Adhd relationship problems cheating
Healthy Relationships & ADHD: Happy Marriage How To
You wonder whether you’ll ever be able to settle down in a relationship, afraid that no one will ever let you be yourself with adult ADHD.
You tell yourself, Listen, listen, just listen, when talking with loved ones.
You try to be patient with a partner who seems to move in slow motion compared to your own faster tempo. You think, “Why do I always have to slow down? Why doesn’t anyone try, just for one day, to keep up with me?”
Your need for action and stimulation isn’t a character defect, it’s just a difference. ADHD is not a disorder that has to be hidden. If you can help your partner see the world from your point of view, you’re on your way to a fulfilling relationship.
The Gifts of ADHD
Impatience, inattention, and fidgeting — all symptoms of ADHD — are not crimes.
With these “deficits” come a lively mind and a life of fun and excitement. You have a lot to offer your spouse and children using your own personal style. If you can articulate — to yourself and others — how your ADHD is a gift, it won’t rob you of your vitality and life. To build a strong relationship, advocate for your gifts.
You won’t last in a relationship in which your ADHD symptoms are summed up as bad behavior. When someone tells you there’s something wrong with you, it hurts. Your partner calling you a “spazz,” or saying you need to “chill” at every turn, can take a serious toll. Let your partner know that such negativity is harmful. Tell him that it hurts to be told there’s something wrong with who you are. Such an admission can build intimacy between the two of you. If you try to cover up the hurt, it will lead to resentment that will prevent you from connecting with your spouse.
If you believe that you shouldn’t feel hurt — or, worse, that you deserve your partner’s criticisms — it is likely you’ll eventually want to end the relationship. Being stuck in reform school is a recipe for resentment.
[Get This Free Download: Manage ADHD’s Impact on Your Relationship]
Because adults with ADHD constantly crave new experiences, maintaining a long-term relationship can be a struggle, even without the burden of criticism.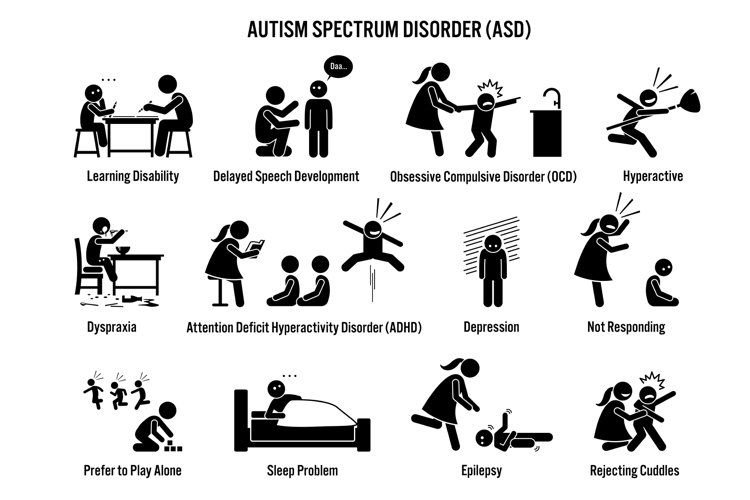 If resentment builds, an their need for stimulation is likely to create the impulse to find another partner. But if you educate your partner about your condition — and its gifts — he won’t be so critical. Try using these statements to advocate for yourself and to show your loved one what you are doing right:
If resentment builds, an their need for stimulation is likely to create the impulse to find another partner. But if you educate your partner about your condition — and its gifts — he won’t be so critical. Try using these statements to advocate for yourself and to show your loved one what you are doing right:
“It’s true I was having trouble listening, but I was keying in to your emotions.” “You’re right: I can’t sit still with the kids, but I can be lots of fun.” “I can’t be as patient as I would like, but I keep our social life hopping.”
Once your spouse understands ADHD and appreciates your strengths, it doesn’t mean that you won’t have problems to solve. Working through them, using the strategies below, will dramatically increase your odds of having a loving relationship.
Find Common Interests
Doing things together as a couple sounds easy, but adults with ADHD often lack patience for activities that a spouse enjoys. Anything that is slow or requires attention to detail can feel like torture to some adults with ADHD: For instance, your partner asks you to play backgammon, but you’d rather pluck out your eyelashes than concentrate on its rules. Or your partner asks you to join him to watch a foreign-language film, and you would rather see an action flick. Although such differences seem tough to resolve, there are solutions (see “Bond with Your Spouse,” below).
Or your partner asks you to join him to watch a foreign-language film, and you would rather see an action flick. Although such differences seem tough to resolve, there are solutions (see “Bond with Your Spouse,” below).
[Click to Read: “What I Love About My Wife with ADHD”]
Instead of letting backgammon or movies separate you and your spouse, show respect for his passion, while honoring your own interests. How? Give your partner a backgammon set, a book on backgammon strategy, or a night off from family duties to play the game with others.
While you may never share your lover’s enjoyment of board games, you can find activities that make you both happy. If you and he enjoy Italian food, say, come up with activities planned around that interest. Try different Italian restaurants, take a trip to Italy, read cookbooks, or collect Italian wines.
If you compromise yourself, chances are, your relationship will fail. This doesn’t mean that your partner should always be ready to meet your needs. It means that you shouldn’t consistently defer to the other person.
It means that you shouldn’t consistently defer to the other person.
Exercise 1: Bond with Your Spouse
Don’t fight with your partner over competing interests. Focus your attention, instead, on interests that you share. Here’s how:
- Each of you should compile a list of 100 interests — intellectual topics, sports events, foods, anything that piques your interest. Nothing is too lowbrow or highbrow to go on your lists.
- Review the lists to identify overlapping interests. Create a new list from these and rank them in order of how much each of you likes them.
- For each of your top five shared interests, come up with activities that the two of you would enjoy. If you both like classical music, you could visit music stores together, attend concerts, go on drives while listening to CDs, share downloads with each other, take singing classes, start a classical music blog, or read books on favorite artists.
- Now slot some of these activities into your weekly schedule.
Listen to Your Spouse
Not being listened to is the major complaint of those in intimate relationships with adults who have ADHD. For many, listening to others is hard. In some cases, you may actually be listening, but you look so spaced-out that others think you are not.
Although those with ADHD can’t stand it when others repeat themselves, you may unwittingly be causing them to do so. If you’re impatient and tend to interrupt, your partner may feel he’s not being heard. So he repeats himself, which causes you to tune out even more. Remember: When others feel they have been heard, they will stop repeating themselves. For people in long-term relationships, good listening can break a dysfunctional pattern that has gone on for years — perhaps for decades.
Exercise 2: Listen and Learn
Sometimes your conversations seem to go on forever. That’s because your sense of time is distorted by feelings of restlessness. So you interrupt your spouse or change the topic. This listening exercise will make your partner feel that he has been heard.
This listening exercise will make your partner feel that he has been heard.
- Figure out the time of day when you typically clash with your spouse over not listening. It may be just after he gets home from work and wants to talk about his stressful day.
- Sit down with him and let him talk. Do not interrupt for five minutes. If you find yourself getting distracted or looking at the clock, put your attention back on the conversation.
- At the end of five minutes, summarize what you heard. You might say, “Wow, it sounds like you had a really hectic day. The lousy commute, the awful meeting, and then your boss wanted the proposal done by the end of the day. At least you got to stop at the gym on the way home.” Of course, you can listen for more than five minutes. I have coached people to look like they’re listening-make eye contact and lean toward the person, even if you’re not absorbing every word. If you can’t listen much beyond five minutes, then give yourself permission to do something you want to do.
 You may say, “Now that you’re home, would you mind hanging out with Robbie for a bit while I go for a run?”
You may say, “Now that you’re home, would you mind hanging out with Robbie for a bit while I go for a run?”
If you’re like most adults with ADHD, your partner will be shocked and pleased that you have listened to him for a full five minutes.
Show Commitment
The main symptoms of ADHD-impulsiveness and the need for constant stimulation and excitement-can enhance or threaten relationships. Because adults with ADHD are impatient and easily bored, adventurous sexual activities are highly stimulating to them. Attraction to the new and different can cause you to find it difficult to stay monogamous. Adults with ADHD are also usually emotionally uninhibited, which can be attractive to others. This can lead to infidelity (see “Tame Temptation,” below).
The upside is that, once an adult with ADHD makes a commitment, life won’t be boring for his or her spouse. Their creativity will keep things lively, both in the bedroom and in social and recreational activities. I talked with an adult with ADHD who had found the woman whom he wanted to spend the rest of his life with. While he loved her, he couldn’t make a commitment. She was afraid that he was interested in other women. This hurt their relationship and put him on edge. He realized that committing to his lover would lead to a happy marriage.
I talked with an adult with ADHD who had found the woman whom he wanted to spend the rest of his life with. While he loved her, he couldn’t make a commitment. She was afraid that he was interested in other women. This hurt their relationship and put him on edge. He realized that committing to his lover would lead to a happy marriage.
Exercise 3: Tame Temptation
Impatience and impulsivity cause many relationship problems for adults with ADHD. Indeed, temptation sometimes overrides longer-term needs and desires. The following activity will you help weigh your choices.
- Imagine you are at a party celebrating your 25th wedding anniversary. Where would it be held? Who would be there? What gift would you give your spouse?
- Is the person you are now with the one you want to be with at your anniversary? Or do you want to be there with someone else? How will you feel, on your 25th wedding anniversary, about the person who may now be causing you to consider cheating on your partner? How would indulging your temptations make you feel on that day in the future? Would it be worth it?
- If you feel that cheating might be worth it, make a list of 10 people you have been attracted to in the last 10 years.
 Write down your feelings about each of them, and whether or not you acted on your feelings. Review the list. What does it tell you about your feelings of sexual attraction? Can you see a difference between the person you want in your life for the long haul and those you don’t? If cheating on your partner still seems like a good idea, you may want to consult a marriage counselor to help you figure out how to move forward.
Write down your feelings about each of them, and whether or not you acted on your feelings. Review the list. What does it tell you about your feelings of sexual attraction? Can you see a difference between the person you want in your life for the long haul and those you don’t? If cheating on your partner still seems like a good idea, you may want to consult a marriage counselor to help you figure out how to move forward.
[Read This Next: “An Open Letter to My Husband”]
Parenting Advice for Adults with ADHD
ADHD traits can not only threaten a marriage, but also get in the way of bonding with your child. For starters, you may not be able to sit still long enough to play games designed for young children. While most adults have difficulty with boring games, the need for stimulation in adults with ADHD makes this task impossible.
Before you blame yourself or your impatience, realize that you can spend time with your children doing activities that also interest you. Make a list of parenting jobs that you enjoy doing. They could be everything from sports coach and nutritionist to event planner and interior designer. Keep yourself alive as a parent by spending more time on these tasks. And remember to let your love and caring shine through, whether you’re engaged in a favorite activity or not.
Make a list of parenting jobs that you enjoy doing. They could be everything from sports coach and nutritionist to event planner and interior designer. Keep yourself alive as a parent by spending more time on these tasks. And remember to let your love and caring shine through, whether you’re engaged in a favorite activity or not.
Also, develop a strategy to spend less time doing activities that you don’t like. One strategy that will work miracles is to respond to your child’s request to do something that bores you by saying, “Yes, for five minutes.” By keeping an activity short, you can meet your child’s needs while honoring your own.
Even if a child protests when the time is up, you can redirect him to continue playing independently. The five minutes you spend with your child — playing hide-and-seek, reading — might otherwise have been spent negotiating or arguing. Using the five-minute strategy creates a win-win situation: Your child gets some playtime and you don’t have to spend that time managing your child’s disappointment.
Additional strategies to try:
- Delegate activities you deeply dislike to a partner, babysitter, or sibling.
- Do something you love or that is useful while doing a parenting activity you don’t like: Create an interesting storyline when playing make-believe, read a favorite magazine while at a soccer game, or do stretching exercises while playing a floor game.
- Redefine an activity to make it fun for you. Instead of putting together train tracks, play trains by lining up chairs and sitting in a seat while the “conductor” collects tickets and drives the train.
Adapted from The Gift of Adult ADD: How to Transform Your Challenges & Build on Your Strengths, by Lara Honos-Webb, Ph.D. Reprinted with permission of New Harbinger Publications.
SUPPORT ADDITUDE
Thank you for reading ADDitude. To support our mission of providing ADHD education and support, please consider subscribing. Your readership and support help make our content and outreach possible. Thank you.
Thank you.
Previous Article Next Article
ADHD and Infidelity — Getting Past the Affair
Is there an association between Adult ADHD and infidelity—that is, cheating on a romantic partner with another person? When there is infidelity, how do you get past it?
The simple answer to the first question is: Maybe. You’ll find a brief summary below.
To the second question (how do you get past it), that’s the main topic of this post. You’ll find an excerpt from perhaps the best book on infidelity. Getting Past the Affair is written by luminaries in the field of couple therapy.
ADHD and Infidelity: A Mixed Picture
When it comes to research, we find very little. Studies on college students with ADHD might find greater rates of sexual promiscuity but how does that relate to adults, including adults in committed relationships? We don’t know.
One genetic study focused on a certain dopamine transporter allele and found associated higher sexual activity. You can read the 2010 paper published in Plos One here: Associations between Dopamine D4 Receptor Gene Variation with Both Infidelity and Sexual Promiscuity
While some research has linked that particular genetic variation to ADHD, it’s not so simple. It’s found in the general population, too, perhaps with counter-vailing genes that exert moderation or forethought.
My ADHD Partner Survey queried the topic of ADHD and infidelity.
Some quick highlights:
- Most respondents said that their ADHD partners were very committed to the relationship.
- A small minority reported their ADHD partners having affairs.
- A small minority reported that they had affairs. Why? They reported feeling neglected and alone, even living with their ADHD partner.
When Infidelity
Has HappenedBelow, you’ll find an excerpt on one of the most-respected books on healing from infidelity. This classic guide is co-written by experts whose research in the couple-therapy field proved key to our new ADHD-Focused Couple Therapy Model.
This classic guide is co-written by experts whose research in the couple-therapy field proved key to our new ADHD-Focused Couple Therapy Model.
I had the pleasure of communicating with one of these highly respected authors and researchers, Douglas K. Snyder, Phd. He graciously provided this endorsement of our new book—and then allowed me to share this excerpt.
In Getting Past the Affair, I found the first chapter provided a useful overview of their program. It is so clearly and compassionately written.
[advertising; not endorsement] [advertising; not endorsement]
Most of all, it takes you by the hand, detailing how and when to move forward, “past the affair.” The authors explain how to move deliberately, and with reflection at each stage.
Please note: I am not the Gina referenced in the opening paragraph. 😉
Excerpt from
Getting Past the Affair:Susan sat motionless in front of the computer. She didn’t know how long she’d been there and just stared at the screen in disbelief.
“I can’t wait to be with you again. Last time was incredible—I still can’t find my bra!”
Someone named Gina had written those words to her husband. She had been searching for a friend’s address when she discovered a series of e-mails to Michael with sexually suggestive subject lines.
Susan could hardly absorb what she’d read. Her brain had turned off and she felt numb. In one brief moment, her life had changed forever.
She felt utterly destroyed.
If you’ve discovered that your partner has had an affair, you probably know how Susan feels. Waves of painful emotion can make it hard to put one foot in front of the other and just go about your daily business.
The barrage of conflicting thoughts about how this could have happened— and the haunting flashbacks and questions about what actually did happen— maybe so distracting that you can’t get anything done.
When you even think about how you’re supposed to react as the woman scorned or the betrayed man, the only solutions that come to mind are the types of soap opera clichés you’ve always laughed at.
What Are You Supposed To Do?
We wrote this book to walk you through an agonizing time in your life and lead you to the answer that’s best for you. The best answer for you may not prove to be the best answer for your partner—and certainly not for the couple down the street. But each of you has a chance to move on in a healthy way.
- Moving on in a healthy way means recovering personally from the affair so that you can pursue the future you want.
- It means knowing enough about what happened and why it happened to make a wise decision about whether to stay together or part.
- It means protecting yourself from being hurt again without carrying the backbreaking—and heartbreaking—burden of anger and suspicion or guilt and shame for the rest of your life.
- The key is the adage “Everything in its time.” In this book, you’ll find a chronological process that has helped hundreds of our clients move on from an affair in a healthy way.
- It’s a methodical but flexible program, and we know it works because it’s based on the only treatment for infidelity that has been scientifically evaluated, a treatment that grew out of more than 50 years of our collective clinical experience and that we’ve taught to other therapists for the past decade.
 Besides being university professors and researchers, all three of us are clinical psychologists and therapists who specialize in working with couples having relationship difficulties, infidelity being one of our major areas of work.
Besides being university professors and researchers, all three of us are clinical psychologists and therapists who specialize in working with couples having relationship difficulties, infidelity being one of our major areas of work.
We’ve also written numerous articles and conducted frequent workshops for therapists in the United States and abroad on helping couples who are struggling to recover from an affair. All of this experience has gone into the program you’ll read about here.
Why Do This Work? To Emerge Whole
Why should you undertake this work, especially when you’re feeling so beaten down by the trauma of the affair? Because the issues you’re wrestling with right now won’t just go away with time. If you simply try to wait out the pain or tackle problems and issues in the wrong order, you can easily make decisions you’ll regret. You can certainly end up with unresolved hurt and anger.
Right after an affair is revealed, the most important tasks are to find a way to cope with the emotional turmoil and to know how to get through the day with your partner without making things worse or letting the rest of your life fall apart. Then, and only then, should you start to take a close look at your partner, yourself, and your history together. You do this so that you can figure out what made your relationship vulnerable to an affair and how you could change things in the future so that this marriage or a future one is on more solid ground. But this is work you should do, to whatever extent you feel able.
Then, and only then, should you start to take a close look at your partner, yourself, and your history together. You do this so that you can figure out what made your relationship vulnerable to an affair and how you could change things in the future so that this marriage or a future one is on more solid ground. But this is work you should do, to whatever extent you feel able.
Our experience has shown conclusively that this is the best way to emerge whole after an affair. Following the program in this book will leave you with a new understanding of yourself and your partner. You may emerge with a new view of what it means to be in a committed relationship and what the ideal partner looks like.
And, though you may not believe it right now, if this turns out to be what you want, you very well could end up with a relationship that’s stronger and better than it was before the affair.
Who Can Benefit From This Book?
- This book is for anyone who has experienced an affair.
 Currently, about 20% of men and 10% of women engage in sexual infidelity at some point in their lives—and nearly 45% of men and 25% of women when emotional (nonsexual) affairs are included.
Currently, about 20% of men and 10% of women engage in sexual infidelity at some point in their lives—and nearly 45% of men and 25% of women when emotional (nonsexual) affairs are included. - An affair involves violating the expectations or standards of a relationship by becoming emotionally or physically involved with someone else, no matter what word you use to define it. You may think of this event in your life as an affair, infidelity, betrayal, outside involvement, tryst, one-night stand, or something else, depending on its duration or intensity and whether it was primarily sexual, primarily emotional, or—as is usually the case—both.
- You stand to gain from this book whether the affair was just revealed or you’ve been struggling with it for some time. The book will help you recover whether you’re the injured partner (the one who did not have the affair) or the participating partner (the one who did).
- When we say “you,” here and in the rest of this book, most of the time we mean the injured partner.
 Our work has shown that injured partners are generally more traumatized by an affair than participating partners. Therefore, they’re more likely to seek help. That’s why we address you in particular through most of this book. But at times we’ll also address the person who had the affair (and we’ll make clear when we’re doing so), as well as the two of you as a couple.
Our work has shown that injured partners are generally more traumatized by an affair than participating partners. Therefore, they’re more likely to seek help. That’s why we address you in particular through most of this book. But at times we’ll also address the person who had the affair (and we’ll make clear when we’re doing so), as well as the two of you as a couple. - We need to talk to your partner, too. We know from our work that you stand the best chance of emerging whole and healthy when you both gain a full understanding of what happened.
How Should You Use
Getting Past the Affair?You can benefit from doing the work in this book whether you do it alone or with your partner. If your partner reads it, too, you will be the beneficiary. That’s true even if you work through it separately,
Participants in affairs need to be honest with themselves about whether they’re ready to end all involvement with the outside person. They need to figure out how to express care for their partners once the affair is over, as well as remorse. It’s important that they understand why they ended up getting involved in an affair. If your partner explores these issues, trust and intimacy may grow between you again.
They need to figure out how to express care for their partners once the affair is over, as well as remorse. It’s important that they understand why they ended up getting involved in an affair. If your partner explores these issues, trust and intimacy may grow between you again.
Ideally, both you and your partner will read each chapter and work through the program. You can do much of the suggested work separately. Yet some of it involves having conversations or engaging in activities together that will help you move forward. Still, we know that reality is rarely ideal. You may end up working through this book alone for different reasons.
Maybe your partner is one of those people who really don’t like “self-help” books. Or perhaps your partner refuses to discuss what’s happened. Or possibly you’ve already ended your relationship because of an affair, but you want to explore the experience on your own. That’s a wise move. There’s plenty of research (including our own) that suggests that if traumatic relationship events such as an affair aren’t addressed adequately, their negative impact could affect future relationships.
If you have children with your partner, reading this book may help you resolve lingering resentments that might otherwise spill over into your co-parenting relationship and negatively affect your children.
As A Couple—Or Solo
Whether for these reasons or any others you plan to use this book on your own, your personal insights and increased understanding will put you in a better position to decide what to do about the future of your relationship if you’re still with your partner.
Moreover, once you learn to think about the affair and approach your life differently, you can change your relationship even if your partner isn’t involved in making the same efforts. Although two people working together to make changes are often more effective than one, even one is better than none. So read this book for yourself and for your relationship— current or future. If you’re involved in individual counseling while reading this book, share what you’re reading with your counselor. Together, explore how this material applies to you.
Together, explore how this material applies to you.
We’ve presented the chapters in the order that has been most helpful to the couples we’ve counseled. The chapters generally build on each other. If certain questions, however, seem particularly important to you, go ahead and read in whatever order you wish.
What Will You Gain?
From all the couples we’ve ushered through this process, we know that your first challenge is to deal with the initial devastation by avoiding further damage and managing essential tasks in the home.
Part I: Coping With The Immediate Trauma
Part I is about coping with the immediate trauma. It will help you:
- Deal with intense feelings—your own and your partner’s.
- Communicate about extremely difficult topics.
- Decide how to go on with your daily routine, from managing chores and finances to parenting.
- Figure out how to keep living together while you regroup (should you sleep together? have sex?)—and under what limited circumstances an immediate separation makes sense.
- Establish boundaries with the outside affair person (i.e., the one with whom the participating partner had the affair)—who may not want to end the affair.
- Determine how much, if anything, to share with others about the affair—including your children, family members, or close friends.
- Take care of yourself even when it seems like your lowest priority, including getting help from friends and seeing your doctor when you need to. Once you and your partner have restored some equilibrium to your relationship,
Part II: Examining The Factors
Part II will help you examine all the factors that might have made your relationship vulnerable to an affair. It will help you:
- Look clearly at your relationship over the years—whether it’s fulfilled your dreams, how it’s changed, whether its foundations were shaken, and by what.
- Understand the characteristics and events that led one of you to have an affair.
- Understand what “infidelity” really means—and how boundaries can get crossed without any intention of hurting one’s partner.

- Recognize how your environment, events, and other people helped set the stage.
- Understand how the injured partner can unwittingly contribute to a relationship’s vulnerability—without being responsible for the participating partner’s decision to have an affair.
- Avoid the temptation to be content with incomplete or partly accurate explanations just to avoid delving deeply into difficult topics.
- Arrive at a coherent picture or “narrative” of the affair that makes sense.
Part III: Moving Forward
Part III guides you in making good decisions about moving forward— either separately or together. It will help you:
- Consider what it means to “move on” and how to get past disabling hurt feelings.
- Anticipate and deal with setbacks, whether together or apart.
- Continue strengthening your relationship and minimizing future risks if you’ve decided to stay together.
We don’t presume to know what decisions you’ll make down the road. Yet, we’re confident that working through this book will lead you through a healthy process as you make the journey. We hope it will help ease the pain and uncertainty along the way. Right now, just understanding what’s happened, figuring out how to get through the day, and hurting less are important goals. So let’s get started.
Yet, we’re confident that working through this book will lead you through a healthy process as you make the journey. We hope it will help ease the pain and uncertainty along the way. Right now, just understanding what’s happened, figuring out how to get through the day, and hurting less are important goals. So let’s get started.
End Excerpt
Have You Experienced Adult ADHD and Infidelity?How do you suspect ADHD—probably unrecognized or poorly managed—might have played a role?
If you and your partner worked past it, how did you do it?
Please share in a comment.
—Gina Pera
How to Stay Productive with Attention Deficit Hyperactivity Disorder
January 13, 2020 Productivity
Personal experience of a woman who built a successful career, despite the tendency to procrastinate and forget everything in the world.
Attention deficit hyperactivity disorder (ADHD) is a neurological disorder that makes it very difficult for people to focus on anything for long periods of time. According to statistics, 4.4% of the total adult population suffers from this disorder. People with this syndrome experience problems with employment, education, more often abuse alcohol and get into traffic accidents.
According to statistics, 4.4% of the total adult population suffers from this disorder. People with this syndrome experience problems with employment, education, more often abuse alcohol and get into traffic accidents.
However, ADHD is not a death sentence. Some manage to adapt to it. For example, Sasha Kollekat.
Sasha Collecutt
Blogger, training specialist at Fusion Sport.
The diagnosis of ADHD has had a profound effect on my career. I have lived my whole life in the sincere belief that meeting a deadline is like reaching for the clouds in the sky. That choosing clothes before going to work can take all morning. And that criticism must necessarily be discouraging and frustrating.
I realized that my career experience was not normal. And this understanding helped me: I was able to adapt.
I am now 33 years old and have a job that I love and excel at. Each new day brings me interesting tasks that I can foresee, evaluate and solve in a timely manner. Many of my colleagues believe that I am a very responsible and organized person (which surprises me myself).
Many of my colleagues believe that I am a very responsible and organized person (which surprises me myself).
Various productivity tips and techniques that are good for other people are usually not effective for me. And so, in order to keep my job and achieve career growth, I set myself the task of finding a system that would help me. ADHD usually has a specific effect on executive functions. In my case, the following abilities were affected:
- Working memory - that is, the ability to retain information in the head for a short period of time. Problems with this characteristic at work make it very difficult to return to your assignment after you have been interrupted or distracted. For the same reason, people with ADHD find it difficult to follow complex instructions.
- Emotional self-regulation — the ability to correctly build one's behavior depending on the current situation. If you do not have well-developed emotional regulation skills, you will react painfully to criticism and miss out on career opportunities.
- Self-motivation - the ability to act in accordance with one's desires. Even if you want to improve your life, keeping promises to yourself can be very difficult. And if you do not cope, it will entail sad career and financial consequences.
- Planning - the ability to foresee the future, reasonably estimate time and predict the results of events. Meeting deadlines, being punctual in meetings, and determining the resources needed for a given task are important in any job. But people with ADHD have a hard time even just thinking about time - this strange, often unrecognized symptom has been studied by specialists from Umeå University in Sweden.
Procrastination and forgetfulness - eternal companions of attention deficit hyperactivity disorder - constantly haunted me at work. They just ruined my career, causing a lot of stress and frustration. And I set myself the goal of dealing with them.
How to deal with procrastination
Constant painful procrastination is one of the main signs of ADHD in adults. This is a real spiritual torture - depressing, exhausting and ... voluntary. And to defeat her, you must make your own choice. I am want to be in the office on time, complete projects on time, achieve success and be a great training manager. I do not want to be a bad or at least an average worker.
This is a real spiritual torture - depressing, exhausting and ... voluntary. And to defeat her, you must make your own choice. I am want to be in the office on time, complete projects on time, achieve success and be a great training manager. I do not want to be a bad or at least an average worker.
I believe that procrastination is just a symptom of my disease.
It's like realizing that you're just not prepared for climbing. Yes, it's a problem (let's not pretend ADHD is all about rainbows and unicorns). But this is a problem that can be dealt with.
Don't think about other people's expectations
I'm very careful about the things I'm given. Instead of thinking that I should do this or that because it is a colleague or client needs , I pull myself together and say to myself: I want to do this because I believe that my tasks are important for me . I try to fit my tasks into my own plan for the future and not perceive them as being imposed on me.
When I think I must do something because others expect me to do it, I run the risk of becoming indifferent to it. And it allows the procrastination monster to take over my mind. Therefore, I think of the company's projects as my own initiatives, work schedules as my personal schedule, and so on. I am always looking for ways to motivate myself personally.
Look at the problem differently
If you can't bring yourself to do something, try a more interesting problem. Do not quit what you started and switch to something completely different, no. Just look at the problem from a different angle.
For example, if you are tired of writing the same e-mails with answers to the same questions of colleagues, write a detailed guide and send them a link to it. Instead of tediously entering data manually using the same template, learn the basics of programming and automate the routine.
Delegate low priority projects to subordinates or interns. Ask for help from colleagues.
Most importantly, avoid procrastination.
Do something you haven't done before
Procrastination is a merciless beast, but it doesn't adapt well to sudden changes. Take advantage of this. Not working in the office - try doing it in the library, cafe or park with a laptop. Do you usually work in silence? Turn on the music this time.
Buy a new perfume. Eat something unusual for lunch. Rearrange your table. Write with a non-dominant hand. Install another text editor. Change the hours you work. In general, introduce some novelty into the routine, and procrastination will recede. At least for a while.
Fool your procrastination
Sounds silly, but it works. For example, if I can’t get ready for work in the morning, I say to myself: “I’m not going anywhere yet, I’m just packing my things.” Then: “I don’t get into the car yet, but just enjoy the weather outside.” And then, having come to work: “I haven’t sat down at the table yet, I just drink coffee. ”
”
And finally, starting the tasks: "I'm not working yet, I'm just sketching out a plan." And by the time the procrastination monster realizes what's going on, I'm already fully immersed in the work process and redoing a bunch of things.
Praise yourself for accomplishments
Finishing important work at 3 am because you have been putting it off for a long time is very unpleasant. You would probably be glad that the deed is done, but, most likely, you will still be angry with yourself that you have been pulling the cat by the tail for so long.
Anger is a bad weapon against procrastination, while contentment and self-pride, on the contrary, help a lot.
Therefore, do not forget to praise yourself for the seemingly smallest victories.
I enjoy going through my to-do list and having fun checking off completed items. Opening the inbox of your email and finding that all emails have been answered - what could be more beautiful? And watching the company thrive because of my efforts is very motivating.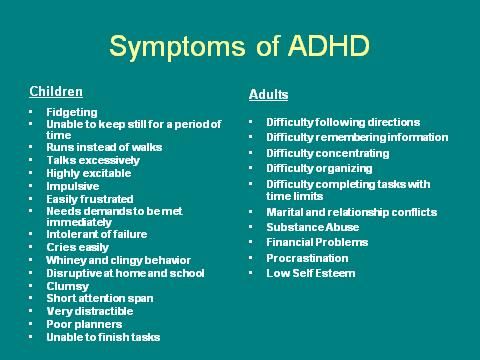 And for self-esteem.
And for self-esteem.
Understand the very nature of procrastination
This will help you be a little more tolerant of yourself as you try to curb it. Procrastination is a kind of attempt to restore your mood. This monster is trying to convince you that the pleasure of doing nothing in the short term outweighs all the problems that you will face later as a result of your inactivity.
How to deal with forgetfulness
Forgetfulness is extremely common among people with ADHD. In fact, this is the most common symptom of this disorder. I was very embarrassed because of my bad memory and was constantly criticized and even scorned by others.
I keep forgetting little things. For example, I can suddenly forget what I did yesterday. Or who are my favorite writers. I forget to make regular backups, perform scheduled tasks, and come to appointments and meetings, even if they repeat weekly at the same time.
Dealing with ADHD is hard work, and dealing with forgetfulness requires a lot of effort. Don't waste your resources trying to deal with your weak memory. Focus on acquiring permanent knowledge.
Don't waste your resources trying to deal with your weak memory. Focus on acquiring permanent knowledge.
Observe
Saying "focus your attention" in an article about ADHD is silly, so I won't tell you that. Observation is much more than just attention.
It requires openness, curiosity, interest and focus on your feelings.
Curiosity is fine with people with ADHD. The main thing is that when you observe, do it with the firm intention of understanding and repeating the actions you see yourself.
Read
I read a lot. This is the most efficient way to learn. The more I read, the better I learn. I am not picky in this matter. I read news in the RSS manager, newsletters, media, open access magazines and new books. I borrow, buy and even restore many titles.
Take the time to reread books and absorb, summarize, test, and apply the knowledge you gain through reading. Knowledge is of no use if you do not put it into practice.
Write
Even the process of writing this article is helping me to combat forgetfulness from ADHD. Just like reading an article helps you.
Packing what you know into logical and understandable text is difficult, but doing so reinforces your knowledge.
No wonder students take notes. If you can write by hand instead of typing, even better. As with reading, take the time to reread and rethink what you write down—days, weeks, months, or even years later.
Teach others
Can you explain something of which you are competent to an inexperienced beginner? The ability to share your knowledge is a true sign of professionalism. I teach others to test how deep my knowledge is. This is for me something like a test of my own abilities - how quickly can I pull up a beginner to my personal level.
Enjoy your own learning
Like most people with ADHD, I have an inexorable drive for novelty and surprise. And it's good for learning. The topics that I master are remembered better if they are relevant to my work.
The topics that I master are remembered better if they are relevant to my work.
Therefore, I try to gain knowledge about everything that is even remotely related to my field of activity.
Do your best to constantly learn something new in your field. Strive to master all aspects of your work.
Recognize ephemeral knowledge and get rid of it in time
Ephemeral knowledge is information that is useful only for a short time. You need to remember that your flight is scheduled for 3 p.m. on Tuesday so you know when to pack and go to the airport. But as soon as you find yourself on a plane, this information can be thrown out of your head without any consequences - as no longer necessary.
Ephemeral knowledge can be easily forgotten and restored later. Therefore, do not waste energy on memorizing such information. Research shows that it's better to remember as Access ephemeral knowledge rather than trying to keep it in your head.
Here are some examples of such information (I don't even try to remember this information because I know where to get it if needed):
- The day my colleague left for work (this is written in my calendar).
- Vincenty's inverse equation (there is a Wikipedia for such things).
- What Nothofagus pollen looks like (see reference book).
- Do I need a visa to travel to a particular country (Google will help here).
I have this information stored in many places at the same time. For example, I enter something in my notebook and at the same time make a note on the calendar with a detailed description. I email a note to myself and then forward it to my messenger so it's available on all my devices. I even use sketches on scraps of paper.
But if it's possible to save yourself the trouble of remembering things and deal with them right away, do it. For example, if you think you'll forget to send an email to a client, send it now, without delay.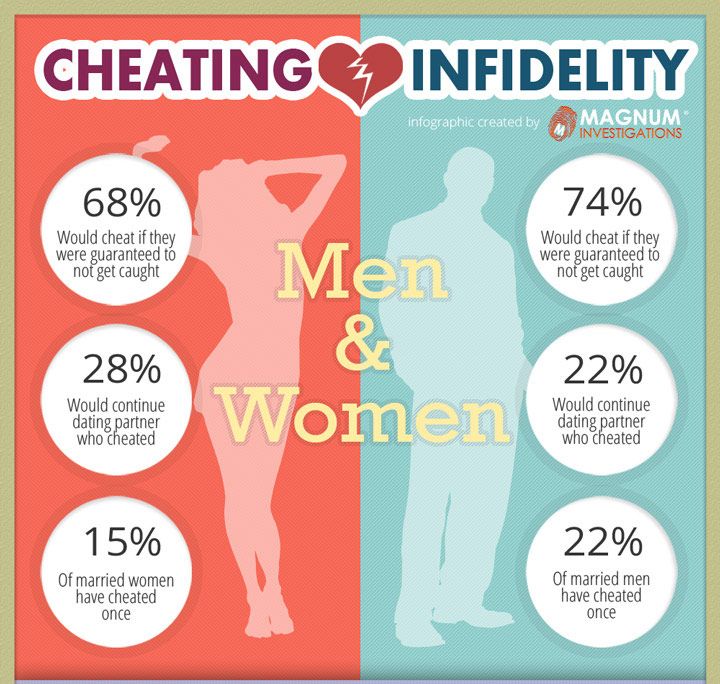 At the same time, save time for more pressing things.
At the same time, save time for more pressing things.
What is the result
I have adapted to my ADHD and it helps me in my life and career. You can do it too. I won't pretend it's easy, but progress is progress.
My goal was to deal with the two main symptoms of ADHD: procrastination and forgetfulness. And I had two strategies:
- Against procrastination: avoid direct interaction with the procrastination monster.
- Against forgetfulness: study what is really important and weed out ephemeral knowledge.
I hope that my experience will be useful for you.
Read also 🧐
- How to manage attention and concentrate
- What really goes on in a procrastinator's head
- How to recognize ADHD in a child and help him
Higher education BSPU
Lecture on the training course "Pedagogical support for children with ADHD", topic 1 "Concept, clinical principles and manifestations of ADHD"
Concept, clinical signs and manifestations ADHD
Questions:
- The concept of ADHD.

- Clinical manifestations and types of ADHD.
- A historical outline of the study of ADHD.
- Prognosis of the development of a child with ADHD.
- Typical problems of a child with ADHD.
1. The concept and signs of the disease
A hyperactive child is constantly on the move, does not complete a single task, does not respond to comments. He "starts" the class and got everyone already: teachers, parents, and children! However, the main symptom of the disease is distracted attention: the child cannot concentrate on anything, whether it is a game, study or watching a TV show.
Have you all seen such children and used an unkind word to commemorate their parents who raised them poorly? In fact, these children are sick.
PORTRAIT OF FIDGET PHIL
For the first time a child with a similar pathology was described by the German neuropsychiatrist Heinrich Hoffman and gave him the nickname Fidget Phil ; since then, doctors have called children with this syndrome.
At the age of 7, Phil, as a rule, is not yet ready for school, his higher brain functions have not fully matured. He is often distracted in class and makes many mistakes. It can be difficult for him to master reading, writing and counting, but not because of a weak intellect, but because of a violation of perception. He can work productively for no more than 5-15 minutes - then his brain "turns off" for 3-7 minutes, accumulating energy for the next work cycle. At this time, Phil is engaged in extraneous matters and does not react to the words of the teacher.
Phil is always in a hurry, fussing, aimlessly grabbing objects, opening drawers... He is long-winded, jumping from one to another in conversation. May suffer from tics, grimace, make obsessive movements. He often bumps into corners, cannot stand on one leg, and sometimes suffers from fine and gross motor impairments. In 68% of such livestock, sleep disturbances are noted, in 40% - bedwetting.
Phil is impulsive, excitable and aggressive. He is internally tense all the time, his mood instantly changes, often there is a feeling of fear, anxiety and anxiety. Phil finds it difficult to get along with his peers. He lags behind them in mental development, but seeks to command and lead, so he has few friends. Relationships with adults are also difficult: punishments do not work on him, and praises do not stimulate him. The reward must be very strong in order for Phil to behave better.
He is internally tense all the time, his mood instantly changes, often there is a feeling of fear, anxiety and anxiety. Phil finds it difficult to get along with his peers. He lags behind them in mental development, but seeks to command and lead, so he has few friends. Relationships with adults are also difficult: punishments do not work on him, and praises do not stimulate him. The reward must be very strong in order for Phil to behave better.
Previously, this pathology was called as soon as: "mild brain dysfunction", "hyperkinetic syndrome", "motor disinhibition"... In recent years, doctors have settled on the name "attention deficit hyperactivity disorder".
ADHD is one of the manifestations of minimal brain dysfunction (MCD), that is, very mild brain insufficiency, which manifests itself in a deficit of certain structures and impaired maturation of higher levels of brain activity. MMD is classified as a functional disorder that is reversible and normalizes as the brain grows and matures. MMD is not a medical diagnosis in the truest sense of the word; rather, it is only a statement of the fact of the presence of mild disorders in the brain, the cause and essence of which have yet to be clarified in order to begin treatment. Children with a reactive type of MMD and are called differently hyperactive .
MMD is not a medical diagnosis in the truest sense of the word; rather, it is only a statement of the fact of the presence of mild disorders in the brain, the cause and essence of which have yet to be clarified in order to begin treatment. Children with a reactive type of MMD and are called differently hyperactive .
Attention deficit/hyperactivity disorder - dysfunction of the central nervous system (mainly the reticular formation of the brain), manifested by difficulties in concentrating and maintaining attention, learning and memory disorders, as well as difficulties in processing exogenous and endogenous information and stimuli.
Prevalence.
According to statistics, about 5-10% of school-age children suffer from Attention Deficit Hyperactivity Disorder. Approximately 20%-60% of the syndrome persists into adulthood. By adolescence, motor hyperactivity usually subsides, but learning disabilities, lack of attention, and inability to concentrate persist in most children.
Now this diagnosis is heard more and more often. Statistics (Zavadenko N.N.) shows that in Russia there are 4 - 18% of such children, in the USA - 4 - 20%, in the UK - 1 - 3%, in Italy - 3 - 10%, in China - 1 - 13 %, in Australia - 7 - 10%.
On average, there are at least 1-2 children in each class who need treatment for this condition. Most often, it manifests itself at the age of 6-12, when the "zhivchik" goes to school and it turns out that he himself cannot study, and interferes with others.
And then the problem turns from a medical one into a social one: not achieving success in studies, receiving criticism for their behavior, such children behave worse and worse. World statistics confirms that among juvenile delinquents there are many patients with attention deficit hyperactivity disorder.
Gender differences
All researchers emphasize the higher prevalence of the disease among boys compared to girls.
According to the authors and the literature, among boys 7-12 years old, signs of the syndrome are diagnosed 2-3 times more often than among girls. Among adolescents, this ratio is 1:1, and among 20-25-year-olds it is 1:2, with a predominance of girls. In the clinic, the ratio of boys and girls varies from 6:1 to 9:1.
Among adolescents, this ratio is 1:1, and among 20-25-year-olds it is 1:2, with a predominance of girls. In the clinic, the ratio of boys and girls varies from 6:1 to 9:1.
The predominance of boys is not only a consequence of the subjective opinion of the respondents answering the questionnaire. Although teachers most often see violators of the order in boys. The high frequency of symptoms of the disease in boys may be due to the influence of hereditary factors, as well as the higher vulnerability of the male fetus to pathogenetic effects during pregnancy and childbirth. In girls, the large hemispheres of the brain are less specialized, so they have a greater reserve of compensatory functions compared to boys with damage to the central nervous system.
In addition, there are gender differences in the structure and dynamics of behavioral disorders. In boys, symptoms of hyperactivity and other behavioral disorders appear from the age of 3-4, which forces parents to consult a doctor even before the child enters school.
Among girls, hyperactivity is less common, the disease in them often manifests itself in the form of attention disorders. In girls, behavioral deviations manifest themselves more latently and therefore are not detected during one or two follow-ups, therefore they are not treated and have a more unfavorable prognosis. To a much greater extent, compared with boys, they have social maladaptation, learning difficulties, and personality disorders.
Status and race
There is no clear evidence that either socioeconomic status (SES) or race affects the prevalence of ADHD. Although some studies indicate a higher percentage of ADHD among children with low SES and African American children, these data may be due to the increase in this set of conditions of aggression and behavior problems, and not ADHD itself (see Barkley, 1996).
2. Clinical manifestations and types of ADHD
Psychological portrait of a hyperactive child
You cannot hold such a child in your hands, he is like a spinning top. To say of him that he is restless is to say nothing. It's like mercury. They did not keep track - and he is somewhere upstairs, from where he can be removed only with the help of a fire escape. Penetrating into all the cracks, falling into all the pits, climbing all the nooks and crannies, exploring all the attics and basements, touching everything and overturning everything, filling himself with bruises and bumps, he rushes day and day around the apartment, around the yard, and without proper supervision and through the streets.
To say of him that he is restless is to say nothing. It's like mercury. They did not keep track - and he is somewhere upstairs, from where he can be removed only with the help of a fire escape. Penetrating into all the cracks, falling into all the pits, climbing all the nooks and crannies, exploring all the attics and basements, touching everything and overturning everything, filling himself with bruises and bumps, he rushes day and day around the apartment, around the yard, and without proper supervision and through the streets.
It is the super mobile who most often escapes from the kindergarten, but not intentionally, but because he discovers an accidentally open gate or a gap in the fence. It is he who most often finds himself on the carriageway of the street, arranges a short circuit in the electrical network or overturns a pot of boiling water on himself. If at least one sewer manhole is not covered by negligence in the city, the super-mobile one will climb in there without thinking how he will get out of it. It is he who finds and blows up the cartridges and grenades left over from the war. Naturally, the lion's share of accidents happens to him.
It is he who finds and blows up the cartridges and grenades left over from the war. Naturally, the lion's share of accidents happens to him.
His hands are in constant motion: they are wrinkling, tearing, turning buttons, peeling the paint on the wall. He can't sit still. He even stands, shifting from foot to foot, and it seems that in another moment - and he will take off, rush to the ends of the world. He eats either standing, or literally bouncing on a chair. He will dodge all over, even playing, listening to a fairy tale, looking at the TV screen. Sometimes it seems that he never learned to sit, and it is hard to believe that he did not run for over a year.
Some of the overactive are especially unbearable in the morning, others in the evening, and then they cannot be put to sleep. They play tricks in bed, fall asleep, standing on their knees and elbows, and when they fall asleep, they knock the sheet into a ball, because they are restless even in a dream. Those who are restless in the morning fall asleep instantly and sleep like the dead. But both about the first and the second they say: "It's good when he sleeps." And parents take a breath, feel calm, only after laying down such a child and making sure that he finally calmed down.
But both about the first and the second they say: "It's good when he sleeps." And parents take a breath, feel calm, only after laying down such a child and making sure that he finally calmed down.
Clothes and shoes literally "burn" on the super mobile. He constantly loses his hat, scarf, mittens, and then his school bag, and you can’t get enough of it.
The Overactive is impulsive, and no one dares to predict what he will do in the next moment. And he doesn't know it either. He has everything on a short circuit: he saw - he grabbed - he ran. He acts without thinking about the consequences, although he does not plan bad things and he himself is sincerely upset by the incident, the fault of which he becomes. However, more often he believes that he did nothing wrong, because he did not want it. And if an overactive child broke a vase, then, in his opinion, it fell by itself, because it did not stand well.
He takes punishment easily, because traditional slaps, reproaches, refusals of requests do not upset him. An overactive person does not remember resentment, does not hold a grudge, and, although he quarrels every minute, he immediately reconciles. True, sometimes he is excessively quick-tempered, aggressive, pugnacious, and not harmless and good-natured, but evil and even cruel, but in such cases we are talking about a more severe brain lesion and certainly with increased convulsive readiness of it, which is found during electroencephalographic examination.
An overactive person does not remember resentment, does not hold a grudge, and, although he quarrels every minute, he immediately reconciles. True, sometimes he is excessively quick-tempered, aggressive, pugnacious, and not harmless and good-natured, but evil and even cruel, but in such cases we are talking about a more severe brain lesion and certainly with increased convulsive readiness of it, which is found during electroencephalographic examination.
Due to an excess of feelings, the overactive person is not able to speak calmly, but shouts, proving, justifying, arguing. This is the noisiest child of all. Naturally, he chooses only noisy and active games, in which everything reduces to running around. He's always in the middle of a boyish dump. Not a single "heap is small" can do without it. Extracted from its very thick, rumpled, but happy - this is it, super-mobile. Sweat doesn't dry out. From constant overexcitation, his hair stands on end, his eyes shine and just do not pop out of their sockets. He has many friends, because he is sociable, ready recklessly for any leprosy, does not whine when hurt, and never lose heart.
He has many friends, because he is sociable, ready recklessly for any leprosy, does not whine when hurt, and never lose heart.
The biggest problem of the super mobile is distractibility. His head is like a weather vane in the wind: now turning in one direction, where something briefly attracted attention, then in the other. Having become interested in something, he forgets about the previous one, does not bring a single thing to the end. New impressions lead him from one passion to another. If he ended up at the opposite end of the city, then not knowing how, not remembering the way, for he went first to an unusual car near the parapet, then to a bright shop window, then to the crowd that had gathered on the occasion and as a result found himself in a police station picket, from where every minute sounds of radio: "Attention, who lost the boy?".
Everything attracts his attention, but it does not linger on anything, it slides from one to another: here he is watching a television program, immediately shifts his gaze to a fly on the ceiling, only to be distracted a second later by a conversation between his mother and grandmother. He can't concentrate in class at school. He looks at the blackboard in fits and starts, and the teacher does not attract his attention. He does not hear her explanations, never knows what is given at home. When writing, the overactive skips letters, does not complete words and sentences. In the simplest examples, he makes ridiculous mistakes, but not because of a lack of ability, but due to damage to the areas of the brain that are in charge of writing ( dysgraphia ).
He can't concentrate in class at school. He looks at the blackboard in fits and starts, and the teacher does not attract his attention. He does not hear her explanations, never knows what is given at home. When writing, the overactive skips letters, does not complete words and sentences. In the simplest examples, he makes ridiculous mistakes, but not because of a lack of ability, but due to damage to the areas of the brain that are in charge of writing ( dysgraphia ).
The Overactive is curious, but not inquisitive. He looks at everything, but as a result he sees nothing. If you do not engage in his upbringing, he will remain so: not stupid, but not really smart either. Superficial will be his knowledge, reasoning, conclusions, because in his thoughts he runs, not stopping at anything. Chaos in the head of a hypermobile is akin to chaos in his pockets, where there are a lot of random and scattered things.
Without educative influence, he will confine himself to questions: "Who is this?" and "what is it?", "where?", "where?" and where?" "Why?" will sound, but the hypermobile will be satisfied with the simplest answers, but "what will happen?" may not arise, because it does not interest him. As a result, his orientation will be reduced to superficial ideas about objects and people, to a simplified and concretely grounded knowledge of life, limited to the near space and narrowed environment of communication with those who are like himself. He is not interested in tomorrow and even what will happen tonight.
As a result, his orientation will be reduced to superficial ideas about objects and people, to a simplified and concretely grounded knowledge of life, limited to the near space and narrowed environment of communication with those who are like himself. He is not interested in tomorrow and even what will happen tonight.
Peak manifestations of hyperdynamic syndrome or hypermobility syndrome - 6-7 years with reverse development in favorable cases by 14-15 years. However, obvious already in the first year of life, with improper upbringing, it crushingly manifests itself just from the age of 13 and older, in this case determining the fate of an adult.
In no other case does a child's difficulty, expressed in such blatant disinhibition and distractibility, cause so many complaints and complaints from parents, kindergarten teachers and teachers, as in this one. The super mobile is most threatened by rejection. He is able to bring out of patience the most calm and familiar adults. No one is reproached, shamed, reprimanded, punished as much as someone who is super mobile. In the end, he himself is convinced that there is no more difficult and stupid child in the whole wide world. As a result, most of the super-mobile protesters become embittered. After all, they have, albeit slightly, but the nervous system is damaged: it is highly excitable. And such children tend to react aggressively to incessant pulling and suppression of their activity.
No one is reproached, shamed, reprimanded, punished as much as someone who is super mobile. In the end, he himself is convinced that there is no more difficult and stupid child in the whole wide world. As a result, most of the super-mobile protesters become embittered. After all, they have, albeit slightly, but the nervous system is damaged: it is highly excitable. And such children tend to react aggressively to incessant pulling and suppression of their activity.
If the restraint and suppression is constant and the child is finally convinced that he is "the worst", the hyperactive becomes the leader of the protest difficult teenagers, demonstratively deviating in behavior, ignoring school studies or may become unstable, which he carries like a chip in river, from trouble to trouble. The hypermobile then blindly follows any group of teenagers in their idle pastime. In this variant, the superficiality of interests and relationships with other adolescents, which follows from distractibility, comes to the fore. Some of the over-active, if they are nevertheless scorched with censures and punishments, if they are endlessly pursued by failures, fall into a hysterical neurosis.
Some of the over-active, if they are nevertheless scorched with censures and punishments, if they are endlessly pursued by failures, fall into a hysterical neurosis.
Also, with hyperactivity, children have poor motor coordination, characterized by awkward erratic movements. They are characterized by constant external chatter, which happens when the internal speech that controls social behavior is unformed.
Among these children there may be gifted children with extraordinary abilities. Hyperactive children may have good general intelligence , but developmental disorders prevent its full development. The uncompensated discrepancy between the level of development and intellect is manifested on the one hand in the somatic sphere, on the other hand in the characteristics of behavior. Since the fixed patterns of such deviant behavior (due to the imperfection of the restraining centers) lead to the fact that these children retain them in adulthood, although they cease to be disinhibited and can already concentrate their attention.
One of the three main components of the syndrome is impulsivity, which is determined by a deficiency of a deterrent. The child shows impulsive motor and verbal activity, he acts as if thoughtlessly, moves from one activity to another, chats without thinking (“speech is ahead of thought”). He often does not get along with his peers, in games he becomes a "target".
Annoying and distracting environmental factors in situations such as being at a party or in a store, at a party, in a crowd, etc., change the child's behavior for the worse. An outburst of anger or a shout is accompanied by trivial insults.
The social-behavioral aspects of these children are important not only because of their widespread negative influence on their peers, but also because these children serve as a kind of social catalyst that influences the behavior of others and often in an undesirable direction.
The child has difficulties in relationships not only with peers, but also with adults. In relation to the first, they are aggressive and demanding. School-age children are very sensitive to the behavior of such classmates and reject their friendship. Parents often complain that their children do not have friends and that their peers refuse to study or play with them.
In relation to the first, they are aggressive and demanding. School-age children are very sensitive to the behavior of such classmates and reject their friendship. Parents often complain that their children do not have friends and that their peers refuse to study or play with them.
In sociometric studies, these children often receive negative characteristics from their comrades. They note that these children are "a cause for concern", "annoying other children".
Deviant behavior is manifested in the fact that children are aggressive, explosive, impulsive. Impulsivity remains a pervasive trait. Such children are prone to delinquency, to various forms of grouping, since it is easier to imitate bad behavior than good. And since the will, higher emotions and higher needs have not matured, life develops in such a way that personal problems are already on the way.
Children with ADHD may experience difficulties in relationships, including peer loneliness, affective disorders, anxiety, and even substance abuse. Adolescents with ADHD are more likely to be involved in traffic accidents and are twice as likely to receive notices and fines from traffic inspectors.
Adolescents with ADHD are more likely to be involved in traffic accidents and are twice as likely to receive notices and fines from traffic inspectors.
Types of ADHD in children.
The following types of ADHD can be classified according to the manifestation of symptoms:
Combined type (inattentive/hyperactive/impulsive). A syndrome that combines attention deficit hyperactivity disorder.
Children with this type of ADHD show all three symptoms. This is the most common form of the syndrome.
It is difficult for them to concentrate on one subject for a long time. In addition, they are impulsive, very mobile - they are "jumping" (hyperactive), which can be very annoying during a lesson in the classroom.
Children with this type of disorder are more visible and easier to diagnose.
Hyperactive/impulsive typ. Attention Deficit Hyperactivity Disorder. In this type of ADHD, children show both hyperactivity and impulsivity, but are able to focus.
They are fussy and talkative, feel restless, cannot sit in one place for a long time (for example, during dinner, doing homework, etc.). These children may be traumatized, that is, because of their activity, they are more likely to be injured than children who do not have ADHD. Young children may be overly active and have problems with their impulsiveness (they may interrupt others when talking, grab objects with their hands, behave inappropriately).
Inattentive type . Attention Deficit Disorder Without Hyperactivity This type of ADHD used to be called Attention Deficit Disorder. Children with this type do not show excessive activity. They do not interfere with school lessons and other activities, so their symptoms may not even be paid attention to.
Children with inattention are not able to maintain attention at the appropriate level for their age. Parents and teachers may complain that children are unable to concentrate, are distracted, jump from one activity to another, disorganized, forgetful, and prone to daydreaming.
This type of disorder is more difficult to identify and diagnose. These are the dreamers. They seem to be listening, but in fact they are thinking about something else, easily distracted. They are calm, not very mobile, and the teacher does not pay attention to them. Parents also do not always understand why a quiet, calm child has problems in school, and consider laziness to be the reason.
Attention deficit without hyperactivity is more common in girls.
3. A historical outline of the study of ADHD
The syndrome itself appeared suddenly and very recently. Only in 1980, in the third edition of the American Diagnostic and Statistical Handbook (DSM-III), did a mention of ADHD appear, and until that time no one knew anything about it at all.
In general, the evolution of DSM causes fair bewilderment for many. The first edition of this handbook (1952) provided data on 112 mental illnesses and disorders. In subsequent editions, their number has steadily increased, reaching 374 in the modern, fourth edition!
In subsequent editions, their number has steadily increased, reaching 374 in the modern, fourth edition!
Dr. Carol Travis, author of the best-selling Misdiagnosis, was given a sarcastic diagnosis of her own by the authors of the handbook: "compulsive diagnostic word-creation."
The existence of such a psychological disorder as ADHD was "proven" by a simple vote of experts from the American Psychiatric Association. On the other hand, latent homosexuality was excluded from the list of psychological disorders (where it existed quite reasonably and for many years) under the pressure of politically engaged individuals.
The term "attention deficit disorder" was separated from the broader concept of "minimal brain dysfunction".
The history of the study of minimal brain dysfunction is associated with the studies of E. Kahn et al. (1934), although separate studies have been carried out earlier. Observing school-age children with such behavioral disorders as motor disinhibition, distractibility, impulsive behavior, the authors suggested that the cause of these changes is brain damage of unknown etiology, and proposed the term "minimal brain damage". Later, learning disorders (difficulties and specific impairments in learning writing, reading, counting skills; disorders of perception and speech) were included in the concept of "minimal brain damage".
Later, learning disorders (difficulties and specific impairments in learning writing, reading, counting skills; disorders of perception and speech) were included in the concept of "minimal brain damage".
In 1962 the Oxford International Research Group in Child Neurology held a symposium on the problem of minimal brain damage. It decided that a more appropriate term for this disorder is "minimal brain dysfunction".
It was assumed that while with "minimal brain damage" there are structural changes in the central nervous system, then with "mild brain dysfunction" there is no localized brain damage, but there is neurochemical and neurophysiological dysfunction.
Various authors referred at least 100 clinical manifestations to "mild brain dysfunction", including, in addition to increased motor activity and insufficient concentration of attention, aggressiveness, dyslexia, dysgraphia, dyscalculia, visual-perceptual disturbances, etc.
According to Clements, "mild brain dysfunction" is a disorder in children of average or near average (in some above average) intelligence, with mild to severe behavioral disturbances associated with minimal abnormalities in the central nervous system, which may be characterized by various combinations disorders of perception, speech, memory, attention control, motor functions.
B 1975 . B.D. Schmitt opposed the name of the disease "mild brain dysfunction", justifying this by the fact that such a name is usually associated with brain damage, causing parents to fear for the future of the child, his intellectual development. This "label" follows the child from class to class, from school to school. In addition, according to the author, there is no reliable scientific evidence in favor of this term.
The author substantiates this by the following facts: despite the high prevalence of this pathology in various countries of the world, in some of them, for example in the UK, it is quite rare (0.4%).
In 1980, the American Psychiatric Association developed a working classification - DSM-IV (4th edition of the Diagnostic and Statistical Manual of Mental Disorders) - the term "attention deficit" was first introduced, which replaced the term "mild brain dysfunction ", "hyperactivity". Cases previously described as minimal brain dysfunction are proposed to be considered as attention deficit hyperactivity disorder. The underlying premise was that the most common and significant clinical symptoms of minimal brain dysfunction included impaired attention and hyperactivity.
The underlying premise was that the most common and significant clinical symptoms of minimal brain dysfunction included impaired attention and hyperactivity.
In the ICD-10, the syndrome is covered under "Emotional and behavioral disorders with onset usually in childhood and adolescence" under "Activity and attention impairment" (F90.0) and "Hyperkinetic conduct disorder" (F90.1).
ICD-10 - International Classification of Diseases 10th revision. As of January 2007, this is the generally accepted classification for coding medical diagnoses, developed by the World Health Organization. ICD-10 consists of 21 sections, each of which contains subsections with codes for diseases and conditions.
The basic symptom of the syndrome was the symptom of "impaired attention". This was justified by the fact that attention disorder occurs in all patients with this pathology, and increased motor activity is not always. In addition to the violation of attention, the emphasis is on the inappropriate behavior of the child.
Later S.E. Schawith et al. divided the syndrome into 3 types: attention deficit hyperactivity disorder, attention deficit hyperactivity disorder without hyperactivity, and the so-called residual type syndrome, a term used to describe adolescents and young adults who had attention deficit hyperactivity disorder at an early age.
4. Development prognosis
The prognosis of the disease depends on the severity of symptoms, timely diagnosis and appropriate treatment. With early therapeutic intervention, the prognosis for these children is favorable. However, they need constant supervision until graduation.
Experts note the variability of the course of the syndrome: disorders can continue during adolescence and into adulthood. Excessive activity is usually the first symptom that begins remission - alleviating the course of the disease. The peak manifestation of motor disinhibition occurs at 6–7 years of age, with a reverse development by 14–15 years, impulsivity decreases by the end of school, attention deficit, as a rule, remains to one degree or another throughout life. Remissions are not usually observed before the age of 12 years.
Remissions are not usually observed before the age of 12 years.
R.A. Barkley notes that 25 to 50% of hyperactive children outgrow the syndrome. However, in 6-8% of patients, according to O.V. Khaletskaya and V.M. Troshin, the symptoms of the disorder lead to mental retardation, and at an older age they contribute to the emergence of serious psychopathological disorders and asocial conditions.
For the rest, symptoms of varying severity persist and lead to problems in daily life. Such people are often accompanied by a feeling of "impatient and restless", impulsiveness, social inadequacy, a feeling of low self-esteem throughout life. They are disorganized and have little control over their activities.
In adolescence, hyperactive children develop early cravings for alcohol and drugs. For them, to a greater extent than for healthy peers, a tendency to delinquency is characteristic. Only a small percentage (15% versus 50% in controls) of them graduate from school.
What is the prognosis for children with attention deficit hyperactivity disorder?
1. Over time, the symptoms disappear and the children become adolescents, adults without abnormalities. Analysis of the results of most studies suggests that 25 to 50% of children "outgrow" this syndrome.
Over time, the symptoms disappear and the children become adolescents, adults without abnormalities. Analysis of the results of most studies suggests that 25 to 50% of children "outgrow" this syndrome.
2. Symptoms in varying degrees of severity persist, but without signs of psychopathology. Such children are the majority (from 50% or more). They have problems in their daily life. According to the survey, they are constantly accompanied by a feeling of "impatient and restless", impulsiveness, social inadequacy, a feeling of low self-esteem throughout their lives. There are reports of a higher frequency of accidents, divorces, job changes among this group of people.
3. Severe complications develop in adults in the form of personality or antisocial changes, alcoholism and even psychotic states.
Antisocial behavior is manifested by a wide range of violations, up to serious crime.
Unfavorable prognosis factors for syndrome are its combination with mental illness, the presence of psychopathology in the mother, as well as symptoms of impulsivity in the patient himself.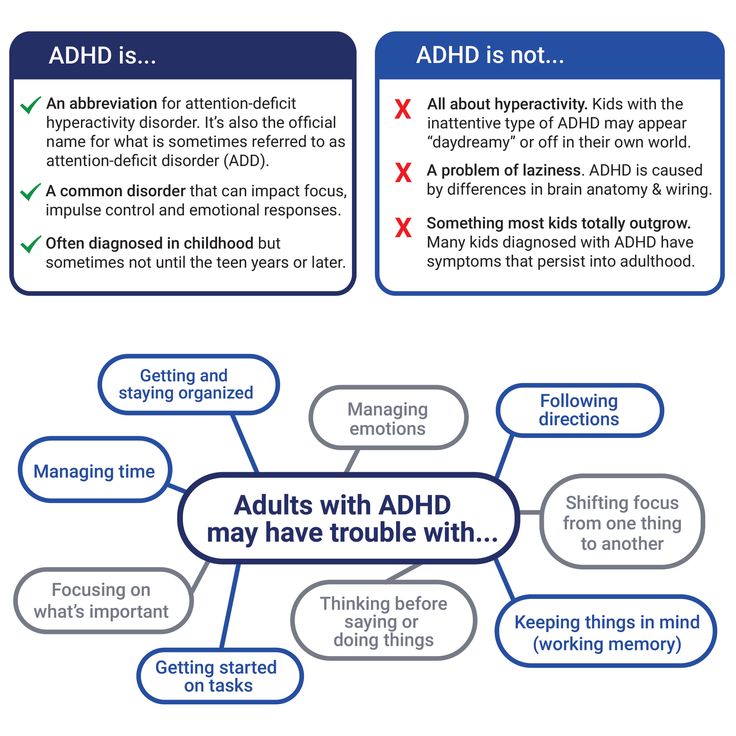
Thus, the prognosis for children with attention deficit hyperactivity disorder is alarming, and the prospects are rather bleak. In such a situation, one cannot hope that children will "outgrow" their condition. Therefore, there is a need for further development of diagnostic methods adapted to our conditions.
5. Typical problems of a child with ADHD
ADHD + conduct disorder (CD). There is a strong association between ADHD and disruptive behavior disorders. By 7 years of age, 35-60% of children with ADHD who are referred to a clinic are also diagnosed with oppositional defiant disorder (ODD), and in mid-childhood and adolescence, 30-50% are also diagnosed with RP. The combination of ADHD + RP occurs earlier than ADHD alone, and the ratio of boys to girls is higher in this case. In general, this is a more severe impairment that negatively affects a wide range of variables related to the children themselves, their relationships with their parents and school performance.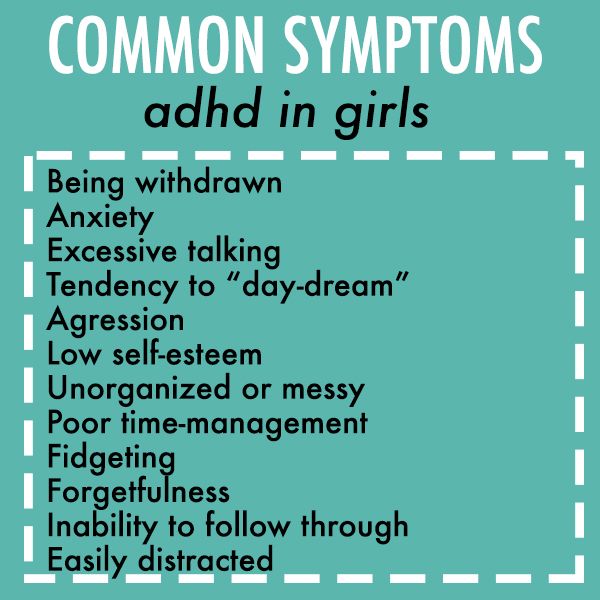
ADHD + anxiety disorder ( TP ). ADHD overlaps with anxiety disorders in 25-40% of the clinical population. The presence of an anxiety disorder, unlike conduct disorder, usually ameliorates rather than exacerbates the disorder. In particular, in children with ADHD + TP, there is a decrease in externalized manifestations in general and impulsivity in particular.
ADHD + learning disability (LL). From 19up to 26% of children with ADHD also have some form of learning disability.
Family relations . The DSM-IV characterizes ADHD as a "disturbing (disturbing) behavior disorder" because its symptoms of aggression, opposition, pushiness, and disorganization undermine the compromise inherent in normal social communication. As you might expect, these symptoms have a negative impact on family relationships.
Mothers are less responsive or less likely to reward their children with ADHD, more negative and domineering in their reactions. Although the relationship of children to fathers is somewhat less problematic, there is also an increase in father-child conflicts.
Although the relationship of children to fathers is somewhat less problematic, there is also an increase in father-child conflicts.
Peer relationships. Annoying, intrusive, and insensitive behavior in children with ADHD markedly increases the likelihood of peer rejection and social isolation. In addition, the time it takes for peers to notice and react negatively to new kids with ADHD is frighteningly short, estimated at minutes and hours. Parental behavior also plays a role in the status of children with ADHD among their peers. Hinshaw and colleagues (Hinshaw et al., 1997) found that authoritative parenting, with its inherent combination of firmly established boundaries, adequate confrontation, reasoning, warmth, and support, markedly promoted social competence in children with ADHD.
Academic problems . Most children with ADHD who are referred to clinics do poorly in school, and about a quarter of them are characterized by more aggressive manifestations.