks. This may include cognitive behavioral therapy (CBT). CBT examines thoughts and their links to feelings and behaviors. CBT and other psychotherapies take several months to work. It is important that the patient continue their treatment plan during this time.
Rage attacks do not respond to anti-seizure medications. However, medications for depression or anxiety may be used as part of the treatment plan.
© 2000-2022 The StayWell Company, LLC. All rights reserved. This information is not intended as a substitute for professional medical care. Always follow your healthcare professional's instructions.
How to distinguish a panic attack from a heart attack? An expert tells
Back to list
10/18/2022
Severe stress, depression or exhaustion of the body can cause panic attacks.
This is a state of severe anxiety or panic fear, which is accompanied by a rapid heartbeat and a feeling of suffocation. How to distinguish a panic attack from a heart attack? What to do in case of a panic attack? Which doctor should I contact for help? - 9 told about it0010 Irina Golotina, general practitioner at INVITRO-Rostov-on-Don LLC.
What are the similar symptoms and differences between a panic attack and a heart attack?
Panic attack and heart attack have similar symptoms such as rapid heart rate, shortness of breath, sweating, chest pain. However, in the case of a panic attack, the symptoms may last for about 20 minutes and then disappear, while the symptoms of a heart attack do not go away until medical attention is received. In addition, patients feel warning symptoms before a heart attack, usually a few days before, and the heart attack itself most often occurs during physical activity. Panic attacks occur regardless of physical activity.
However, in the case of a panic attack, the symptoms may last for about 20 minutes and then disappear, while the symptoms of a heart attack do not go away until medical attention is received. In addition, patients feel warning symptoms before a heart attack, usually a few days before, and the heart attack itself most often occurs during physical activity. Panic attacks occur regardless of physical activity.
If a young person with no risk factors has chest pain, the chance of a heart attack is very low, but chest pain in a 50-year-old man who smokes for many years and has diabetes most likely signals a heart attack, and that he needs urgent medical attention.
The main risk factors for panic attacks are mental health, but in the case of a heart attack, the main role is played by the physical condition of a person, where the main indicator is age, cholesterol, body weight, blood pressure and other factors.
The nature of the pain may determine the type of attack it accompanies.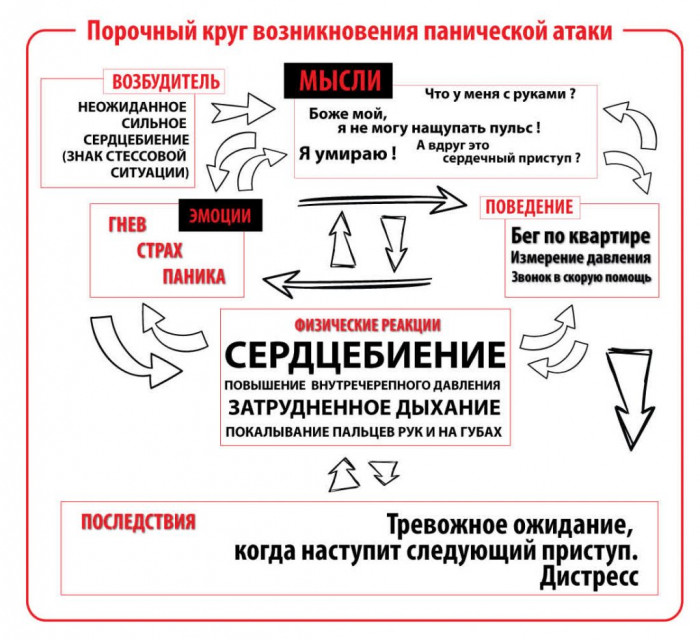 Sharp pain behind the sternum or pain concentrated in one small area is associated with a panic attack. This pain is stabbing in nature, and it is also short-lived and lasts about 5-10 seconds. During a heart attack, they complain of pressing, squeezing chest pains that spread to the left arm, can radiate to the right arm, neck, interscapular region, that is, they are most often associated precisely with physical exertion - physical and emotional overstrain.
Sharp pain behind the sternum or pain concentrated in one small area is associated with a panic attack. This pain is stabbing in nature, and it is also short-lived and lasts about 5-10 seconds. During a heart attack, they complain of pressing, squeezing chest pains that spread to the left arm, can radiate to the right arm, neck, interscapular region, that is, they are most often associated precisely with physical exertion - physical and emotional overstrain.
What to do if a panic attack occurs?
If you have had a panic attack, first of all pay attention to your bodily condition: you need to focus on breathing: breathe with your stomach, focusing on exhalation, try to find your body, realize its presence. To do this, you need to stand on both legs, “ground yourself” - imagine that fear goes through you into the ground, like an electric current, grab onto something or start shaking your hands, shaking off the tense state. If there is someone nearby, then it is better to tell him about it, that you are experiencing a panic attack and you need help. You can try to verbalize your feelings: say each sensation out loud, tell others that you are afraid. By voicing our fear, we reduce our anxiety.
You can try to verbalize your feelings: say each sensation out loud, tell others that you are afraid. By voicing our fear, we reduce our anxiety.
Which specialist should I contact?
Panic attacks should be treated by a psychotherapist who has a medical background. The doctor will help you choose a therapy, help a person and tell you about methods that you can independently use to relieve a panic attack. Self-help methods are physiological and psychological. If these methods do not help, the doctor prescribes medication.
To clarify this disease, the doctor can refer to a cardiologist to rule out pathologies from the cardiovascular system, to an endocrinologist to rule out thyroid diseases, a pulmonologist to rule out respiratory diseases.
Heart attack and panic attack: how to tell the difference?
The difference between a heart attack and a panic attack worries many people. It is especially acute in persons who, with persistent periodicity, experience discomfort in the chest, increased sweating, dizziness, shortness of breath and trembling.
Medical examination is the only way to determine the type of attack, since it is difficult to identify a person's condition by subjective indicators. However, understanding the symptoms and risk factors can point to the root of the problem.
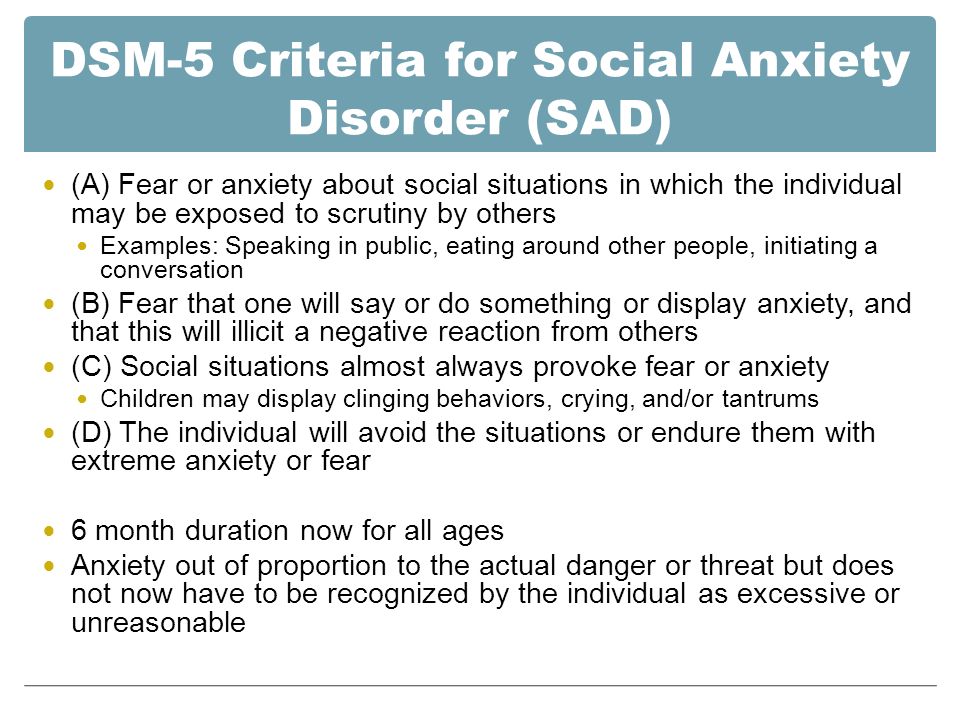
Panic attacks are a characteristic manifestation of panic-type disorders, but they can also be associated with other psychiatric conditions such as obsessive-compulsive disorder or social anxiety disorder.
The main risk factor for panic attacks is mental health, and in the case of heart attacks, physical health plays a large role. Among the main indicators: age, cholesterol level, body weight, blood pressure level, diet, etc.
Many doctors note that the nature of the pain can help determine the type of attack it accompanies. Sharp pain behind the sternum or pain concentrated in one small area is associated with panic attacks. This pain is stabbing in nature and usually lasts 5-10 seconds.
According to Dr. MaryAnn McLaughlin, cardiologist at Mount Sinai Hospital, USA, patients with a heart attack in most cases report a feeling of tightness in the chest rather than pain. This sensation is comparable to the sensation that occurs when wearing a tight bra or as if something is constricting in the chest.
MaryAnn McLaughlin, cardiologist at Mount Sinai Hospital, USA, patients with a heart attack in most cases report a feeling of tightness in the chest rather than pain. This sensation is comparable to the sensation that occurs when wearing a tight bra or as if something is constricting in the chest.
"There are certain types of heart attacks that are accompanied by a feeling of intense pain, but in general they begin with a feeling of squeezing, squeezing, which can spread towards the arms," explained M. McLaughlin.
The duration of the attack is also one of the key differences. Typically, panic attacks last up to 10 minutes, and heart attacks can usually last longer. If a person experiences the above symptoms for more than 5 minutes, seek immediate medical attention.
There are some studies that indicate that heart attacks are often accompanied by intense physical exertion or feelings of anger or frustration. For example, if an older person is not used to exercise, they may be at risk of having a heart attack after exercising.