How long does venlafaxine stay in your system
Effexor Withdrawal: Symptoms & Timeline
Effexor (venlafaxine) is notorious for causing uncomfortable withdrawal symptoms, known as “antidepressant discontinuation syndrome.” Effexor is generally prescribed starting at 75 mg per day, but the max dose can range from 225 mg daily to 375 mg daily, depending on the dosage form of the drug. Skipping doses of Effexor or quitting the drug cold turkey, especially at higher doses, can lead to unpleasant withdrawal symptoms. For this reason, it’s important to take Effexor exactly as your doctor prescribes.
Effexor Withdrawal
When your body becomes used to a substance, suddenly stopping it can cause withdrawal symptoms. Someone who abruptly stops taking Effexor may start to experience withdrawal symptoms 8–12 hours after the last dose. Effexor withdrawal symptoms usually resolve within two weeks.
The most reliable way to prevent or minimize withdrawal symptoms is to gradually taper the Effexor dose over a minimum of two weeks, although a longer taper may be needed. No matter what, it is important to taper Effexor under a doctor’s supervision, especially if you are taking Effexor for a mental health condition like depression. Suddenly stopping Effexor while leaving your mental health untreated may be dangerous.
Effexor Withdrawal Symptoms
Among antidepressants, Effexor is one of the most difficult to quit. Antidepressant discontinuation syndrome (ADS) is characterized by a variety of withdrawal symptoms that occur because of physical dependence. Dependence develops with the regular use of antidepressants. Though it usually develops in six weeks or more, it can develop within just three weeks in some cases.
The presence and severity of Effexor withdrawal symptoms do not seem to be correlated with dose. Currently, it is impossible to reliably predict who will experience symptoms of ADS.
Effexor Brain Zaps
Venlafaxine has one of the highest rates of “brain zap” frequency associated with antidepressant discontinuation. Brain zaps are an electric shock sensation that may also include visual disturbances. Doctors are not sure why this phenomenon occurs. Although this symptom resolves quickly in most people, others experience brain zaps for months or years.
Brain zaps are an electric shock sensation that may also include visual disturbances. Doctors are not sure why this phenomenon occurs. Although this symptom resolves quickly in most people, others experience brain zaps for months or years.
Other Effexor Withdrawal Symptoms
Other common Effexor withdrawal symptoms can be uncomfortable or even debilitating, including:
- Vertigo
- Electric shock sensations in hands or feet
- Nausea
- Lethargy
- Flu-like symptoms
- Loss of coordination
- Anxiety
- Irritability
- Vivid dreams
- Insomnia
Effexor Withdrawal Timeline
The Effexor withdrawal timeline can vary. Symptoms typically begin as early as 12 hours after the last dose and generally resolve within one to two weeks. Because Effexor has a half-life of four hours, it is completely out of the system within a day. Antidepressants with longer half-lives stay in the body for longer amounts of time and may limit the onset and severity of ADS.
Factors Affecting Effexor Withdrawal
ADS typically affects about 20% of people who abruptly stop antidepressant use. However, Effexor may have a somewhat higher rate of ADS frequency — possibly up to 34%. There is currently no reliable way to predict the occurrence of ADS or its severity. Studies have even shown that higher Effexor doses are not predictive of ADS development.
A number of studies have shown that people who taper off of Effexor are significantly less likely to experience ADS, and their symptoms are milder and resolve more quickly compared to people who abruptly stop taking Effexor.
Effexor Withdrawal Treatment
The most reliable way to prevent Effexor withdrawal is to work with your doctor to develop a tapering regime. If you abruptly stop taking Effexor and are experiencing withdrawal symptoms, the only proven way to relieve them is to resume taking Effexor and gradually taper the dose with your doctor. Some studies have shown that cognitive behavioral therapy or mindfulness-based therapies can help people better manage their symptoms.
Medical Detox
Medical detox is not required for Effexor withdrawal, but people with ADS could find success in a rehab center that can help them taper off Effexor safely while providing behavioral therapy and other treatment.
People who take Effexor along with other substances may benefit from a medical detox to avoid withdrawal complications. This is especially true if you take Effexor for a mental health condition, which can worsen withdrawal symptoms.
How to Taper Off Effexor
Anyone who is considering quitting Effexor or other antidepressants should consult with a medical professional. Several studies have shown that the best way to prevent ADS and withdrawal symptoms is to gradually discontinue use.
An Effexor taper schedule may vary from person to person, but a general guideline is to reduce the Effexor dose by 10 mg every two weeks, for a minimum of four weeks. Your doctor can work with you to develop an appropriate tapering schedule that is most effective for your unique situation.
Effexor Withdrawal Remedies
There are no verified remedies for Effexor withdrawal. If you stop Effexor and start to notice withdrawal symptoms, talk to your prescriber immediately. They may be able to restart you on Effexor or another antidepressant, which can resolve your withdrawal.
In addition, it is important to focus on your health, as this may ease withdrawal symptoms. Some tips include:
- Eat a nutritious diet
- Stay well-hydrated
- Consider regular, light exercise, like yoga
- Consider therapy or counseling, especially if you were taking Effexor for a mental health condition
Alternative Treatments for Effexor Withdrawal
Cross-tapering may be an effective method to prevent or minimize Effexor ADS symptoms. Cross-tapering involves transitioning from high doses of Effexor to another antidepressant, often duloxetine, that has a similar makeup. However, there is a risk of serotonin syndrome if cross-tapering is done incorrectly. A “wash-out” period of approximately five half-lives — about 20 hours for Effexor — must be done before starting another medication that inhibits serotonin reuptake.
A “wash-out” period of approximately five half-lives — about 20 hours for Effexor — must be done before starting another medication that inhibits serotonin reuptake.
Outpatient Treatment for Effexor Withdrawal
Outpatient rehab programs that offer cognitive behavioral therapies and other forms of psychotherapy may help people experiencing Effexor withdrawal symptoms. Behavioral therapies are also likely to be incredibly beneficial for people who are concerned about experiencing a recurrence of depression or anxiety.
Detoxing From Effexor at Home
Many people who stop using Effexor, either abruptly or with a taper, do so at home. Since quitting abruptly can increase the risk of ADS, it’s essential to follow your doctor’s advice when it comes to quitting Effexor and home and managing side effects. This includes having a friend or loved one available for support, or to help identify mood changes that can come from stopping an antidepressant.
If you have severe mood swings after stopping Effexor or start thinking about harming yourself or others, seek medical attention right away. Call 911 or the National Suicide Prevention Lifeline at 1-800-273-8225. If you don’t have access to a phone, you can chat online with the hotline.
Call 911 or the National Suicide Prevention Lifeline at 1-800-273-8225. If you don’t have access to a phone, you can chat online with the hotline.
Finding a Detox Center
If you are concerned about Effexor ADS, it is advised to follow a tapering regimen under the care of medical professionals. Look for a rehab facility that has experience with tapering clients off of antidepressants and provides cognitive behavioral therapy.
If you are experiencing antidepressant withdrawal syndrome, The Recovery Village Columbus can help. Our experts will work with you to develop a tapering plan and provide cognitive behavioral therapy to help you overcome withdrawal symptoms and prevent the return of depression. Contact us today to learn about treatment programs that can work well for you.
Editor – Erica Weiman
Erica Weiman graduated from Pace University in 2014 with a master's in Publishing and has been writing and editing ever since. Read more
Medically Reviewed By – Dr. Jessica Pyhtila, PharmD
Jessica Pyhtila, PharmD
Dr. Jessica Pyhtila is a Clinical Pharmacy Specialist based in Baltimore, Maryland with practice sites in inpatient palliative care and outpatient primary care at the Department of Veteran Affairs. Read more
Drugs.com. “Venlafaxine.” October 1, 2021. Accessed March 7, 2022.
Drugs.com. “Venlafaxine ER.” September 1, 2021. Accessed March 7, 2022.
Campagne, DM. “Venlafaxine and Serious Withdrawal Sympt[…]: Warning to Drivers.” Medscape General Medicine, July 6, 2005. Accessed March 7, 2022.
Warner, CH; Bobo, W; et al. “Antidepressant Discontinuation Syndrome.” American Family Physician, August 2006. Accessed March 7, 2022.
Papp, A; Onton, JA. “Brain Zaps: An Underappreciated Symptom […]sant Discontinuation.” The Primary Care Companion for CNS Disorders, 2018. Accessed March 7, 2022.
Maund, E; Stuart, B; et al. “Managing Antidepressant Discontinuation: A Systematic Review.” Annals of Family Medicine, February 2019. Accessed March 7, 2022.
Keks, N; Hope, J; et al. “Switching and stopping antidepressants.” Australian Prescriber, June 2016. Accessed March 7, 2022.
Outhoff, K. “Switching antidepressants.” South African Family Practice, 2015. Accessed March 7, 2022.
Medical Disclaimer
The Recovery Village aims to improve the quality of life for people struggling with a substance use or mental health disorder with fact-based content about the nature of behavioral health conditions, treatment options and their related outcomes. We publish material that is researched, cited, edited and reviewed by licensed medical professionals. The information we provide is not intended to be a substitute for professional medical advice, diagnosis or treatment. It should not be used in place of the advice of your physician or other qualified healthcare provider.
How Long Does Effexor Stay in Your Urine, Blood, Hair and Saliva?
Effexor is a prescription medication that is used to treat depression, generalized anxiety disorder and social phobias.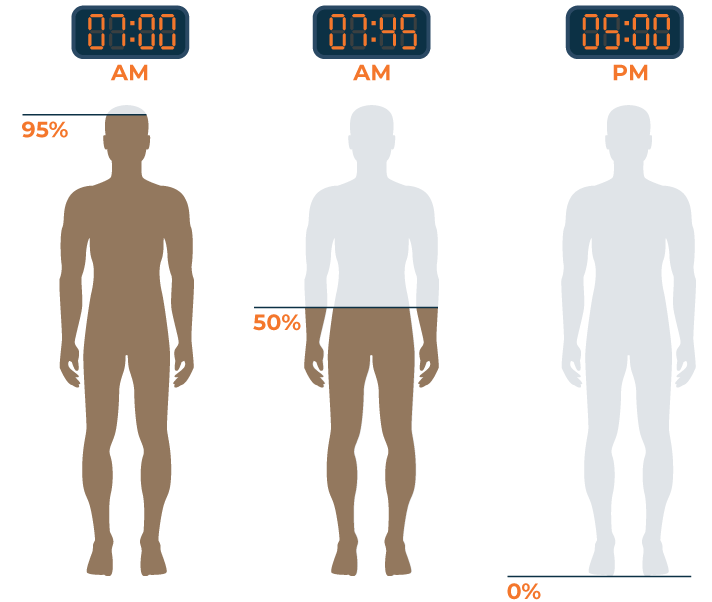 Also known by its generic name as venlafaxine, this drug is classified as a serotonin-norepinephrine reuptake inhibitor (SNRI), which works by helping to restore the balance of serotonin and norepinephrine in the brain. By doing this, a person diagnosed with depression may exhibit improved mood and energy levels.
Also known by its generic name as venlafaxine, this drug is classified as a serotonin-norepinephrine reuptake inhibitor (SNRI), which works by helping to restore the balance of serotonin and norepinephrine in the brain. By doing this, a person diagnosed with depression may exhibit improved mood and energy levels.
It is essential that you read the medication guide provided by your pharmacist before you start using Effexor. It should always be taken by mouth as directed by your doctor, usually two to three times daily with food. To reduce your risk of side effects, your doctor may start you out at a low dosage and gradually increase as you build a tolerance (it will range anywhere from 37.5 mg to 300 mg). It may take several weeks to feel the benefit of this medication, so be sure to take it every day around the same time for best results.
- Alventa XL
- Depefex X
- Effexor XL
- Politid XL
- Rodomel XL
- Sunveniz XL
- Tonpular XL
- Venaxx XL
- Vencarm XL
- Venlablue XL
- Venladex XL
- Venlalic XL
- Venlasov XL
- Vensir XL
- ViePax XL
Effexor works by enhancing the activity of the neurotransmitters serotonin and noradrenaline in the brain. These neurotransmitters are natural chemicals found in the body, and they act as chemical messengers between the nerve cells. Serotonin and noradrenaline are neurotransmitters that are involved in regulating emotions, mood and behavior — therefore, in people experiencing signs of depression and anxiety, there is generally less of these neurotransmitters released from nerve cells in the brain.
These neurotransmitters are natural chemicals found in the body, and they act as chemical messengers between the nerve cells. Serotonin and noradrenaline are neurotransmitters that are involved in regulating emotions, mood and behavior — therefore, in people experiencing signs of depression and anxiety, there is generally less of these neurotransmitters released from nerve cells in the brain.
Norepinephrine is a stress hormone, controlling parts of the brain related to attention and response and “fight or flight.” It also increases heart rate, triggers the release of glucose from energy stores and boosts blood flow to muscles. Serotonin controls other processes within the brain, including mood, emotions, anxiety, aggression, sleep, appetite, perceptions and memory. In other words, they play a critical role in maintaining a person’s well-being.
Venlafaxine works by preventing or inhibiting the reabsorption of these neurotransmitters — serotonin and noradrenaline — back into the nerve cells of the brain. Over time, this process helps to relieve depression, anxiety and fear. It does not, however, change your personality or make you feel like a new person. It simply works by getting you back to your normal self: the person you were before feeling crippled by fear and anxiety.
Over time, this process helps to relieve depression, anxiety and fear. It does not, however, change your personality or make you feel like a new person. It simply works by getting you back to your normal self: the person you were before feeling crippled by fear and anxiety.
Most people wonder how long it will take for a drug to fully leave their system. To determine how long Effexor stays in your system, it is necessary to understand the metabolite of its active ingredient: venlafaxine. You must first know about a drug’s half-life, which is the time taken for the plasma concentration to reduce to half its original value. The half-life of Effexor is approximately 5 hours (+/- 2 hours), which is extremely short compared to other antidepressants. It also means that if you took a 50-mg venlafaxine tablet at 5 pm, then by 10 pm, there would be 25 mg remaining in your system, and by 3 am, there would be 12.5 mg remaining in your system, and so on, until the tablet is fully cleared from your system.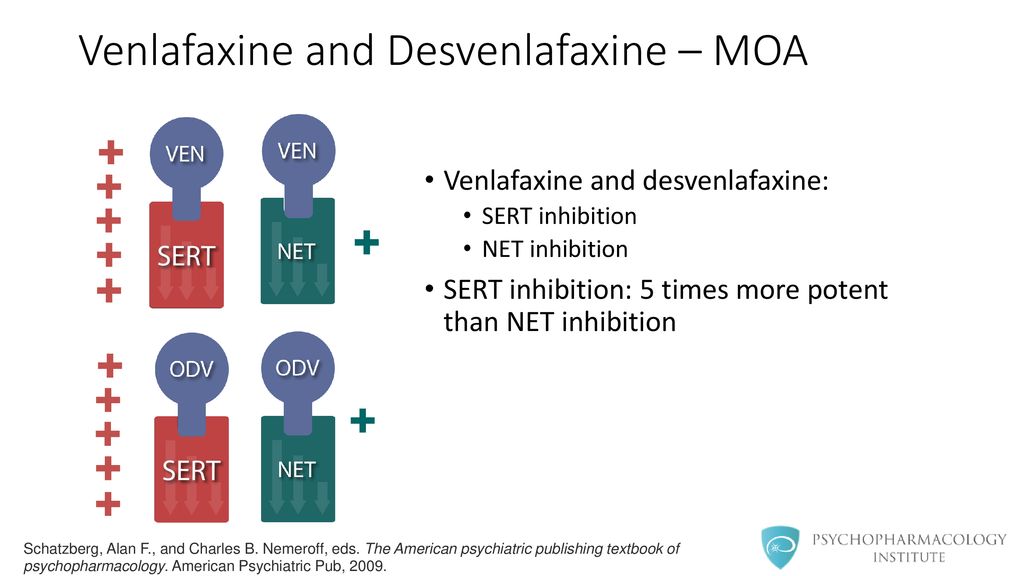
The overall average is around less than two days, though it depends on a variety of factors.
Individual factors such as age, body composition, genetics and liver function play a critical role in how long it takes to flush venlafaxine out of your system. This can explain why two people who take Effexor at the same dose, starting on the exact same day and quitting at the exact same time, will still not clear the drug at the same time.
Another factor is dosage. It is common knowledge that the greater the amount of a drug you ingest, the longer it will stay in your system. The person taking the lowest possible dose of Effexor a day will likely metabolize and excrete it quicker than someone taking the maximum dose. Though Venlafaxine doesn’t accumulate throughout tissues, high doses place a greater burden on the liver (for metabolism) and kidneys (for excretion). Since the body can only metabolize a certain amount of this drug at a time and the kidneys can only secrete a set amount at a time, those on greater doses will likely keep the drug in their systems longer.
There are also some drugs that interfere with metabolizing of Effexor, and they are known as “inducers” and “inhibitors.” Inhibitors tend to interfere with the enzyme that metabolizes venlafaxine, thus prolonging metabolism and excretion of the drug. Inducers, on the other hand, enhance activation of this enzyme, allowing for quicker metabolism and excretion of Effexor.
In regards to the factors above, we know that it can vary. However, to get the drug out of your system as quickly as possible, it is important to remember to stay hydrated, exercise and keep an acidic diet. The alkalinity of urine results in prolonged excretion and reabsorption of the drug. Manipulating your urinary pH to become more acidic through your diet could enhance the excretion of Effexor.
Read Previous
Effexor (Venlafaxine) Withdrawal Symptoms, Timeline and Detox
Read Next
What You Need to Know About Taking Effexor While Pregnant
Medical Disclaimer
The Recovery Village aims to improve the quality of life for people struggling with substance use or mental health disorder with fact-based content about the nature of behavioral health conditions, treatment options and their related outcomes. We publish material that is researched, cited, edited and reviewed by licensed medical professionals. The information we provide is not intended to be a substitute for professional medical advice, diagnosis or treatment. It should not be used in place of the advice of your physician or other qualified healthcare providers.
We publish material that is researched, cited, edited and reviewed by licensed medical professionals. The information we provide is not intended to be a substitute for professional medical advice, diagnosis or treatment. It should not be used in place of the advice of your physician or other qualified healthcare providers.
Antidepressants - stopstress.lv
- Antidepressants are taken only on prescription.
- These drugs are usually cleared from the body fairly quickly.
- These must be taken every day. Since the use of antidepressants, depending on the time of day, can change their effect on the body, it is necessary, if possible, to take antidepressants exactly at the time of day at which the doctor recommended you.
It is important to know that antidepressants are not addictive and are intended for long-term treatment. nine0009
Antidepressants, like other medications, have their side effects. The most common side effect that a patient may experience at the very beginning of treatment is loss of appetite and nausea.
 The mechanism of this side effect is well understood. Most antidepressants increase the amount of serotonin, which is the reason for the effect of normalizing mood and improving well-being. But since 90% of the body's serotonin receptors are located in the gastrointestinal tract, a too rapid increase in serotonin leads to irritation of these receptors in the first days of taking the medication. Within 1-2 weeks after starting the antidepressant, this side effect usually disappears spontaneously In almost all cases, nausea disappears quite quickly with a slower increase in doses of the drug at the very beginning of its use. There are extremely rare cases of intolerance to antidepressants, when nausea does not decrease and lasts more than two weeks, in these cases it is necessary to consult with your doctor. This side effect is in no way associated with any stomach disease and disappears completely without a trace when the drug is discontinued. nine0009
The mechanism of this side effect is well understood. Most antidepressants increase the amount of serotonin, which is the reason for the effect of normalizing mood and improving well-being. But since 90% of the body's serotonin receptors are located in the gastrointestinal tract, a too rapid increase in serotonin leads to irritation of these receptors in the first days of taking the medication. Within 1-2 weeks after starting the antidepressant, this side effect usually disappears spontaneously In almost all cases, nausea disappears quite quickly with a slower increase in doses of the drug at the very beginning of its use. There are extremely rare cases of intolerance to antidepressants, when nausea does not decrease and lasts more than two weeks, in these cases it is necessary to consult with your doctor. This side effect is in no way associated with any stomach disease and disappears completely without a trace when the drug is discontinued. nine0009 Another side effect that patients taking antidepressants should be informed about is various sexual dysfunctions.
 They appear in both men and women. The mechanism of this phenomenon is also well understood and is also associated with an increase in serotonin in the body. This phenomenon does not decrease and does not disappear with further use of antidepressants in the same doses, however, when the drug is discontinued, it disappears without a trace. In no case should you stop using the drug, but you should not continue to experience this side effect either. It is necessary to inform the attending physician about this in order to find the most suitable solution for this problem for you. Currently, there are many ways to deal with this. The doctor may suggest, for example, to change the dose of the drug, change the antidepressant, add other medications to reduce the manifestation of this side effect, or, in certain cases, in a stable state of health, on certain days will recommend that you stop using the medication, given that these days the effect side effects are greatly reduced. nine0009
They appear in both men and women. The mechanism of this phenomenon is also well understood and is also associated with an increase in serotonin in the body. This phenomenon does not decrease and does not disappear with further use of antidepressants in the same doses, however, when the drug is discontinued, it disappears without a trace. In no case should you stop using the drug, but you should not continue to experience this side effect either. It is necessary to inform the attending physician about this in order to find the most suitable solution for this problem for you. Currently, there are many ways to deal with this. The doctor may suggest, for example, to change the dose of the drug, change the antidepressant, add other medications to reduce the manifestation of this side effect, or, in certain cases, in a stable state of health, on certain days will recommend that you stop using the medication, given that these days the effect side effects are greatly reduced. nine0009 In patients with arterial hypertension, when taking antidepressants, blood pressure usually normalizes, and it may be necessary over time to reduce doses and even stop antihypertensive drugs.
 Although in rare cases, when taking certain antidepressants, an increase in blood pressure is also possible.
Although in rare cases, when taking certain antidepressants, an increase in blood pressure is also possible. If you are taking antidepressants and begin to notice swelling in the legs, weight gain, or uncharacteristic vivid dreams, then you need to pay attention to this doctor, as these manifestations, in all likelihood, may be associated with the use of these drugs. antidepressants due to the fact that when the condition improves, patients significantly decrease or even disappear anxiety and anxiety. And the body no longer burns calories, but begins to accumulate them, so it is necessary to monitor weight and calorie intake. nine0009
Antidepressants usually do not cause allergic reactions, and in the case of an allergy, another cause must be sought.
what are antidepressants and do you need them at all? / Habr
Depression is not only when you are sad all day and there is no desire to work. You may not know about it at all and be treated for another, not realizing that we are talking about a hormonal imbalance that can be corrected. And since going to a neurologist is “embarrassing,” there is every chance of living a long, miserable life with a lack of a couple of hormones. nine0009
And since going to a neurologist is “embarrassing,” there is every chance of living a long, miserable life with a lack of a couple of hormones. nine0009
About ten years ago, it was customary to hide any problems with the nervous system more complicated than a twitching eye. People almost with a false beard went to see a private psychiatrist on the other side of the city and were afraid that they would be registered, reported to work or relatives. Now, in my subjective opinion, the situation has begun to change for the better, and neurological disorders are less and less perceived as something shameful.
Today we're going to talk about depression, which isn't actually about being sad in any way. Disturbances in the synthesis, release and reuptake of neurotransmitters can manifest themselves not only in the desire to sit and watch the carpet all day long, but in completely sudden things like severe problems with the gastrointestinal tract, chronic pain and other things. nine0009
nine0009
With the invention of a wide variety of substances from the group of antidepressants, doctors have the opportunity to treat and significantly improve the quality of life of many patients who may not have guessed that their problems begin with the nervous system. But, as usual, even "magic pills" require very careful selection of the drug, dose and side effects. Today we will talk about how our synapses function, how the triad of key neurotransmitters affects our body, and which doctor to go to if something went wrong. nine0031
How synapses work
Nerve cells are very similar in concept to the quartz elements of a clock. They can generate electrical impulses by changing the concentration of ions outside and inside the cell membrane. Nevertheless, in the form of an electrical impulse, the signal is transmitted only within the framework of one element - the cell. To transmit a signal to the next neuron, you need a specific port (similar to USB) for interaction - a synapse.
Synapses are very different in structure and mechanism of action, but today we are interested in chemical synapses that use biogenic amines for signal transmission: serotonin, norepinephrine and dopamine. The neuron synthesizes them and stores them in special synaptic vesicles. In order to inform a neighboring cell about its excited status, a neuron must throw a neurotransmitter into the synaptic cleft - those same biogenic amines. As soon as the concentration of the neurotransmitter in the contact zone - the synaptic cleft - becomes sufficient, the receptors of the second neuron will begin to capture it, transmitting the chemical signal further. nine0009
It would be too expensive for the body to produce tons of conditional serotonin just like that, and besides that, it would also be harmful: the intercellular space would resemble a dump of neurotransmitters. That is why all the neurotransmitters that fell off the receptor after its activation and went back into the synaptic cleft are vacuumed back by the neuron using active reuptake pumps. The pumps consume some ATP, so it's much more economical than synthesizing a neurotransmitter molecule from scratch. The biogenic amines collected in this way can be recycled many times at minimal cost. nine0009
The pumps consume some ATP, so it's much more economical than synthesizing a neurotransmitter molecule from scratch. The biogenic amines collected in this way can be recycled many times at minimal cost. nine0009
If there is too much serotonin or dopamine, then a simple reuptake is no longer enough. This is where MAO, the enzyme monoamine oxidase, comes into play. He knows how to break down key neurotransmitters into their constituent fragments. MAO-A specializes mainly in epinephrine, norepinephrine, serotonin and histamine. MAO-B - on phenylethylamine and dopamine.
When everything is in order, the neurotransmitter is exactly as much as needed. Neurons produce it in the normal mode, slowly capture it back, use it again and destroy the excess. If the balance is shifted for various reasons, then the transfer of excitation to the neighboring neuron becomes difficult or, conversely, too intense. And that's when the problems begin. Let's take a closer look at the key triad of neurotransmitters. nine0009
nine0009
Serotonin
Serotonin molecule: the hormone of happiness, digestion and the feeling of unloading train cars at night. This amine has a huge number of physiological effects, not only in the central nervous system, but also on the periphery of the body. In particular, it is serotonin receptors that are one of the key in the regulation of intestinal motility, stimulating its activity and secretory activity. In part, this process is stimulated by the bacteria themselves, which can convert the amino acid, tryptophan, into serotonin with their enzymes - but this serotonin cannot enter the brain because of the barrier through which these large molecules do not pass. Therefore, simply adding tryptophan to food will not improve the situation. nine0009
In the CNS, this neurotransmitter plays a very important role in the regulation of pain sensitivity. With a decrease in its amount, the pain threshold is significantly reduced. This is one of the factors in the formation of a pronounced sensitivity to pain when a person is overtired. In addition, depending on its shortage or excess, human behavior changes greatly. If serotonin is conditionally low, then the person becomes depressed, apathetic and irritable. He is not sad, but rather "no way." At the same time, the mood is bad even when normally it would be worth rejoicing. Thus, one can sit sadly on a tropical island and munch fresh fruit in disgust under the rustle of the ocean. nine0009
In addition, depending on its shortage or excess, human behavior changes greatly. If serotonin is conditionally low, then the person becomes depressed, apathetic and irritable. He is not sad, but rather "no way." At the same time, the mood is bad even when normally it would be worth rejoicing. Thus, one can sit sadly on a tropical island and munch fresh fruit in disgust under the rustle of the ocean. nine0009
If there is little serotonin, then, upon waking up, one might think that there was no sleep, and all night you unloaded the wagons. There is no feeling of relaxation and freshness.
The reverse situation is also possible when there is a lot of serotonin. Most often, it occurs as a temporary side effect of antidepressants or as a result of the wrong combination of them. And then the opposite effect occurs. Hypomania sets in at first. She is pleasant. Very pleasant. The mood is abnormally good, even if there are no special prerequisites for this. You sit in a crowded office with the full feeling that you have been sent on vacation. Energy overflows, I want to do something actively. There is a feeling of incredible efficiency. The problem is that this efficiency is strongly reminiscent of the old joke. nine0009
Energy overflows, I want to do something actively. There is a feeling of incredible efficiency. The problem is that this efficiency is strongly reminiscent of the old joke. nine0009
A girl comes to get a job as a secretary.
The boss asks, “How fast can you type on a typewriter?”
Girl: "Well... 1000-1200 characters per minute."
Chief: "Is it possible to print at such a speed?"
Girl: “You can print, but it turns out such a game!”
Same here. Thousands of ideas are swarming in my head, but it all comes at the expense of a loss of criticality. What used to be discarded at the planning stage seems like a good option in a manic episode. In mild hypomania, this can even be a useful effect in solving creative problems. If hypomania turns into mania, then everything becomes bad: criticality is completely lost and a person can shave his head, paint his car pink and drive off into the sunset, and the like. In its most severe form, this can lead to serotonin syndrome with shaking hands, but along with euphoria, agitation, mania, hallucinations and coma in the final. nine0009
nine0009
Norepinephrine
Norepinephrine molecule
Norepinephrine is closely related to serotonin. They have very similar metabolic pathways, similar receptors and intracellular metabolism. This leads to the formation of a bunch of negative feedbacks between them, when one suppresses the effects of the other. For example, when taking antidepressants that increase serotonin and norepinephrine at the same time, at first there may be an imbalance between these neurotransmitters. Often, norepinephrine builds up faster than serotonin, and side effects like wet hands and feet and agitation begin to creep in. Then serotonin also rises to the desired level, and they again balance each other. nine0009
Norepinephrine also has the same effects as adrenaline, but from the side of the nervous system. When stressed, the adrenal glands release adrenaline into the blood, and you immediately feel this unpleasant feeling, as if everything in your stomach is shrinking and getting colder, your heart beats faster, your palms and feet become wet. This is a manifestation of humoral regulation. There is also neurogenic, which is realized through the sympathetic nervous system. Here, norepinephrine already ensures the functioning of synapses and the transmission of a signal from the central nervous system to organs. Nothing is thrown into the blood, and the effects are almost the same. nine0009
This is a manifestation of humoral regulation. There is also neurogenic, which is realized through the sympathetic nervous system. Here, norepinephrine already ensures the functioning of synapses and the transmission of a signal from the central nervous system to organs. Nothing is thrown into the blood, and the effects are almost the same. nine0009
Mentally, noradrenaline suppresses pain sensitivity, provides positive reinforcement and a sense of "victory", even if bleeding from a wound after a duel. The very stress against the backdrop of bright positive events, when emotions overwhelm.
It is this neurotransmitter that is the key target for a neurologist when a patient complains of chronic pain that is not relieved by conventional non-steroidal anti-inflammatory drugs.
Dopamine
Dopamine molecule
Mesocortical and mesolimbic pathways
Contrary to popular belief, dopamine does not produce feelings of pleasure on its own.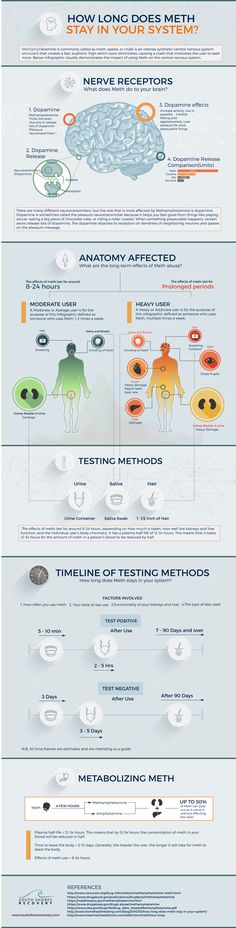 Current research suggests that it provides a sense of anticipation for the result that is about to be achieved. This is a very important mechanism. Without it, we would just sit in the corner and occasionally try to crawl away from whatever hurts. Almost any intrinsic motivation is somehow connected with this neurotransmitter. That is why it encourages us to perform evolutionarily fixed actions like sex, getting delicious food and other pleasures. This contributes to successful survival and reproduction. You take away dopamine and you get poorly breeding pandas who don't understand why they need this sex at all. nine0009
Current research suggests that it provides a sense of anticipation for the result that is about to be achieved. This is a very important mechanism. Without it, we would just sit in the corner and occasionally try to crawl away from whatever hurts. Almost any intrinsic motivation is somehow connected with this neurotransmitter. That is why it encourages us to perform evolutionarily fixed actions like sex, getting delicious food and other pleasures. This contributes to successful survival and reproduction. You take away dopamine and you get poorly breeding pandas who don't understand why they need this sex at all. nine0009
Neurobiological research suggests that dopamine is released not only when a pleasurable goal is achieved, but also when memories of past experiences are recalled. This allows you to firmly reinforce key memories and encourage the repetition of positive experiences. Unfortunately, it is this mechanism that underlies all addictions of a modern person. We suffer at the memory of juicy fat cheburek and dream of sweet chocolate cake, with a delicate layer of salted caramel, in the middle of the night. And we get drug addiction very quickly if the substance affects dopamine. So, for example, addiction to cocaine, which stimulates the release of norepinephrine and dopamine, is quickly formed. Invigorates, stimulates and very much praises for the next dose. After some time, it becomes more and more difficult for a person to refuse to receive a new dose of the drug, since his motivation system simply screams that he needs it. Moreover, such substances, when abused, can irreversibly break the motivation system as a whole, after which a person does not want anything but the next dose. nine0009
And we get drug addiction very quickly if the substance affects dopamine. So, for example, addiction to cocaine, which stimulates the release of norepinephrine and dopamine, is quickly formed. Invigorates, stimulates and very much praises for the next dose. After some time, it becomes more and more difficult for a person to refuse to receive a new dose of the drug, since his motivation system simply screams that he needs it. Moreover, such substances, when abused, can irreversibly break the motivation system as a whole, after which a person does not want anything but the next dose. nine0009
A rat presses a lever to release a dose of dopamine for a virtual reward
Most drugs that affect dopamine levels carry the risks of recreational use and addiction in one way or another. Therefore, the same amphetamine derivatives are banned in many countries, although they can be used as a medicine under strict control for certain pathologies.
In addition to the motivation system and the emotional sphere, dopamine regulates automatic motor activity. These are movements that we perform unconsciously, such as maintaining a posture, rearranging our legs in the right order when walking, and so on. nine0009
These are movements that we perform unconsciously, such as maintaining a posture, rearranging our legs in the right order when walking, and so on. nine0009
With its lack, we get parkinsonism. Outwardly, this is very similar to the behavior of some older people: stiffness of movements, lethargy, shuffling gait, tremor of the limbs. With excessive stimulation, on the contrary, involuntary grimaces, obsessive muscle movements.
In general, due to the peculiarities of the physiological effects of dopamine, neurologists and psychiatrists try not to touch it without a strong need, limiting themselves to more selective drugs.
So everything is broken
For starters, don't get discouraged. There is nothing to be ashamed of. A person with equal success may experience gastritis, acute hemorrhoids or clinical depression. The brain is also an organ and can get sick. For some reason, with gastritis, we already calmly go to the gastroenterologist, we try not to mention visits to the proctologist once again, and we often don’t even talk about neurological treatment even to close people. This is a very big mistake, since it is the help of a loved one from the outside that can greatly help the treatment. nine0009
This is a very big mistake, since it is the help of a loved one from the outside that can greatly help the treatment. nine0009
What kind of depression is it? It can be depression provoked by some external traumatic factor. It is completely natural to be depressed for a while, having experienced the loss of a loved one or losing your job. In such cases, there is a clear connection between the external factor and the state of the person. As a rule, this should pass by itself, as soon as the external traumatic factor loses its relevance. In this case, the neurologist, most likely, will be able to help only slightly extinguish anxiety and negative emotions with anxiolytics. nine0009
Sometimes the cause of depression cannot be found. Everything seems to be fine, there is work, the family loves, and the patient sits and watches the carpet. One of the main theories of the last century suggests that there is such a type of depression as endogenous, associated with a lack of norepinephrine, serotonin and dopamine. Nevertheless, now such a term does not exist, and modern research does not allow us to reliably state that the reason is strictly related precisely to the lack of serotonin that has come from nowhere. And usually there is a factor that provokes this lack: lack of sleep, a large amount of work, a constant focus on a large number of details, 24-hour stress resistance. And with all this - the impossibility and lack of time to restore strength. nine0009
Nevertheless, now such a term does not exist, and modern research does not allow us to reliably state that the reason is strictly related precisely to the lack of serotonin that has come from nowhere. And usually there is a factor that provokes this lack: lack of sleep, a large amount of work, a constant focus on a large number of details, 24-hour stress resistance. And with all this - the impossibility and lack of time to restore strength. nine0009
Depression is characterized by the classic triad:
- Asthenia - weakness, increased fatigue, which does not go away for a long time.
- Apathy is a detached emotional state, when neither good nor bad.
- Anhedonia - the inability to rejoice in what used to please. This state includes the reluctance to have sex, the reluctance to please yourself with your favorite dish or your favorite trip to the theater.
Very often, this condition can progress slowly, over months, and be invisible from the inside. It is worth listening to your loved ones if they say that you have changed a lot and become somehow bleak and withdrawn. It's time to go to the doctor for a consultation. nine0009
It is worth listening to your loved ones if they say that you have changed a lot and become somehow bleak and withdrawn. It's time to go to the doctor for a consultation. nine0009
How to diagnose depression
As I said, the main problem of depressive states is that they are very difficult to recognize from the inside. This is the classic problem of a crowbar to open a box that lies inside the box.
It is extremely rare that a person will come with the words “I have depression”. Or "I have anxiety." Most often, he will talk about memory loss, a decrease in concentration, an internal feeling of anxiety or a feeling of a “tight string”. He will tell that he cannot fall asleep at night, simply because there are a lot of thoughts in his head. He will complain that during the descent on the escalator his head began to spin and there is a feeling of fear that he will not stay on his feet. nine0009
If you have a suspicion that something is wrong with you emotionally, you can try the classic Beck questionnaire. It was developed in 1961 and is still considered one of the main tools in the diagnosis of depression. Also, the reason for self-diagnosis can be not only a psychological condition, but also some chronic conditions that cannot be treated with standard therapy. For example, various variants of chronic pain syndrome that make the patient go in circles from the urologist to the proctologist in search of a problem that has a neurological cause. nine0009
It was developed in 1961 and is still considered one of the main tools in the diagnosis of depression. Also, the reason for self-diagnosis can be not only a psychological condition, but also some chronic conditions that cannot be treated with standard therapy. For example, various variants of chronic pain syndrome that make the patient go in circles from the urologist to the proctologist in search of a problem that has a neurological cause. nine0009
As I said above, neurotransmitters are not only about sad/happy, but also about the direct regulation of the functions of internal organs due to the autonomic nervous system. Neurological changes associated with biogenic amines can cause gastrointestinal disturbances: nausea, constipation, or vice versa diarrhea.
Antidepressants
If the patient does go to the neurologist, the doctor may find it necessary to prescribe antidepressants. There is no need to be afraid of this group of drugs: this is a huge class of substances that can effectively help in the treatment of neurological and somatic disorders.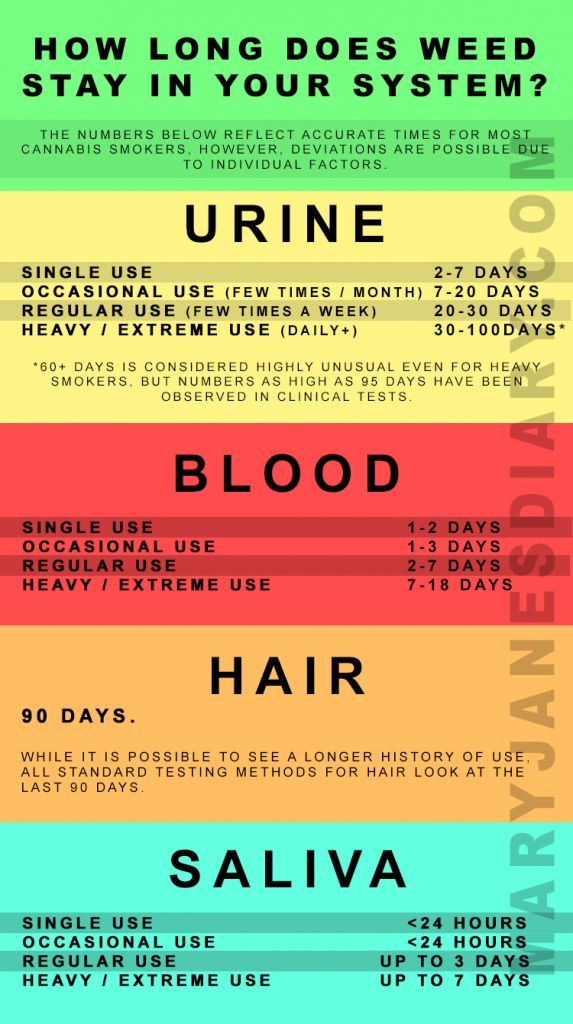 nine0009
nine0009
Above, we have already analyzed the ways of reuptake and destruction of excess neurotransmitters. If their regulatory mechanisms have failed, then the appointment of antidepressants can help solve this problem.
Non-selective MAO inhibitors
Older and less selective classes of antidepressants inhibit MAO - monoamine oxidase. As a result, excess biogenic amines begin to accumulate, and their concentration in the synaptic cleft begins to grow. This non-selectivity leads to a large number of side effects in comparison with modern narrow groups. Currently, this group of drugs is not used as the first line. That is, therapy will definitely not begin with it. There are more effective groups with fewer side effects. nine0009
Neurotransmitter reuptake inhibitors
Current classes of antidepressants tend to work by inhibiting the reuptake of neurotransmitters without interfering with the utilization of the excess throughout the body. There are both non-selective tricyclic antidepressants, which simultaneously block the capture of all three neurotransmitters, and selective ones, which selectively block the capture of one or two neurotransmitters.
There are both non-selective tricyclic antidepressants, which simultaneously block the capture of all three neurotransmitters, and selective ones, which selectively block the capture of one or two neurotransmitters.
A representative non-selective reuptake inhibitor is amitriptyline. It was originally used to treat severe depression, but has been superseded by more modern drugs for many cases. Although it still works great in small doses in the treatment of chronic pain syndromes:
- Tension headache.
- Migraine.
- Neuropathic pain.
- Chronic pain in cancer patients.
- Rheumatic pains.
Selective ones are divided depending on the neurotransmitter whose concentration they increase:
- SSRIs - serotonin.
- SSRIs - serotonin + norepinephrine.
The doctor selects the best option depending on the clinical situation and then monitors the patient's condition, adjusting the dose and, possibly, the drug itself. In the treatment of pain syndromes, drugs that increase the level of norepinephrine are most often used. They are more likely to cause negative side effects than SSRIs, but are much more effective in treating pain. nine0009
In the treatment of pain syndromes, drugs that increase the level of norepinephrine are most often used. They are more likely to cause negative side effects than SSRIs, but are much more effective in treating pain. nine0009
Anxiety disorders
Very often, patients come with a complex complex problem, and not depression in its purest form. This includes various types of anxiety disorders, which are also treated with SSRI antidepressants, but, as we remember, they do not start working immediately. Therefore, in the treatment of such patients, it is most often necessary to start work with lowering anxiety using anxiolytics (they are also tranquilizers).
Also, antidepressants often have an increase in anxiety in the first 1-2 weeks, as a manifestation of one of the side effects. So imagine. nine0009
A person has anxiety, possibly panic attacks, but at the same time he is constrained by a depressive state. He sits in a corner and suffers in silence. You can't just take and give him an antidepressant. If he has a severe anxiety disorder, then on an antidepressant, his anxiety and motor activity may become even more active, and he will have the strength to do something. What is most unpleasant is that there will be strength to do the wrong things, which in the end can even lead to suicide.
You can't just take and give him an antidepressant. If he has a severe anxiety disorder, then on an antidepressant, his anxiety and motor activity may become even more active, and he will have the strength to do something. What is most unpleasant is that there will be strength to do the wrong things, which in the end can even lead to suicide.
Therefore, the first time such patients are usually covered with anxiolytics. And they are watching closely. When anxiety goes away, they begin to gradually withdraw from the state of depression and return to normal activity. nine0009
It is reasonable to ask a question: why not just prescribe anxiolytics to everyone, since they have fewer side effects and the effect comes faster? Anxiolytics do not affect serotonin, they temporarily suppress anxiety, but do not repair this complex mechanism of serotonin metabolism. And more often than not, they are addictive. Therefore, they cover the intake of antidepressants for the first time - 2-3 weeks, no more.
Terminals
The most important thing is that you don’t have to sit and watch the carpet, closed in on your problem. Almost always, the problem can be solved with the right selection of drugs. But there are a few important points:
- I'll have to go to a neurologist. It is possible that a neurologist can refer you to a psychiatrist if you need clarification on the diagnosis and the appointment of different combinations of drugs. This is normal, there is no need to be afraid of this.
- Any psychotropic drugs should be taken strictly according to the scheme agreed with the attending physician. Usually the doctor explains how to carefully adjust the dose of treatment depending on how you feel.
- Tune in to the fact that there will be no quick result. Anxiety with anxiolytics is usually removed quite quickly, but the repair of these components - anxiety and depression - is months of therapy with a possible change or reselection of the drug.
 Typical waiting times: first effects after 7-14 days, initial evaluation of effectiveness - 3 months. The duration of the course is at least 6 months, more often longer. nine0004
Typical waiting times: first effects after 7-14 days, initial evaluation of effectiveness - 3 months. The duration of the course is at least 6 months, more often longer. nine0004 - Antidepressants should not be abruptly discontinued, like any psychotropic drugs. Withdrawal and side effects can be very severe. Only a very slow dose reduction under the supervision of a doctor and, possibly, with an anxiolytic cover.
- Hence the consequence is to always have a supply of the drug with you. In no case should you be left without medicine while traveling or on vacation. When flying overseas, take a prescription from your doctor if asked. Abroad, there is a different attitude towards antidepressants - in the pharmacy they are released calmly and with understanding. nine0004
- Many antidepressants like fluvoxamine are completely incompatible with alcohol. Even just a little. Side effects can be the most unpredictable, up to trying to catch leprechauns in the night park and leaving for the next world.
- Keep a mood diary. It can be paper, it can be in the form of an application. This will help you with dose adjustments and your doctor to evaluate the effectiveness. From time to time, you can take the Beck questionnaire.
- If the therapy was correct, was not interrupted prematurely, then the remission can be very long, without repeated episodes of depression. nine0004
- Let there always be someone close, or rather a specialist, who is aware of your problem. That makes it much easier to deal with it.
Thanks to edogs for the nice comment about transporting drugs across the border:
When flying abroad, and abroad, you really need to remember about the attitude towards antidepressants in particular and prescription drugs in general.
But it is not enough just to "take the recipe" and "show if asked" relying on the "kindness of foreign countries." nine0031 When crossing the border, you must definitely go through the red corridor and declare.At the same time, a certified doctor's prescription and a certified copy of the prescription (if it is one-time) must be presented and they must be translated into at least English, and at most be in the language of the countries from/where you are flying to. The recipe itself should contain the name of the active substance (and not the branded name) in Latin. Moreover, before the trip, it would be nice to check whether this drug is allowed in the country of destination in principle, if not, you cannot enter with it even if you have all the papers. In addition, there is often a requirement to have a supply of no more than 1 month / 1 course. nine0031 Yes, in most cases it will “carry over”, because. Customs officers rarely check pills unless they are transported in bulk. But if they suddenly check or the detectors catch or the dogs sniff out, the consequences can be very serious. And not only in Thailand and the Emirates (where landing is almost guaranteed, but in completely innocent countries such as Bulgaria, Estonia, Turkey, Belarus (sic!), Germany, etc.