Grieving coping mechanisms
SAMHSA’s National Helpline | SAMHSA
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Main page content
-
SAMHSA’s National Helpline is a free, confidential, 24/7, 365-day-a-year treatment referral and information service (in English and Spanish) for individuals and families facing mental and/or substance use disorders.
Also visit the online treatment locator.
SAMHSA’s National Helpline, 1-800-662-HELP (4357) (also known as the Treatment Referral Routing Service), or TTY: 1-800-487-4889 is a confidential, free, 24-hour-a-day, 365-day-a-year, information service, in English and Spanish, for individuals and family members facing mental and/or substance use disorders.
This service provides referrals to local treatment facilities, support groups, and community-based organizations.
Also visit the online treatment locator, or send your zip code via text message: 435748 (HELP4U) to find help near you. Read more about the HELP4U text messaging service.
The service is open 24/7, 365 days a year.
English and Spanish are available if you select the option to speak with a national representative. Currently, the 435748 (HELP4U) text messaging service is only available in English.
In 2020, the Helpline received 833,598 calls. This is a 27 percent increase from 2019, when the Helpline received a total of 656,953 calls for the year.
The referral service is free of charge. If you have no insurance or are underinsured, we will refer you to your state office, which is responsible for state-funded treatment programs. In addition, we can often refer you to facilities that charge on a sliding fee scale or accept Medicare or Medicaid.![]() If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
If you have health insurance, you are encouraged to contact your insurer for a list of participating health care providers and facilities.
The service is confidential. We will not ask you for any personal information. We may ask for your zip code or other pertinent geographic information in order to track calls being routed to other offices or to accurately identify the local resources appropriate to your needs.
No, we do not provide counseling. Trained information specialists answer calls, transfer callers to state services or other appropriate intake centers in their states, and connect them with local assistance and support.
-
Suggested Resources
What Is Substance Abuse Treatment? A Booklet for Families
Created for family members of people with alcohol abuse or drug abuse problems. Answers questions about substance abuse, its symptoms, different types of treatment, and recovery. Addresses concerns of children of parents with substance use/abuse problems.
Addresses concerns of children of parents with substance use/abuse problems.It's Not Your Fault (NACoA) (PDF | 12 KB)
Assures teens with parents who abuse alcohol or drugs that, "It's not your fault!" and that they are not alone. Encourages teens to seek emotional support from other adults, school counselors, and youth support groups such as Alateen, and provides a resource list.After an Attempt: A Guide for Taking Care of Your Family Member After Treatment in the Emergency Department
Aids family members in coping with the aftermath of a relative's suicide attempt. Describes the emergency department treatment process, lists questions to ask about follow-up treatment, and describes how to reduce risk and ensure safety at home.Family Therapy Can Help: For People in Recovery From Mental Illness or Addiction
Explores the role of family therapy in recovery from mental illness or substance abuse. Explains how family therapy sessions are run and who conducts them, describes a typical session, and provides information on its effectiveness in recovery.
For additional resources, please visit the SAMHSA Store.
Last Updated: 08/30/2022
Alcohol, Tobacco, and Other Drugs
Your browser is not supported
Switch to Chrome, Edge, Firefox or Safari
Misusing alcohol, tobacco, and other drugs can have both immediate and long-term health effects.The misuse and abuse of alcohol, tobacco, illicit drugs, and prescription medications affect the health and well-being of millions of Americans. NSDUH estimates allow researchers, clinicians, policymakers, and the general public to better understand and improve the nation’s behavioral health. These reports and detailed tables present estimates from the 2021 National Survey on Drug Use and Health (NSDUH).
Alcohol
Data:
- Among the 133.1 million current alcohol users aged 12 or older in 2021, 60.0 million people (or 45.1%) were past month binge drinkers.
 The percentage of people who were past month binge drinkers was highest among young adults aged 18 to 25 (29.2% or 9.8 million people), followed by adults aged 26 or older (22.4% or 49.3 million people), then by adolescents aged 12 to 17 (3.8% or 995,000 people). (2021 NSDUH)
The percentage of people who were past month binge drinkers was highest among young adults aged 18 to 25 (29.2% or 9.8 million people), followed by adults aged 26 or older (22.4% or 49.3 million people), then by adolescents aged 12 to 17 (3.8% or 995,000 people). (2021 NSDUH) - Among people aged 12 to 20 in 2021, 15.1% (or 5.9 million people) were past month alcohol users. Estimates of binge alcohol use and heavy alcohol use in the past month among underage people were 8.3% (or 3.2 million people) and 1.6% (or 613,000 people), respectively. (2021 NSDUH)
- In 2020, 50.0% of people aged 12 or older (or 138.5 million people) used alcohol in the past month (i.e., current alcohol users) (2020 NSDUH)
- Among the 138.5 million people who were current alcohol users, 61.6 million people (or 44.4%) were classified as binge drinkers and 17.7 million people (28.8% of current binge drinkers and 12.8% of current alcohol users) were classified as heavy drinkers (2020 NSDUH)
- The percentage of people who were past month binge alcohol users was highest among young adults aged 18 to 25 (31.
 4%) compared with 22.9% of adults aged 26 or older and 4.1% of adolescents aged 12 to 17 (2020 NSDUH)
4%) compared with 22.9% of adults aged 26 or older and 4.1% of adolescents aged 12 to 17 (2020 NSDUH) - Excessive alcohol use can increase a person’s risk of stroke, liver cirrhosis, alcoholic hepatitis, cancer, and other serious health conditions
- Excessive alcohol use can also lead to risk-taking behavior, including driving while impaired. The Centers for Disease Control and Prevention reports that 29 people in the United States die in motor vehicle crashes that involve an alcohol-impaired driver daily
Programs/Initiatives:
- STOP Underage Drinking interagency portal - Interagency Coordinating Committee on the Prevention of Underage Drinking
- Interagency Coordinating Committee on the Prevention of Underage Drinking
- Talk. They Hear You.
- Underage Drinking: Myths vs. Facts
- Talking with your College-Bound Young Adult About Alcohol
Relevant links:
- National Association of State Alcohol and Drug Abuse Directors
- Department of Transportation Office of Drug & Alcohol Policy & Compliance
- Alcohol Policy Information Systems Database (APIS)
- National Institute on Alcohol Abuse and Alcoholism
Tobacco
Data:
- In 2020, 20.
 7% of people aged 12 or older (or 57.3 million people) used nicotine products (i.e., used tobacco products or vaped nicotine) in the past month (2020 NSDUH)
7% of people aged 12 or older (or 57.3 million people) used nicotine products (i.e., used tobacco products or vaped nicotine) in the past month (2020 NSDUH) - Among past month users of nicotine products, nearly two thirds of adolescents aged 12 to 17 (63.1%) vaped nicotine but did not use tobacco products. In contrast, 88.9% of past month nicotine product users aged 26 or older used only tobacco products (2020 NSDUH)
- Tobacco use is the leading cause of preventable death, often leading to lung cancer, respiratory disorders, heart disease, stroke, and other serious illnesses. The CDC reports that cigarette smoking causes more than 480,000 deaths each year in the United States
- The CDC’s Office on Smoking and Health reports that more than 16 million Americans are living with a disease caused by smoking cigarettes
Electronic cigarette (e-cigarette) use data:
- In 2021, 13.2 million people aged 12 or older (or 4.7%) used an e-cigarette or other vaping device to vape nicotine in the past month.
 The percentage of people who vaped nicotine was highest among young adults aged 18 to 25 (14.1% or 4.7 million people), followed by adolescents aged 12 to 17 (5.2% or 1.4 million people), then by adults aged 26 or older (3.2% or 7.1 million people).
The percentage of people who vaped nicotine was highest among young adults aged 18 to 25 (14.1% or 4.7 million people), followed by adolescents aged 12 to 17 (5.2% or 1.4 million people), then by adults aged 26 or older (3.2% or 7.1 million people). - Among people aged 12 to 20 in 2021, 11.0% (or 4.3 million people) used tobacco products or used an e-cigarette or other vaping device to vape nicotine in the past month. Among people in this age group, 8.1% (or 3.1 million people) vaped nicotine, 5.4% (or 2.1 million people) used tobacco products, and 3.4% (or 1.3 million people) smoked cigarettes in the past month. (2021 NSDUH)
- Data from the Centers for Disease Control and Prevention’s 2020 National Youth Tobacco Survey. Among both middle and high school students, current use of e-cigarettes declined from 2019 to 2020, reversing previous trends and returning current e-cigarette use to levels similar to those observed in 2018
- E-cigarettes are not safe for youth, young adults, or pregnant women, especially because they contain nicotine and other chemicals
Resources:
- Tips for Teens: Tobacco
- Tips for Teens: E-cigarettes
- Implementing Tobacco Cessation Programs in Substance Use Disorder Treatment Settings
- Synar Amendment Program
Links:
- Truth Initiative
- FDA Center for Tobacco Products
- CDC Office on Smoking and Health
- National Institute on Drug Abuse: Tobacco, Nicotine, and E-Cigarettes
- National Institute on Drug Abuse: E-Cigarettes
Opioids
Data:
- Among people aged 12 or older in 2021, 3.
 3% (or 9.2 million people) misused opioids (heroin or prescription pain relievers) in the past year. Among the 9.2 million people who misused opioids in the past year, 8.7 million people misused prescription pain relievers compared with 1.1 million people who used heroin. These numbers include 574,000 people who both misused prescription pain relievers and used heroin in the past year. (2021 NSDUH)
3% (or 9.2 million people) misused opioids (heroin or prescription pain relievers) in the past year. Among the 9.2 million people who misused opioids in the past year, 8.7 million people misused prescription pain relievers compared with 1.1 million people who used heroin. These numbers include 574,000 people who both misused prescription pain relievers and used heroin in the past year. (2021 NSDUH) - Among people aged 12 or older in 2020, 3.4% (or 9.5 million people) misused opioids in the past year. Among the 9.5 million people who misused opioids in the past year, 9.3 million people misused prescription pain relievers and 902,000 people used heroin (2020 NSDUH)
- According to the Centers for Disease Control and Prevention’s Understanding the Epidemic, an average of 128 Americans die every day from an opioid overdose
Resources:
- Medication-Assisted Treatment
- Opioid Overdose Prevention Toolkit
- TIP 63: Medications for Opioid Use Disorder
- Use of Medication-Assisted Treatment for Opioid Use Disorder in Criminal Justice Settings
- Opioid Use Disorder and Pregnancy
- Clinical Guidance for Treating Pregnant and Parenting Women With Opioid Use Disorder and Their Infants
- The Facts about Buprenorphine for Treatment of Opioid Addiction
- Pregnancy Planning for Women Being Treated for Opioid Use Disorder
- Tips for Teens: Opioids
- Rural Opioid Technical Assistance Grants
- Tribal Opioid Response Grants
- Provider’s Clinical Support System - Medication Assisted Treatment Grant Program
Links:
- National Institute on Drug Abuse: Opioids
- National Institute on Drug Abuse: Heroin
- HHS Prevent Opioid Abuse
- Community Anti-Drug Coalitions of America
- Addiction Technology Transfer Center (ATTC) Network
- Prevention Technology Transfer Center (PTTC) Network
Marijuana
Data:
- In 2021, marijuana was the most commonly used illicit drug, with 18.
 7% of people aged 12 or older (or 52.5 million people) using it in the past year. The percentage was highest among young adults aged 18 to 25 (35.4% or 11.8 million people), followed by adults aged 26 or older (17.2% or 37.9 million people), then by adolescents aged 12 to 17 (10.5% or 2.7 million people).
7% of people aged 12 or older (or 52.5 million people) using it in the past year. The percentage was highest among young adults aged 18 to 25 (35.4% or 11.8 million people), followed by adults aged 26 or older (17.2% or 37.9 million people), then by adolescents aged 12 to 17 (10.5% or 2.7 million people). - The percentage of people who used marijuana in the past year was highest among young adults aged 18 to 25 (34.5%) compared with 16.3% of adults aged 26 or older and 10.1% of adolescents aged 12 to 17 (2020 NSDUH)
- Marijuana can impair judgment and distort perception in the short term and can lead to memory impairment in the long term
- Marijuana can have significant health effects on youth and pregnant women.
Resources:
- Know the Risks of Marijuana
- Marijuana and Pregnancy
- Tips for Teens: Marijuana
Relevant links:
- National Institute on Drug Abuse: Marijuana
- Addiction Technology Transfer Centers on Marijuana
- CDC Marijuana and Public Health
Emerging Trends in Substance Misuse:
- Methamphetamine—In 2019, NSDUH data show that approximately 2 million people used methamphetamine in the past year.
 Approximately 1 million people had a methamphetamine use disorder, which was higher than the percentage in 2016, but similar to the percentages in 2015 and 2018. The National Institute on Drug Abuse Data shows that overdose death rates involving methamphetamine have quadrupled from 2011 to 2017. Frequent meth use is associated with mood disturbances, hallucinations, and paranoia.
Approximately 1 million people had a methamphetamine use disorder, which was higher than the percentage in 2016, but similar to the percentages in 2015 and 2018. The National Institute on Drug Abuse Data shows that overdose death rates involving methamphetamine have quadrupled from 2011 to 2017. Frequent meth use is associated with mood disturbances, hallucinations, and paranoia. - Cocaine—In 2019, NSDUH data show an estimated 5.5 million people aged 12 or older were past users of cocaine, including about 778,000 users of crack. The CDC reports that overdose deaths involving have increased by one-third from 2016 to 2017. In the short term, cocaine use can result in increased blood pressure, restlessness, and irritability. In the long term, severe medical complications of cocaine use include heart attacks, seizures, and abdominal pain.
- Kratom—In 2019, NSDUH data show that about 825,000 people had used Kratom in the past month. Kratom is a tropical plant that grows naturally in Southeast Asia with leaves that can have psychotropic effects by affecting opioid brain receptors.
 It is currently unregulated and has risk of abuse and dependence. The National Institute on Drug Abuse reports that health effects of Kratom can include nausea, itching, seizures, and hallucinations.
It is currently unregulated and has risk of abuse and dependence. The National Institute on Drug Abuse reports that health effects of Kratom can include nausea, itching, seizures, and hallucinations.
Resources:
- Tips for Teens: Methamphetamine
- Tips for Teens: Cocaine
- National Institute on Drug Abuse
More SAMHSA publications on substance use prevention and treatment.
Last Updated: 01/05/2023
Five stages of grief. The Rise and Fall of Kübler-Ross
- Lucy Burns
- BBC
Image copyright Getty Images
Denial. Anger. Finding a compromise. Despair. Adoption. Many people know the theory according to which grief, when receiving unbearable information for a person, goes through these steps. The scope of its application is wide: from hospices to boards of directors of companies. nine0018
nine0018
A recent interview with a psychologist in English on the Internet proves that the perception of the current quarantine is subject to the same rules. But do we all experience the same?
When Swiss psychiatrist Elisabeth Kübler-Ross began working in American hospitals in 1958, she was struck by the lack of methods of psychological care for dying patients.
- A method that can predict your death
"Everything was impersonal, the attention was paid exclusively to the technical side of things," she told the BBC at 1983 year. “Terminally ill patients were left to their own devices, no one talked to them.”
She started a workshop with Colorado State University medical students based on her conversations with cancer patients about what they thought and felt.
Author photo, LIFE/Getty Images
Photo caption, Elisabeth Kübler-Ross talks to a woman with leukemia in Chicago, 1969. Seminar participants observe through a special mirror glass
Seminar participants observe through a special mirror glass
Despite the misunderstanding and resistance of a number of colleagues, soon there was nowhere for an apple to fall at the Kübler-Ross seminars.
In 1969 she published a book, On Death and Dying, in which she quoted typical statements from her patients and then moved on to discuss how to help doomed people pass from life as free of fear and pain as possible.
Kübler-Ross described in detail the five emotional states that a person goes through after being diagnosed with a terminal diagnosis:
- Denial: "No, that can't be true"
- Anger: "Why me? Why? It's not fair!!!"
- Bargaining: "There must be a way to save myself, or at least improve my situation! I'll think of something, I'll behave properly and do whatever is necessary!"
- Depression: "There is no way out, everything is indifferent"
- Acceptance: "Well, we must somehow live with this and prepare for the last journey"
difficult situation. nine0011
nine0011
A separate chapter of the book is devoted to each of the stages. In addition to the five main ones, the author identified intermediate states - the first shock, preliminary grief, hope - from 10 to 13 types in total.
Image copyright Getty Images
Elisabeth Kübler-Ross died in 2004. Her son, Ken Ross, says she never insisted that every person must go through these five stages in sequence.
"It was a flexible framework, not a panacea for dealing with grief. If people wanted to use other theories and models, the mother did not object. She wanted to start a discussion of the topic first," he says. nine0011
- Last will: how did the photo of a dying American touch the world?
- "You hear everything, Fernando." How was the evening in honor of the terminally ill football player
The book "On Death and Dying" became a bestseller, and Elisabeth Kübler-Ross was soon inundated with letters from patients and doctors from all over the world.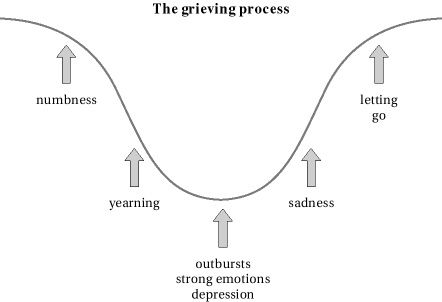
"The phone kept ringing, and the postman started visiting us twice a day," recalls Ken Ross.
The notorious five steps took on a life of their own. Following the doctors, patients and their relatives learned about them. They were mentioned by the characters of the series "Star Trek" and "Sesame Street". They were parodied in cartoons, they gave food for creativity to the mass of musicians and artists and gave rise to many successful memes. nine0011
Literally thousands of scientific papers have been written that have applied the theory of the five steps to a wide variety of people and situations, from athletes suffering career-incompatible injuries to Apple fans' worries about the release of the 5th iPhone.
Image copyright, Getty Images
Skip the Podcast and continue reading.
Podcast
What was that?
We quickly, simply and clearly explain what happened, why it's important and what's next.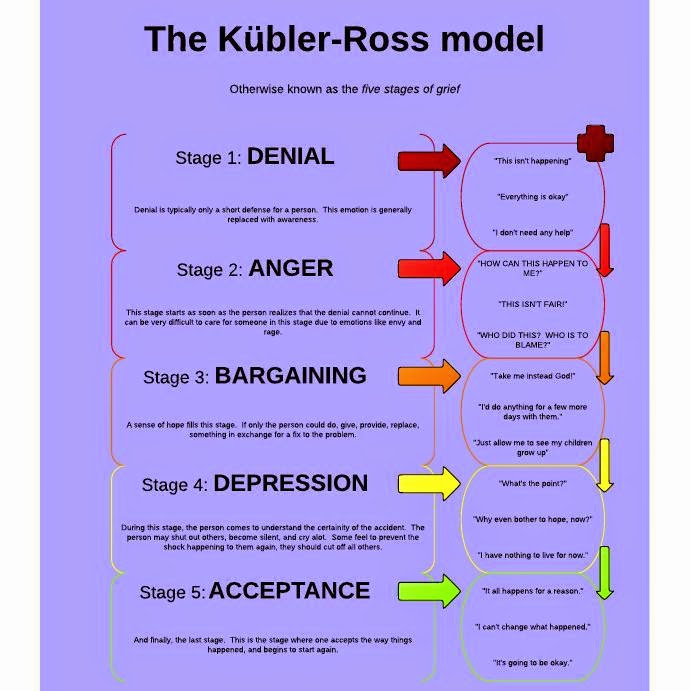 nine0011
nine0011
episodes
The End of History Podcast
Kübler-Ross's legacy has found its way into corporate governance: Big companies from Boeing to IBM (including the BBC) have used her "change curve" to help employees at times of great business change.
And during the coronavirus pandemic, it applies, says psychologist David Kessler.
Kessler worked with Elisabeth Kübler-Ross and co-authored her latest book, Grief and How We Grieve. His interview with the Harvard Business Review at the start of the pandemic garnered a lot of attention online as people everywhere searched for solutions to their emotional problems. nine0011
"And here, first comes denial: the virus is not terrible, nothing will happen to me. Then anger: who dares to deprive me of my usual life and force me to stay at home?! Then an attempt to find a compromise: okay, if after two weeks of social distancing it gets better, then why not? Followed by sadness: no one knows when it will end. And, finally, acceptance: the world is now like this, you have to somehow live with it, "describes David Kessler.
And, finally, acceptance: the world is now like this, you have to somehow live with it, "describes David Kessler.
"As you can see, strength comes with acceptance. It gives you control: I can wash my hands, I can keep a safe distance, I can work from home," he says. nine0011
"It's a roadmap," says George Bonanno, professor of clinical psychology and head of the Loss, Trauma, and Emotion Laboratory at Columbia University. "When people are in pain, they want to know: how long will it last? What will happen to me? something to grab on to. And the five-step model gives them that opportunity."
"This scheme is seductive," notes Charles Corr, social psychologist and author of Death and Dying, Life and Being. "It offers an easy solution: sort everyone, and it takes no more than the fingers of one hand to label each one." . nine0011
George Bonanno sees this as a possible harm.
"People who don't fit exactly into these stages - and I've seen the majority of them - may decide they're grieving the wrong way, so to speak," he explains.
According to him, over the years he has seen many cases when people themselves inspired that they must certainly experience this and that, or they were convinced of this by friends and relatives, but they did not feel it and decided, that they need a doctor.
Experimental evidence of the existence of the five stages of grief is not enough. The longest and most extensive bereavement interview was conducted in 2007.
According to him, the most common state at any time is acceptance, only a few go through the stage of denial, and the second most common emotion is longing.
However, according to David Kessler, while scientists debate the nuances and terms, people who experience grief continue to find meaning in the Kübler-Ross scheme. nine0011
"I meet people who tell me, 'I don't know what's wrong with me. Now I'm angry, and a minute later I'm sad. I must be crazy.” And I say, “It has names. These are called the stages of grief. ” The person says, “Oh, so there is a special stage called 'anger'? It's about me!" And feels more normal."
” The person says, “Oh, so there is a special stage called 'anger'? It's about me!" And feels more normal."
Image copyright, Getty Images
"People need catchy statements. If Kübler-Ross hadn't called it stages and stated that there are exactly five of them, then she probably would have been closer to the truth. But then she would not have attracted to attention," says Charles Corr. nine0011
He believes that talking about the five stages distracts from the main scientific legacy of Elisabeth Kübler-Ross.
"She wanted to take on the topic of death and dying in the broadest sense: how to help terminally ill people come to terms with their diagnosis, how to help those who care for them, support these patients and cope with their own emotions, how to help everyone live a full life, realizing that we are not eternal,” says Charles Corr.
"The terminally ill can teach us everything: not only how to die, but also how to live," said Elisabeth Kübler-Ross at 1983 year.
During the 1970s and 1980s, she traveled the world, giving lectures and giving workshops to thousands of people. She was a passionate supporter of the hospice idea pioneered by British nurse Cecily Saunders.
Kübler-Ross has established hospices in many countries, the first in the Netherlands in 1999. Time magazine named her one of the 100 most important thinkers of the 20th century.
Professor Kübler-Ross' scientific reputation was shaken after she became fascinated with theories about the afterlife and began to experiment with mediums. nine0011
One of them, a certain Jay Barham, practiced non-standard religious-erotic therapy, in particular, he persuaded women to have sex, assuring that he was possessed by a person close to them from the afterlife. In 1979, because of this, a loud scandal arose.
In the late 1980s, she tried to set up a hospice for children with AIDS in rural Virginia, but faced strong local opposition to the idea.
In 1995, her house caught fire under suspicious circumstances. The next day Kübler-Ross had her first stroke. nine0011
She spent the last nine years of her life with her son in Arizona, moving around in a wheelchair.
In her last interview with the famous TV presenter Oprah Winfrey, she said that at the thought of her own death she feels only anger.
"The public wanted the famed expert on death and dying to be some kind of angelic personality and quickly get to the stage of acceptance," says Ken Ross. "But we all deal with grief and loss as best we can."
The theory of the five stages of grief is not widely taught in medical schools these days. It is more popular at corporate trainings under the name "Curve of Change". nine0011
Since then, there have been many theories about how to deal with your grief.
David Kessler, with the consent of Kübler-Ross's family, added a sixth stage to the five: the understanding that everything that is done makes sense.
"Understanding can come in a million different ways. Let's say I've become a better person after losing a loved one. Maybe my loved one passed away in a different way than it should have happened, and I can try to make the world a better place to this has not happened to others," says David Kessler. nine0011
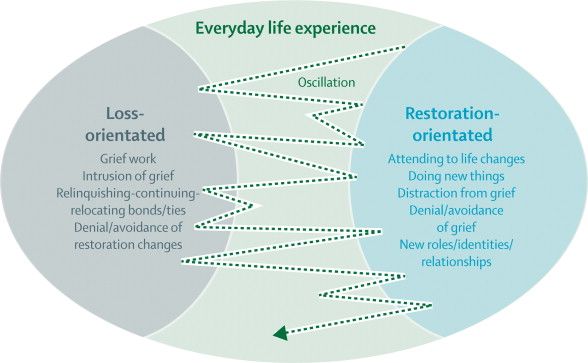
Charles Corr recommends the "double process model". It was developed by Dutch researchers Margaret Stroebe and Nenk Schut and suggests that a person in grief is simultaneously experiencing a loss and preparing himself for new things and life challenges.
George Bonanno talks about four trajectories of grief. Some people have great stamina and do not fall into depression, or it is weakly expressed in them, others remain morally broken for many years, others recover relatively close, but then a second wave of grief rolls over them, and finally, the fourth becomes stronger from the loss. nine0011
Over time, one way or another, the vast majority of people get better.
But Professor Bonanno admits that his approach is less clear-cut than the five-stage theory.
"I can say to a person: 'Time heals.' But that doesn't sound so convincing," he says.
Grief is difficult to control and hard to endure. The thought that there is some kind of road map that suggests a way out is comforting, even if it is an illusion.
Elisabeth Kübler-Ross, in her latest book, Grief and How We Grieve, wrote that she did not expect to sort out the tangled human emotions. nine0011
Everyone experiences grief in their own way, even if some patterns can sometimes be deduced. Everyone goes their own way.
Work of grief — About Palliative
Psychologist Larisa Pyzhyanova herself experienced the loss of loved ones and, working in the Ministry of Emergency Situations, hundreds of times helped people whose relatives died tragically and suddenly. We publish an excerpt from her book “Sharing the pain. The experience of a psychologist from the Ministry of Emergency Situations, which is useful to everyone, ”which tells about what the work of grief is, what processes and why a person experiences after the death of a loved one, how long it can last, what is considered the norm, and what should alert. nine0178
The experience of a psychologist from the Ministry of Emergency Situations, which is useful to everyone, ”which tells about what the work of grief is, what processes and why a person experiences after the death of a loved one, how long it can last, what is considered the norm, and what should alert. nine0178
The book can be bought on the site of the publishing house "Nikeya".
Crisis of grief
It is impossible to draw a clear framework and determine exactly whether the experience of loss is complicated or not complicated in a person. But still, it is possible to indicate when the process of natural grief goes through certain stages, each of which is characterized by its own set of physical and psychological symptoms.
The symptoms of "normal" grief in the middle of the last century were identified by the German-American psychiatrist, a specialist in social psychiatry, Erich Lindemann. The mourning process is divided into two main stages: the grief crisis and the work of grief. nine0011
nine0011
A crisis of grief begins with the death of a loved one or the discovery of an imminent loss, for example, when a loved one is diagnosed with a fatal illness and his days are numbered. Human consciousness rejects the fact of loss, rushes between denial, splitting, persuasion, anxiety and guilt.
According to Lindemann, the first hours after a loss are usually characterized by the presence of periodic bouts of physical suffering, spasms in the throat, fits of suffocation with rapid breathing, a constant need to breathe - this breathing disorder is especially noticeable when a person talks about his grief. At the spiritual level, grief manifests itself as tension or acute suffering. Usually the grieving person feels the unreality of what is happening, deafness, the feeling that everything is happening as if not with him. He has the so-called "tunnel vision", a veil is growing before his eyes. Time speeds up or, conversely, stops. The perception of the surrounding reality is dulled, sometimes in the future there will be gaps in the memories of this period. nine0011
nine0011
Lindemann noted that with a deep emotional experience, changes and disorders of consciousness can be observed. He describes a typical case in which it seemed to the patient that he saw his dead daughter, who was calling him from a telephone booth. He was so captured by this scene that he stopped noticing his surroundings.
It happens that a grieving person has no manifestations of strong feelings at all. Despite the deceptive external well-being, in reality the person is in a serious condition, and one of the dangers is that at any moment this imaginary calmness can be replaced by an acute reactive state. nine0011
It is possible to identify the mechanisms that are necessary for living through a crisis of grief: denial, splitting, persuasion, anxiety and guilt. When the first shock passes and the person begins to realize the reality of what is happening, the physical reactions weaken, and often there is an acute desire to return everything as it was before the loss. At this time, it seems to people that this is just a bad dream, you just need to wake up, and the nightmare will pass.
At this time, it seems to people that this is just a bad dream, you just need to wake up, and the nightmare will pass.
The well-known Russian psychotherapist, doctor of psychological sciences, professor Fedor Efimovich Vasilyuk, in his work “Surviving grief” says that denial at this stage of mourning is not a denial of the fact that the deceased is no more, but a denial of the fact that I, “grieving”, here. But loss denial allows a person to maintain the illusion that the world remains unchanged. This softens the shock and helps to gradually accept reality, which is facilitated by the rituals of farewell to the deceased adopted in different religions. Such important actions as a funeral service in the church, a memorial meal, help to accept the death of a loved one as a fait accompli. nine0011
Farewell to the deceased Farewell in the mortuary, funeral service, funeral service - what you need to know about them
Without such contact with reality, a person can get stuck in denial of the loss.
This is well illustrated by cases of missing people. Their death is very difficult to accept for loved ones. Splitting allows one part of the mind to know about the loss when the other denies it - this is when a person understands with the mind that a loved one has died, but feels his invisible presence. This is such a common phenomenon that many experts perceive it as part of the normal process of grief - people find comfort in this, the last chance to say goodbye to a loved one. nine0011
Vasilyuk writes: “There is… ‘a sort of double being’ (“I live as if on two planes,” says the mourner), where behind the fabric of reality one constantly senses another existence implicitly going through, breaking through islands of ‘meetings’ with the dead. Hope, which constantly gives rise to faith in a miracle, coexists in a strange way with a realistic attitude that guides all the external behavior of the mourner.
Persuasion manifests itself in the resistance of consciousness to what happened in such a way that, trying to deceive fate, as it were, a person concludes an internal deal, again and again remembering the last days, hours before parting, as if wishing to change the course of events: “Oh, if only. .. I would give everything so that ... "Grieving people constantly scroll through the events associated with the loss in their heads: they remember what they did not have time to do for the departed; they regret that they paid little attention to him, did not fulfill some requests, were not affectionate enough, did not have time to say “I love”, unfairly offended and did not have time to ask for forgiveness. nine0011
.. I would give everything so that ... "Grieving people constantly scroll through the events associated with the loss in their heads: they remember what they did not have time to do for the departed; they regret that they paid little attention to him, did not fulfill some requests, were not affectionate enough, did not have time to say “I love”, unfairly offended and did not have time to ask for forgiveness. nine0011
When people experience the reality of loss, they experience anxiety and helplessness. For a person who feels very insecure without his loved one, life is full of fears. Sometimes it is, for example, the fear of sleeping in the same bed or room, living in the same house.
The heaviest feeling when experiencing grief is guilt. Sometimes it can be real, more often far-fetched, but it must always be taken with great seriousness. Death exacerbates the problems that have ever taken place in a relationship, and the “stumbling blocks” that were hardly noticeable before turn into an insurmountable obstacle after the death of a loved one.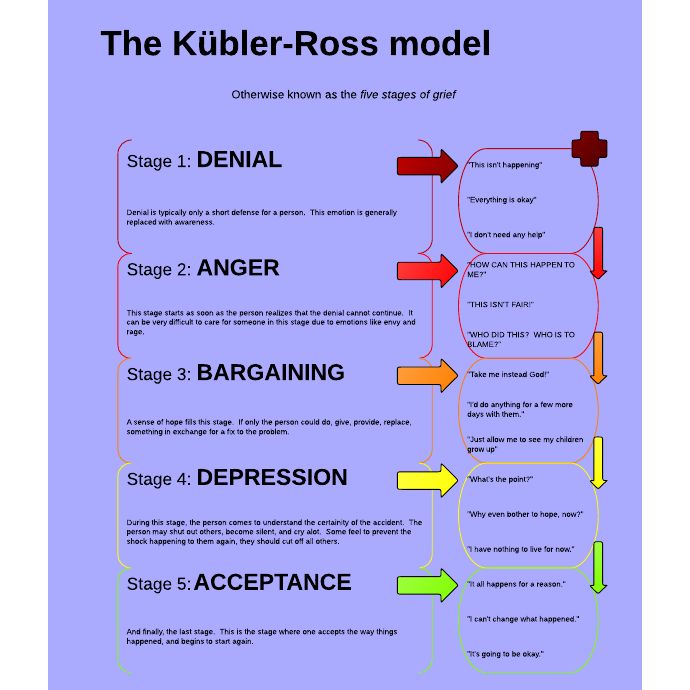 Lindemann describes it this way: “A person who has suffered a loss tries to find in the events that preceded death evidence that he did not do what he could for the deceased. He accuses himself of inattention and exaggerates the significance of his slightest missteps. The person repeats the word "should" like a spell: "I should have done this" or "I should not have done this." There are many heavy thoughts, a feeling of emptiness and meaninglessness. Over time, a rational explanation of what happened will soften the feeling of guilt, but usually it returns until there is full acceptance of the loss. nine0011
Lindemann describes it this way: “A person who has suffered a loss tries to find in the events that preceded death evidence that he did not do what he could for the deceased. He accuses himself of inattention and exaggerates the significance of his slightest missteps. The person repeats the word "should" like a spell: "I should have done this" or "I should not have done this." There are many heavy thoughts, a feeling of emptiness and meaninglessness. Over time, a rational explanation of what happened will soften the feeling of guilt, but usually it returns until there is full acceptance of the loss. nine0011
Feelings of guilt before a deceased loved one: how to deal with it? When a loved one dies, a feeling of guilt often arises: you didn’t give enough, you didn’t say it, you didn’t do it, and now you can’t fix anything. Is this guilt always just, or is there something else behind it?
Israeli director Shmuel Maoz told an episode from his life. It was about his teenage daughter, who constantly woke up late, missed her school bus, and had to call her a taxi, which cost the family dearly. Once he told his daughter to take the bus, like all children, and if she oversleeps and is late, let this be a lesson for her. The next morning, the girl got up on time, left the house, and half an hour later, her father heard a message that there had been an explosion in this bus - a terrorist attack, dozens of people had died. He rushed to call his daughter, but could not get through. In the next hour, he experienced more than he had experienced in his entire life. And then the daughter returned home alive and unharmed - she still missed that bus. Shmuel Maoz said that later he tormented himself for a long time with the thought that he seemed to have done the right thing, logically, but how would he live if his daughter died? nine0011
It was about his teenage daughter, who constantly woke up late, missed her school bus, and had to call her a taxi, which cost the family dearly. Once he told his daughter to take the bus, like all children, and if she oversleeps and is late, let this be a lesson for her. The next morning, the girl got up on time, left the house, and half an hour later, her father heard a message that there had been an explosion in this bus - a terrorist attack, dozens of people had died. He rushed to call his daughter, but could not get through. In the next hour, he experienced more than he had experienced in his entire life. And then the daughter returned home alive and unharmed - she still missed that bus. Shmuel Maoz said that later he tormented himself for a long time with the thought that he seemed to have done the right thing, logically, but how would he live if his daughter died? nine0011
Probably, this “but” always arises in front of a person when trouble happens to his loved ones. It seems that he did everything, but . .. But he could have done more, better, could have foreseen everything, warned, averted trouble.
.. But he could have done more, better, could have foreseen everything, warned, averted trouble.
The stages of grief come in waves, one wave of denial, splitting, persuasion, anxiety, guilt is rarely enough to accept the loss.
Over time, they qualitatively change and the impulse "I need to call my mother" is gradually replaced by a more urgent need - "I need to be able to call my mother." The weight of the loss begins to be felt. During a crisis of grief, many processes occur at the level of the unconscious; dreams indicate that serious internal work is underway to overcome the feeling of loss. They solve the main task of the crisis of grief - the recognition of the need to accept the death of a loved one. nine0011
Work of grief
The process of mourning is called the work of grief. This is a huge mental work to process tragic events, the main task of which is not to forget, to preserve the memory of a dear person, while building new relationships with a world in which this person no longer exists.
The work of grief begins when a person accepts the fact of death. Then complex processes of overcoming take place, as a result of which the lost relationships gradually become memories, which, ideally, do not completely absorb a person, but transfer grief into a state of light sadness. nine0011
It should be noted that with all the variety of Western studies, the experience of grief and loss comes down to one scheme of Sigmund Freud, given by him in Sorrow and Melancholy: "Out of sight, out of mind." “Freud's theory explains how people forget the departed, but it does not even raise the question of how they remember them. We can say that this is the theory of oblivion,” writes psychotherapist Fyodor Vasilyuk.
In the book of Metropolitan Anthony of Surozh “Life and eternity. 15 Conversations on Death and Suffering” is an important evidence of the attitude towards death of the British: “Here, in England, the attitude towards death is very surprising for a Russian person like me. It has improved somewhat, I dare say, not much, but it has become, let's say, less terrible. And when I first met him, I was amazed. I was under the impression that it was something completely obscene for a good Briton to die, that people should not do this to their friends and relatives, and if they fell so low as to leave this world, they would be hidden in their room until the funeral home will not take them to their place of rest and will not release the family from their presence, because in relation to their relatives a person should not do such an obscene thing as dying. nine0011
It has improved somewhat, I dare say, not much, but it has become, let's say, less terrible. And when I first met him, I was amazed. I was under the impression that it was something completely obscene for a good Briton to die, that people should not do this to their friends and relatives, and if they fell so low as to leave this world, they would be hidden in their room until the funeral home will not take them to their place of rest and will not release the family from their presence, because in relation to their relatives a person should not do such an obscene thing as dying. nine0011
“Grief is not just one of the feelings, it is a constitutive anthropological phenomenon: not a single most intelligent animal buries its fellows. To bury is to be human. But to bury is not to discard, but to hide and preserve. And on the psychological level, the main acts of the mystery of grief are not the separation of energy from the lost object, but the arrangement of the image of this object for storage in memory. Human grief is not destructive (to forget, tear off, separate), but constructive, it is designed not to scatter, but to collect, not to destroy, but to create - to create memory, ”says Vasilyuk’s work“ Survive Grief. nine0011
Human grief is not destructive (to forget, tear off, separate), but constructive, it is designed not to scatter, but to collect, not to destroy, but to create - to create memory, ”says Vasilyuk’s work“ Survive Grief. nine0011
There are two main components of successful grief work: re-understanding the relationship with the deceased in order to appreciate what they mean to us, and then "translate" them into the category of "memories without a future."
Surviving means realizing what happened, accepting changes in life, adapting to the changed situation and gradually replacing the feeling of suffering and pain with a calm memory.
Freud, in his work "Sadness and Melancholy", emphasized that we never voluntarily give up our emotional attachments, and that we have been abandoned, rejected or left does not mean that we end relationships with those who did this . After the death of a loved one, we, one way or another, continue to respond to his emotional presence, while realizing that the person is not with us. In order to understand what we lost with the departed and what these relationships were for us, we return to them, look through them over and over again and play them again in memory, dreams, daydreams. Warm memories cause feelings of happiness, unfinished disputes and conflicts make us experience disappointment, anger, sadness again and again. The task of the work of grief is to bring us back again and again to these situations and states until we calmly look at them and accept them as they were. nine0011
In order to understand what we lost with the departed and what these relationships were for us, we return to them, look through them over and over again and play them again in memory, dreams, daydreams. Warm memories cause feelings of happiness, unfinished disputes and conflicts make us experience disappointment, anger, sadness again and again. The task of the work of grief is to bring us back again and again to these situations and states until we calmly look at them and accept them as they were. nine0011
One of the biggest obstacles to adjusting to a new life, according to Lindemann, is that many people try to avoid the intense suffering associated with grief and avoid expressing the emotions necessary for this experience.
That is why painful manifestations are observed in the form of a delay in the reaction or in its various distortions. The ability to perform the work of grief depends on many things, including age, the degree of personal maturity. In the absence of healthy breakups in the past, the work of grief is much slower. Before coming to terms with a new loss, a person is forced to experience the previous unfinished losses. nine0011
In the absence of healthy breakups in the past, the work of grief is much slower. Before coming to terms with a new loss, a person is forced to experience the previous unfinished losses. nine0011
The work of grief is exhausting. Unconsciously, a person again and again returns to the past and is under its weight. He is constantly faced with loneliness and acute longing. It takes a lot of strength. Time passes, and little by little the demands of the present begin to assert themselves. The person begins to feel the desire to move on. However, a part of him is still gripped by grief. The desire to end the mourning and only from time to time remember the deceased can be unconsciously perceived as a betrayal, cause a feeling of guilt and slow down the processes of grief. nine0011
When does grief end?
When it seems that grief is over and everything is over, it can sometimes return in the form of acute experiences. In memorable places or on memorable dates. And that's okay.
And that's okay.
Let me give you an example from my own life. Two and a half years have passed since my mother's death, and I finally decided to come to her empty apartment to sort things out and prepare the apartment for sale. It seemed to me that I had already experienced everything and accepted everything. My son and I sorted things out, sometimes hovering over something for a long time, sometimes very quickly deciding who to give what to, where to give what. Behind every item were many of my memories. I talked about something, we laughed, joked, sometimes sad, but in general I had the feeling that everything was going well and I was so afraid in vain. And I also thought: “It’s good that my son went with me.” And on the third day, I suddenly had a very familiar and very severe headache, and I said: “How strange, such a state, as if I have been working for an emergency for the third day.” My son answered me: “And you work for emergency situations.” nine0011
Loss Oncopsychologist - about personal experience of loss, feelings of guilt and warm memories that illuminate the darkness
Loss can always "come to life" and cause acute pain again, it can return on anniversaries or at moments of important life milestones. But gradually more and more memories appear, freed from pain, guilt, resentment. A person gets the opportunity to escape from the past and turns to the future - he begins to plan his life without the deceased. At this stage, life enters its own track, sleep, appetite, daily activities are restored, the deceased ceases to occupy all thoughts. nine0011
But gradually more and more memories appear, freed from pain, guilt, resentment. A person gets the opportunity to escape from the past and turns to the future - he begins to plan his life without the deceased. At this stage, life enters its own track, sleep, appetite, daily activities are restored, the deceased ceases to occupy all thoughts. nine0011
The meaning and task of the work of grief is to make a person forgive himself, let go of resentment, take responsibility for his life. The image of the deceased must take its permanent worthy place in his life, then the person himself will return.
Remembering the deceased, he will no longer experience grief, but sadness - a completely different feeling. And this sadness will forever remain in the heart. If there are tears, they must be wept. But then there comes a time when you can say to yourself: if right now you can restrain yourself and not cry, don’t cry. We must get off the path of tears. If you continue to walk along it, the path can turn into a groove, and then into a trench so deep that it will be impossible to get out of it unless a hand is extended from above. And if you don’t want to reach out in response, then after a while not a single hand will simply be able to reach you - you will be so deep. nine0011
And if you don’t want to reach out in response, then after a while not a single hand will simply be able to reach you - you will be so deep. nine0011
Heavy mourning is not synonymous with love, and to stop mourning does not mean to betray the departed. Because it will not go anywhere from the heart, because Love does not go anywhere.
Stages of grief
- Shock and numbness (from a few seconds to several days). May result in an acute reactive state.
- Suffering and disorganization - acute grief (6-7 weeks). Grief work becomes the leading activity.
- Stage of residual shocks and reorganization (up to a year). Loss gradually enters into life. nine0004
- Completion (1-1.5 years after loss). Grief is replaced by sadness.
The stage of acute grief may include:
- Denial as a natural defense mechanism to maintain the illusion that the world remains unchanged. It is not the fact of loss that is denied, but its irreversibility.