Premorbid personality types
Variants of premorbid personality and personality disorder: a taxonomic model of their relationships
. 2000;250(5):234-48.
doi: 10.1007/s004060070013.
D von Zerssen 1
Affiliations
Affiliation
- 1 Max-Planck-Institut für Psychiatrie, Munich, Germany.
- PMID: 11097166
- DOI: 10.1007/s004060070013
D von Zerssen. Eur Arch Psychiatry Clin Neurosci. 2000.
. 2000;250(5):234-48.
doi: 10.1007/s004060070013.
Author
D von Zerssen 1
Affiliation
- 1 Max-Planck-Institut für Psychiatrie, Munich, Germany.
- PMID: 11097166
- DOI: 10.1007/s004060070013
Abstract
From a biographical analysis of approximately 500 case records of patients with various kinds of mental state (in particular mood, anxiety and schizophrenic) disorders, a typology of premorbid personality variants was derived. It comprises three "affective types" dominating in patients with major affective disorders and three "neurotoid types" prevailing in other, above all anxiety and schizophrenic, disorders. These types were operationalized so that they could be assessed by means of a diagnostically "blind" rating of biographical case reports or of interview protocols concerning the premorbid development of clinically remitted patients. The material for the present analysis consisted of ratings regarding 120 subjects (100 patients and 20 healthy controls) who had been interviewed within a project primarily aiming at the development of a novel assessment tool, the Biographical Personality Interview (BPI). This data was used for constructing a comprehensive taxonomic model of premorbid personality variants and their relationships to personality disorders. The intercorrelation of type-scores representing the six premorbid personality types suggests a circular order of these types, opposing the "neurotoid types" on one side to the "affective types" on the other side of the circle (circumplex) along a dimension of mental abnormality vs.
It comprises three "affective types" dominating in patients with major affective disorders and three "neurotoid types" prevailing in other, above all anxiety and schizophrenic, disorders. These types were operationalized so that they could be assessed by means of a diagnostically "blind" rating of biographical case reports or of interview protocols concerning the premorbid development of clinically remitted patients. The material for the present analysis consisted of ratings regarding 120 subjects (100 patients and 20 healthy controls) who had been interviewed within a project primarily aiming at the development of a novel assessment tool, the Biographical Personality Interview (BPI). This data was used for constructing a comprehensive taxonomic model of premorbid personality variants and their relationships to personality disorders. The intercorrelation of type-scores representing the six premorbid personality types suggests a circular order of these types, opposing the "neurotoid types" on one side to the "affective types" on the other side of the circle (circumplex) along a dimension of mental abnormality vs. normality. Two types, the ("neurotoid") nervous, tense type, and the ("affective") manic type are contrasted with the ("affective") melancholic and the ("neurotoid") anxious, insecure types along an orthogonal dimension of rather changeable vs. rather constant habitual behaviour. This order is confirmed by the correlation of type-scores with factor scores of the two main dimensions of BPI-item scores. It is also concordant with the correlation of type-scores and scores on questionnaire scales of personality. Personality disorders as maladapted extreme variants of personality can be located outside the circle according to their similarity or dissimilarity with the six premorbid personality types. They are necessarily distributed almost exclusively along the "neurotoid" side of the circumplex. This two-dimensional model of variants of premorbid personality and personality disorders is in basic agreement with models derived from dimensions of personality in mentally healthy subjects and with findings concerning the comorbidity among personality disorders.
normality. Two types, the ("neurotoid") nervous, tense type, and the ("affective") manic type are contrasted with the ("affective") melancholic and the ("neurotoid") anxious, insecure types along an orthogonal dimension of rather changeable vs. rather constant habitual behaviour. This order is confirmed by the correlation of type-scores with factor scores of the two main dimensions of BPI-item scores. It is also concordant with the correlation of type-scores and scores on questionnaire scales of personality. Personality disorders as maladapted extreme variants of personality can be located outside the circle according to their similarity or dissimilarity with the six premorbid personality types. They are necessarily distributed almost exclusively along the "neurotoid" side of the circumplex. This two-dimensional model of variants of premorbid personality and personality disorders is in basic agreement with models derived from dimensions of personality in mentally healthy subjects and with findings concerning the comorbidity among personality disorders. Further empirical studies are required for choosing or developing the most appropriate model of the relationships between personality variants and personality disorders.
Further empirical studies are required for choosing or developing the most appropriate model of the relationships between personality variants and personality disorders.
Similar articles
-
Development of an integrated model of personality, personality disorders and severe axis I disorders, with special reference to major affective disorders.
von Zerssen D. von Zerssen D. J Affect Disord. 2002 Apr;68(2-3):143-58. doi: 10.1016/s0165-0327(02)00045-9. J Affect Disord. 2002. PMID: 12063143
-
The relationship of premorbid personality to subtypes of an affective illness. A replication study by means of an operationalized procedure for the diagnosis of personality structures.
von Zerssen D, Tauscher R, Pössl J. von Zerssen D, et al.
 J Affect Disord. 1994 Sep;32(1):61-72. doi: 10.1016/0165-0327(94)90062-0. J Affect Disord. 1994. PMID: 7798468
J Affect Disord. 1994 Sep;32(1):61-72. doi: 10.1016/0165-0327(94)90062-0. J Affect Disord. 1994. PMID: 7798468 -
An operationalized procedure for the recognition of premorbid personality types in biographical case notes on psychiatric patients.
von Zerssen D, Pössl J, Gruben S, Tauscher R, Barthelmes H. von Zerssen D, et al. Eur Arch Psychiatry Clin Neurosci. 1994;243(5):256-72. doi: 10.1007/BF02191584. Eur Arch Psychiatry Clin Neurosci. 1994. PMID: 8172941
-
Extent of comorbidity between mental state and personality disorders.
Tyrer P, Gunderson J, Lyons M, Tohen M. Tyrer P, et al. J Pers Disord. 1997 Fall;11(3):242-59. doi: 10.1521/pedi.1997.11.3.242. J Pers Disord. 1997. PMID: 9348488 Review.
-
[Hyperthymic disorders].
Féline A. Féline A. Encephale. 1993 Mar-Apr;19(2):103-7. Encephale. 1993. PMID: 8275895 Review. French.
See all similar articles
MeSH terms
Cluster C Personality Disorders: Types, Traits, Treatment, Support
What is a personality disorder?
A personality disorder is a type of mental illness that affects the way people think, feel, and behave. This can make it hard to handle emotions and interact with others.
This type of disorder also involves long-term patterns of behavior that don’t change much over time. For many, these patterns can lead to emotional distress and get in the way of functioning at work, school, or home.
There are 10 types of personality disorders. They’re broken down into three main categories:
- cluster A
- cluster B
- cluster C
Read on to learn more about cluster C personality disorders, including how they’re diagnosed and treated.
Intense anxiety and fear mark cluster C personality disorders. Disorders in this cluster include:
- avoidant personality disorder
- dependent personality disorder
- obsessive-compulsive personality disorder
Avoidant personality disorder
People with avoidant personality disorders experience shyness and unjustified fears of rejection. They often feel lonely but avoid forming relationships outside of their immediate family.
Other avoidant personality disorder traits include:
- being overly sensitive to criticism and rejection
- regularly feeling inferior or inadequate
- avoiding social activities or jobs that require working around other people
- holding back from personal relationships
Dependent personality disorder
Dependent personality disorder causes people to rely too much on others to meet their physical and emotional needs. This often stems from not trusting themselves to make the right decision.
This often stems from not trusting themselves to make the right decision.
Other dependent personality disorder traits include:
- lacking the confidence to take care of yourself or make small decisions
- feeling the need to be taken care of
- having frequent fears of being alone
- being submissive to others
- having trouble disagreeing with others
- tolerating unhealthy relationships or abusive treatment
- feeling overly upset when relationships end or desperate to start a new relationship right away
Obsessive-compulsive personality disorder
People with obsessive-compulsive personality disorder are overly focused on maintaining order and control.
They display some of the same behaviors as people with obsessive-compulsive disorder (OCD). However, they don’t experience unwanted or obtrusive thoughts, which are common symptoms of OCD.
Obsessive-compulsive personality disorder traits include:
- being overly preoccupied with schedules, rules, or details
- working too much, often to the exclusion of other activities
- setting extremely strict and high standards for yourself that are often impossible to meet
- being unable to throw things away, even when they’re broken or have little value
- having a hard time delegating tasks to others
- neglecting relationships because of work or projects
- being inflexible about morality, ethics, or values
- lacking flexibility, generosity, and affection
- tightly controlling money or budget
Personality disorders are often harder to diagnose than other mental health conditions, such as anxiety or depression. Everyone has a unique personality that shapes the way they think about and interact with the world.
Everyone has a unique personality that shapes the way they think about and interact with the world.
If you think you or someone close to you may have a personality disorder, it’s important to start with an evaluation by a mental health professional. This is usually done by either a psychiatrist or psychologist.
To diagnose personality disorders, doctors often start by asking a series of questions about:
- the way you perceive yourself, others, and events
- the appropriateness of your emotional responses
- how you deal with other people, especially in close relationships
- how you control your impulses
They might ask you these questions in a conversation or have you fill out a questionnaire. Depending on your symptoms, they may also ask for permission to talk to someone who knows you well, such as a close family member or spouse.
This is completely optional, but allowing your doctor to speak to someone close to you can be very helpful for making an accurate diagnosis in some cases.
Once your doctor gathers enough information, they’ll likely refer to the new edition of the Diagnostic and Statistical Manual of Mental Disorders. It’s published by the American Psychiatric Association. The manual lists diagnostic criteria, including symptom duration and severity, for each of the 10 personality disorders.
Keep in mind that the symptoms of different personality disorders often overlap, especially across disorders within the same cluster.
There are a variety of treatments available for personality disorders. For many people, a combination of treatments works best.
When recommending a treatment plan, your doctor will take into account the type of personality disorder you have and how severely in interferes with your daily life.
You might need to try a few different treatments before you find what works best for you. This can be a very frustrating process, but try to keep the end result — more control over your thoughts, feelings, and behavior — in the front of your mind.
Online therapy options
Read our review of the best online therapy options to find the right fit for you.
Psychotherapy
Psychotherapy refers to talk therapy. It involves meeting with a therapist to discuss your thoughts, feelings, and behaviors. There are many types of psychotherapy that take place in a variety of settings.
Talk therapy can take place on an individual, family, or group level. Individual sessions involve working one-on-one with a therapist. During a family session, your therapist will have a close friend or family member who’s been impacted by your condition join the session.
Group therapy involves a therapist leading a conversation among a group of people with similar conditions and symptoms. This can be a great way to connect with others going through similar issues and talk about what has or hasn’t worked for them.
Other types of therapy that might help include:
- Cognitive behavioral therapy. This is a type of talk therapy that focuses on making you more aware of your thought patterns, allowing you to better control them.
- Dialectical behavioral therapy. This type of therapy is closely related to cognitive behavioral therapy. It often involves a combination of individual talk therapy and group sessions to learn skills for how to manage your symptoms.
- Psychoanalytic therapy. This is a type of talk therapy that focuses on uncovering and resolving unconscious or buried emotions and memories.
- Psychoeducation. This type of therapy focuses on helping you better understand your condition and what it involves.
Medication
There are no medications specifically approved to treat personality disorders. There are, however, certain medications that your prescriber may use “off label” to help you with certain problematic symptoms.
Additionally, some people with personality disorders may have another mental health disorder which can be the focus of clinical attention. The best medications for you will depend on individual circumstances, such as the severity of your symptoms and the presence of co-occurring mental health disorders.
Medications include:
- Antidepressants. Antidepressants help treat symptoms of depression, but they can also reduce impulsive behavior or feelings of anger and frustration.
- Anti-anxiety medications. Medications for anxiety can help manage symptoms of dread or perfectionism.
- Mood stabilizers. Mood stabilizers help prevent mood swings and reduce irritability and aggression.
- Antipsychotics. These medications treat psychosis. They can be helpful for people who easily lose touch with reality or see and hear things that aren’t there.
Make sure to tell your doctor about any medications you’ve tried in the past. This can help them better determine how you’ll respond to different options.
If you try a new medication, let your doctor know if you experience uncomfortable side effects. They can either adjust your dosage or give you tips for managing side effects.
Keep in mind that medication side effects often subside once your body gets used to the mediation.
If someone close to you may have a personality disorder, there are a few things you can do to help them feel comfortable. This is important, because people with personality disorders might be unaware of their condition or think they don’t need treatment.
If they haven’t received a diagnosis, consider encouraging them to see their primary care doctor, who can refer them to a psychiatrist. People are sometimes more willing to follow advice from a doctor than from a family member or friend.
If they’ve received a diagnosis of a personality disorder, here are a few tips to help them through the treatment process:
- Be patient. Sometimes people need to take a few steps back before they can move forward. Try to allow space for them to do this. Avoid taking their behavior personally.
- Be practical. Offer practical support, such as scheduling therapy appointments and making sure they have a reliable way to get there.
- Be available.
 Let them know if you’d be open to joining them in a therapy session if it would help.
Let them know if you’d be open to joining them in a therapy session if it would help. - Be vocal. Tell them how much you appreciate their efforts to get better.
- Be mindful of your language. Use “I” statements instead of “you” statements. For example, rather than saying “You scared me when…,” try saying “I felt scared when you…”
- Be kind to yourself. Make time to care for yourself and your needs. It’s hard to offer support when you’re burned out or stressed.
If you’re feeling overwhelmed and don’t know where to start, consider starting with the National Alliance on Mental Illness’ guide to finding support. You’ll find information about finding a therapist, getting financial help, understanding your insurance plan, and more.
You can also create a free account to participate on their online discussion groups.
Suicide prevention
- If you think someone is at immediate risk of self-harm or hurting another person:
- • Call 911 or your local emergency number.
- • Stay with the person until help arrives.
- • Remove any guns, knives, medications, or other things that may cause harm.
- • Listen, but don’t judge, argue, threaten, or yell.
- If you or someone you know is considering suicide, get help from a crisis or suicide prevention hotline. Try the National Suicide Prevention Lifeline at 800-273-8255.
Premorbid personality types
06/06/2015
Hyperthymic personality type is distinguished, as a rule, by elevated mood, high vitality, and activity. Patients are burdened by loneliness and forced idleness, but strive for self-reliance and independence.
At the same time, patients do not tolerate strict discipline and a regulated regime; interested in something new, they often do not finish what they started.
Cycloid , or affective-labile, personality type is characterized by alternating periods of upsurge with periods of decline in mood and tone, during which patients are noted: lethargy, loss of strength, decreased performance, they become uncommunicative and inactive. Even the most minor troubles at these moments are experienced by patients very hard. Quite often, there can be long periods of equanimity between periods of ups and downs.
Even the most minor troubles at these moments are experienced by patients very hard. Quite often, there can be long periods of equanimity between periods of ups and downs.
Emotionally labile type is characterized by extreme mood variability. In the life plan of such patients, almost everything depends on the mood: well-being, performance, sociability and attitude towards others. Persons with an emotionally labile personality type have a hard time experiencing troubles, prone to neurotic reactions, sincerely becoming attached to those from whom they see care and attention.
Sensitive (anxious, timid) personality type is characterized by great impressionability, a sense of inferiority. As a rule, such people among strangers or in an unfamiliar environment are timid and shy, sociable with those they are used to. Patients have an extremely developed sense of duty and responsibility.
Psychasthenic (pedantic) personality type combines a tendency to reasoning, indecision with anxious suspiciousness in the form of fears for one's future and the future of loved ones. Such persons live with the idea that if they do not deviate from the routine or the planned plan, then nothing bad will happen. When a decision has already been made, indecision is combined with impatience.
Such persons live with the idea that if they do not deviate from the routine or the planned plan, then nothing bad will happen. When a decision has already been made, indecision is combined with impatience.
Schizoid (introverted) personality type is characterized by isolation, formal contacts, as a rule, are not difficult, but emotional contacts often turn out to be an impossible task. Closure, combined with external restraint and coldness, manifests itself in the inability to respond to the joy, sadness or fears of another person, in a lack of empathy.
Epileptoid (excitable) personality type is usually characterized by a tendency to short periods of angry-dreary mood with boiling irritation and the search for an object on which to vent evil. During such periods, affective explosiveness is often manifested, in a state in which patients can reach unbridled rage.
Hysteroid (demonstrative) personality type attracts attention with an insatiable thirst for power, a desire to be in the spotlight. To achieve such goals, patients show deceit and fantasizing, feigned exaggerated expression of emotions, a tendency to show off and posturing, and excessive dramatization of events. An unstable personality type is characterized by a constant increased craving for pleasure, idleness, idleness, the desire to evade any work, duty and duty.
To achieve such goals, patients show deceit and fantasizing, feigned exaggerated expression of emotions, a tendency to show off and posturing, and excessive dramatization of events. An unstable personality type is characterized by a constant increased craving for pleasure, idleness, idleness, the desire to evade any work, duty and duty.
Key words: Disorders, Personality
Source: Geisler E.V., Psychiatry
| Related materials |
|---|
| Emotionally labile personality disorder Belyalov F.I., Mental disorders in the practice of a therapist |
| Dissocial and emotionally unstable forms of personality disorder ... |
| Organic personality disorder after TBI ... |
| Research of personality development disorders Polin A. |
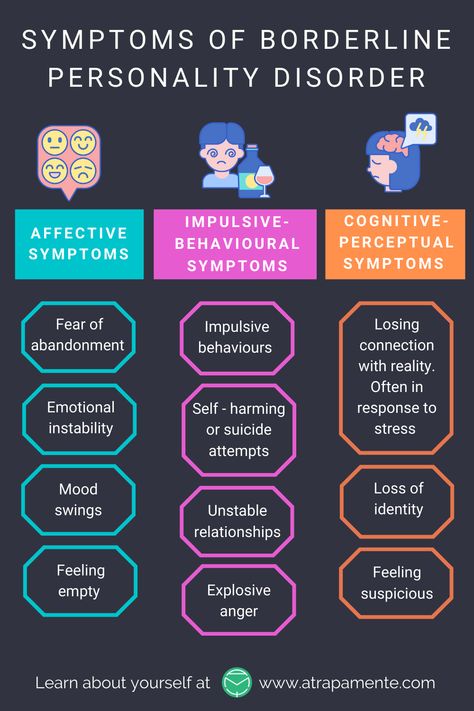
| The concept of "borderline personality disorder" in psychoanalysis Psychoanalysis: a textbook for undergraduate and graduate studies / M. M. Reshetnikov, P86 S. V. Avakumov... |
| Psychodiagnostics of personality disorders ... |
| Personality psychopathology AA Drozdov, MV Drozdova., "The Complete Reference Book of the Psychotherapist": Eksmo; Moscow; 2007 ISBN... |
| Violation of the personal component of thinking T.P. Pushkina Medical psychology |
 V., Medical psychology
V., Medical psychology 1. Premorbid personality types
For diagnostics, prognosis and choice of methods psychotherapy and rehabilitation is important premorbid personality type assessment, which implies its main traits, type of character before it arose mental disorder. Usually, this type is described as the patient himself, as well as his relatives, summary of life history. One of most convenient for evaluation and systematics personality types, as well as premorbid hell is the classification of german psychiatrist K. Leonhard - classification "accentuated personalities". In her based on the concept of accentuation character as excessive amplification its individual features, as a result of which selective vulnerability is detected for certain types of psychogenic impacts at good and even increased resilience towards others. Accentuated personalities are extreme variants of the norm. AT modern society, these include over half of the population.
Usually, this type is described as the patient himself, as well as his relatives, summary of life history. One of most convenient for evaluation and systematics personality types, as well as premorbid hell is the classification of german psychiatrist K. Leonhard - classification "accentuated personalities". In her based on the concept of accentuation character as excessive amplification its individual features, as a result of which selective vulnerability is detected for certain types of psychogenic impacts at good and even increased resilience towards others. Accentuated personalities are extreme variants of the norm. AT modern society, these include over half of the population.
Exist the following main types of accented personalities.
Hyperthymic personality type is different, usually high spirits high vitality, activity. Patients are burdened by loneliness and forced idleness, but strive for autonomy and independence. This type of personality is usually characterized resourcefulness, skill and dodge.
AT at the same time, patients do not tolerate strict discipline and regulated mode; interested in something new, they often do not finish what they started, bad handle work that requires perseverance and meticulousness. Also at these individuals tend to reassessment of their abilities and abilities, excessive optimism in regarding the future.
Cycloid, or affectively labile, type personality is characterized by periods of ups and downs mood and tone, during which Patients are noted: lethargy, decline strength, decreased performance, they become uncommunicative and inactive. Even the smallest troubles in these moments are experienced the sick are very hard. Often enough between ups and downs downturns can be long periods even mood. Duration periods range from several days up to several months.
Emotionally labile type is characterized by extreme mood volatility which occurs even for any about.
AT life plan of such patients from mood depends on almost everything: health, performance, sociability and attitude towards others. Persons with an emotionally labile type individuals are hard pressed for trouble, prone to neurotic reactions, sincerely attached to those from whom see care and attention, need emotional contact and empathy.
Persons with an emotionally labile type individuals are hard pressed for trouble, prone to neurotic reactions, sincerely attached to those from whom see care and attention, need emotional contact and empathy.
Sensitive (anxious, fearful) personality type different great impressionability, feeling own inferiority. How as a rule, such people are among strangers or in an unfamiliar environment timid and shy, sociable with those to whom used to.
At patients are extremely developed sense of duty and responsibility. noticing many shortcomings in themselves, trying overcome them, asserting themselves not there, where their real abilities, but in the area where they weak, trying to overcome shyness and shyness, taking up public posts.
How general anxiety and agitation caused by the fear of making bad impression on others people, it is hard to experience unfriendly attitude towards yourself.
Psychasthenic (pedantic) personality type combines has a tendency to reason, indecisiveness with anxious suspiciousness in the form of fears for their future and the future loved ones. Such persons live with the thought that if you do not deviate from the established order or planned plan, then nothing bad things won't happen. When the decision is accepted, indecision is combined with impatience. Patients tend to introspection, a heavy burden for them is a responsibility, especially when you have to be responsible not only for themselves, but also for others.
Such persons live with the thought that if you do not deviate from the established order or planned plan, then nothing bad things won't happen. When the decision is accepted, indecision is combined with impatience. Patients tend to introspection, a heavy burden for them is a responsibility, especially when you have to be responsible not only for themselves, but also for others.
Schizoid (introverted) type personality is characterized by isolation, formal contacts, like as a rule, not difficult, but overwhelming the task is often emotional contacts. Closure, combined with external restraint and coldness, manifested in the inability to respond to the joy, sadness or fear of another a person with a lack of empathy. Also in this type of persons is greatly reduced intuition, which manifests itself in the impossibility guess about the unspoken desires of other people, to feel sympathy or dislike to yourself.
How as a rule, such patients live internally world filled with hobbies and fantasies that are different unusualness, strength and constancy, patients fantasize about themselves, with others don't share your fantasies.
Epileptoid (excitable) personality type usually tends to be short periods of wickedly dreary mood with seething irritation and search an object on which to unleash evil. During such periods, there is often affective explosiveness, able which patients can reach unbridled rage.
At patients have very strongly developed instincts, especially sexual attraction, which combined with intense jealousy, and sometimes with sadistic and masochistic inclinations. In relation to those around to their people, patients exercise authority. All behavior is heavy, stiffness, inertia. petty accuracy, observance rules, pedantry is often combined with prudence, prudence and vindictiveness.
Hysteroid (demonstrative) personality type draws the attention of an insatiable thirst power, the desire to be in the center attention. To achieve such goals patients show deceit and fantasy, exaggerated expression emotions, a tendency to drawing and posturing, over-dramatization of events.