Cyclic vomiting syndrome forum
Cyclic Vomiting Syndrome Message Board
Cyclic Vomiting Syndrome Message Board
Note: Your browser does not have JavaScript enabled. Many features may not work properly without it. Please enable JavaScript in your browser settings.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| There are currently 2 users online: 0 members, 2 guests Most users ever online was 1419 on . | ||
| Topics: 5,685, Posts: 43,787 , Members: 2,046 - Members List Please welcome our newest member, Hermione | ||
Easily create a Forum Website with Website Toolbox.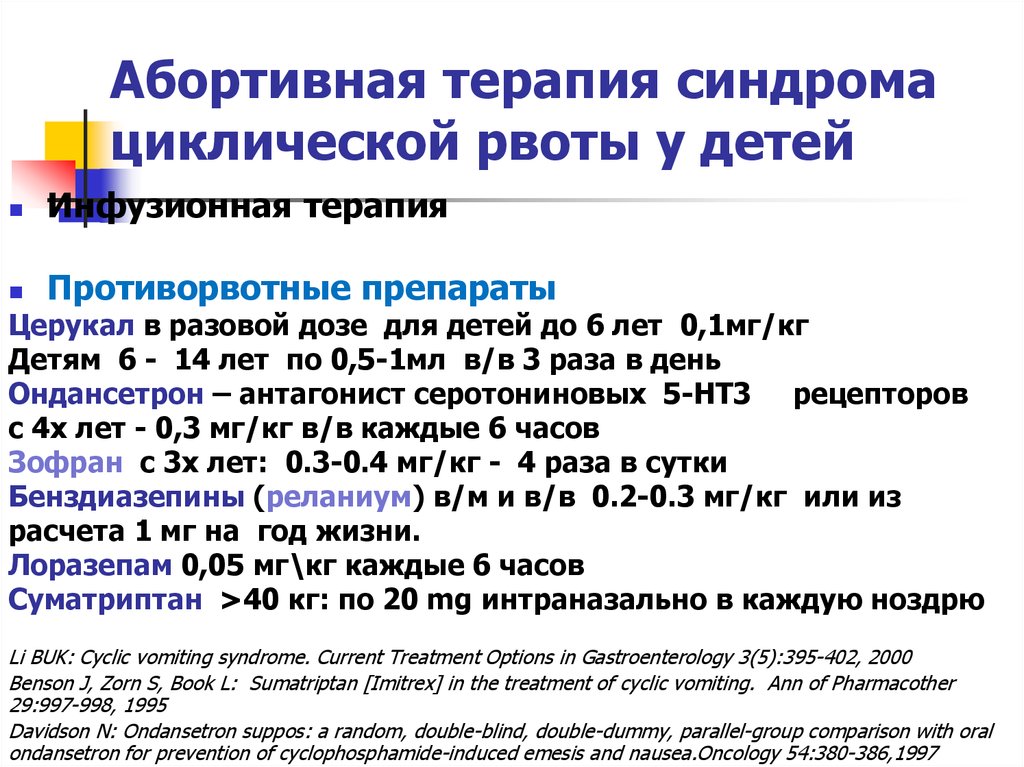
Cyclic Vomiting Syndrome - Gastrointestinal Society
Skip to contentCyclic Vomiting SyndromeGIS2021-07-07T13:22:50-07:00
An Under-Recognized Gastrointestinal Condition
Cyclic vomiting syndrome (CVS) is a functional gastrointestinal (GI) condition, which causes recurring episodes of severe nausea and vomiting. Episodes, or attacks, occur suddenly and can last from hours to days. Individuals with CVS typically do not experience any symptoms (asymptomatic) during the weeks to months between episodes. In most cases, CVS develops during early childhood (often between 3-7 years-of-age) and continues until adolescence. Typically, digestive symptoms cease during adolescence and, although the link is not fully clear, many individuals who have this disorder in childhood begin to experience migraines as adults. However, CVS can also persist until adulthood or, in some cases, develop after childhood.
Causes
As is the case for many functional GI conditions, we do not know exactly what causes CVS, but there are certain factors that might contribute to its development.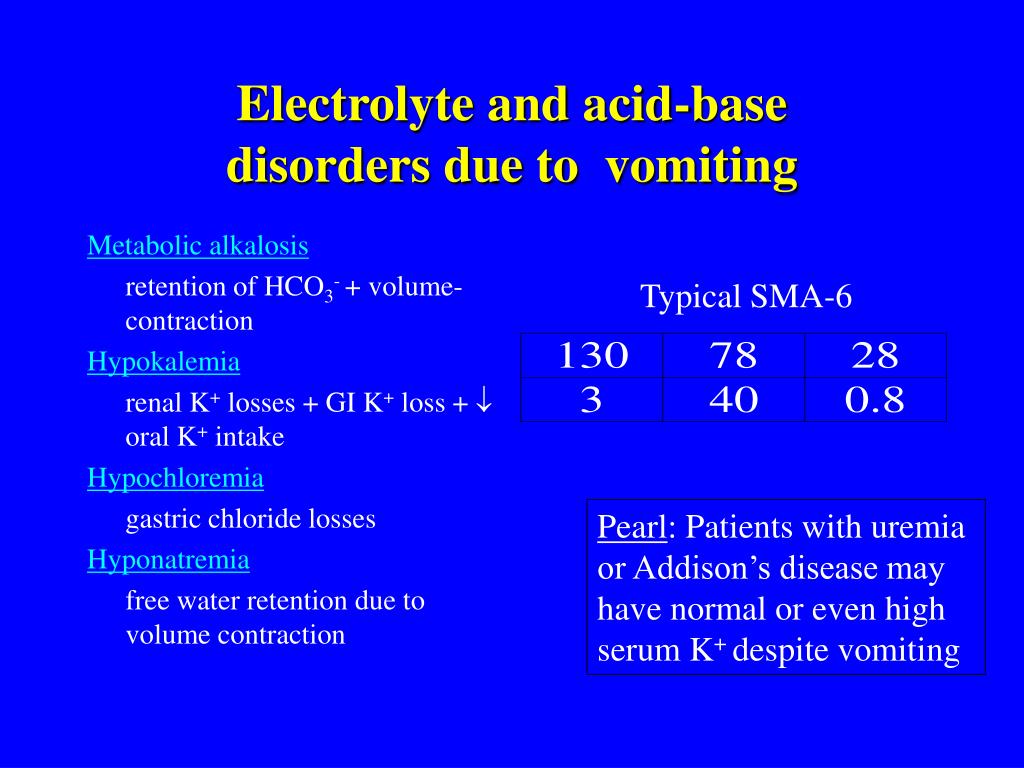
Researchers speculate at the possibility of some degree of mitochondrial inheritance, because a maternal family history of either CVS or migraines can make an individual more likely to develop this condition.1,2
The episodes in CVS can occur without warning, but most affected individuals have triggers that can make attacks more likely. These can include other illnesses or infections, physical exhaustion, lack of sleep, hormonal changes (such as during menstruation), certain foods, overeating or eating before bed, and emotional stress or excitement, including happy occasions such as birthdays and holidays.
While the symptoms of CVS occur in the digestive tract, the true cause might be a brain-gut disorder. This theory is supported by the fact that emotional events are one of the most frequent symptom triggers. The high correlation between CVS and migraines, and the lack of symptoms between episodes, points to the possibility that CVS could be a ‘migraine of the stomach’.
Symptoms
During an episode of CVS, the primary symptoms are severe nausea and vomiting. This typically includes retching for several hours, with no abating of nausea after vomiting. Other symptoms include headaches, fever, pallor, dizziness, and lethargy. Some individuals will also experience increased sensitivity to sensory input such as light, sounds, and smells.
Repeated vomiting can cause dehydration, which might require a hospital visit, particularly if the affected individual is a young child. In severe cases, with very frequent vomiting, symptoms from exposure to harsh stomach acid can occur. These symptoms include inflammation of the esophagus (esophagitis) and erosion of tooth enamel. It is important to minimize symptoms, where possible, to prevent complications.
Many individuals also experience nausea, sweating, and pallor before the vomiting begins (prodromal phase).
Prevalence
Past studies have found that CVS affects approximately 2% of school-aged children. 3 However, given the likeliness of misdiagnosis, the real number of children affected is likely higher. Statistics for CVS in adults are even more uncertain, especially because medical professionals have only acknowledged in the past few decades that this disorder can develop in adults.
3 However, given the likeliness of misdiagnosis, the real number of children affected is likely higher. Statistics for CVS in adults are even more uncertain, especially because medical professionals have only acknowledged in the past few decades that this disorder can develop in adults.
Diagnosis
Since this is a functional condition, there is no diagnostic test to confirm cyclic vomiting syndrome. Therefore, diagnosis relies primarily on patient history. During an exam, physicians may ask questions about symptoms, such as how often they occur, when they occur, and how severe they are, and then use this information to decide if CVS is likely. They might also perform a variety of diagnostic tests to rule out other diseases and disorders.
The Rome IV Criteria (an international set of standards) for CVS helps physicians make a diagnosis. These criteria are:
- at least three episodes of acute vomiting in the past twelve months, with each episode lasting less than one week,
- with two episodes in the last six months, and at least one week between each episode, and
- with no vomiting between episodes (although sometimes there might be nausea)
Physicians might misdiagnose CVS because its symptoms closely mirror those of other illnesses, such as gastroenteritis, and occur periodically rather than continuously.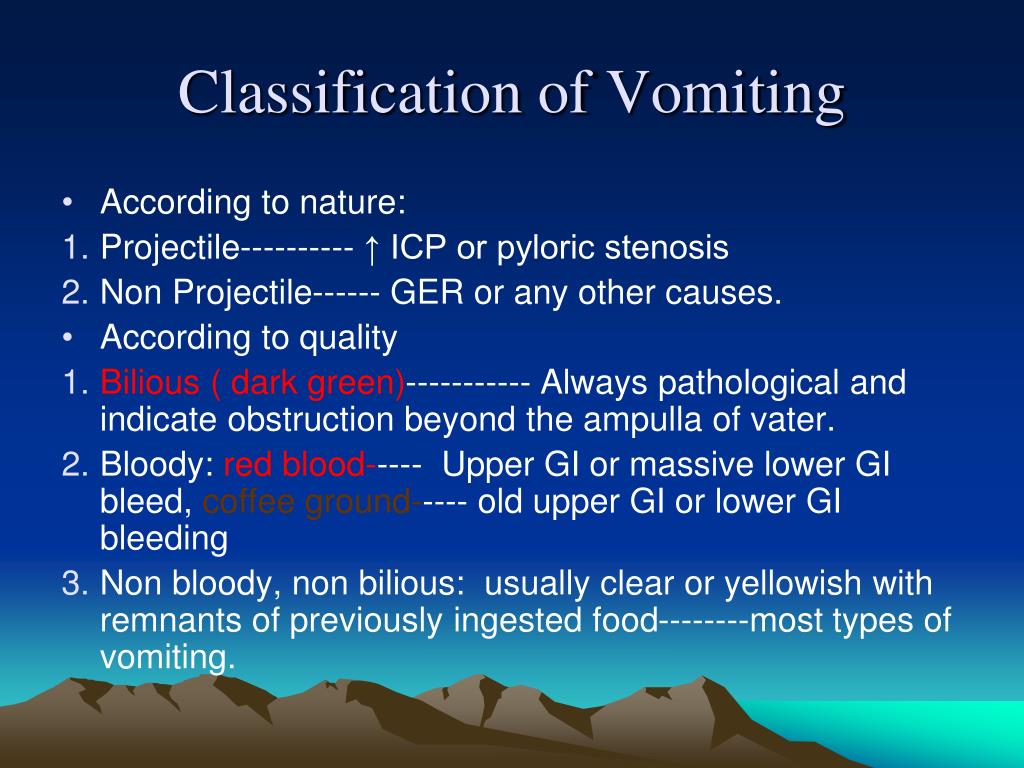
Cannabinoid Hyperemesis Syndrome
Recently, physicians have been increasingly diagnosing a condition called cannabinoid hyperemesis syndrome (CHS) in teenagers and adults who use cannabis. CHS has similar symptoms to CVS: both include periods of nausea and vomiting spaced out between asymptomatic periods. However, these two conditions are not the same, and some physicians might assume an individual has CHS, even if the patient claims not to use cannabis. The distinction becomes even more complex in adults who do use cannabis. Some adults might have started to use cannabis after symptom onset to help ease nausea, or for other reasons unrelated to symptoms, but could still have CVS. One unique feature in cannabinoid hyperemesis syndrome is a strong desire to take hot showers to relieve symptoms, a symptom that is absent in CVS. If a physician is still unsure which syndrome their patient has, it is best for the patient to abstain from cannabis use. If this causes symptoms to stop, then it is likely CHS. If symptoms continue, then it could be CVS.4 However, it is important to stop using cannabis for many weeks – not just a day or two – as it can take quite some time for symptoms to cease in cannabinoid hyperemesis syndrome.
If symptoms continue, then it could be CVS.4 However, it is important to stop using cannabis for many weeks – not just a day or two – as it can take quite some time for symptoms to cease in cannabinoid hyperemesis syndrome.
Management
Treating this condition is two-pronged, and involves preventing attacks whenever possible, and easing symptoms during attacks.
Preventing Episodes
Avoiding known triggers is the best way to prevent attacks from occurring. If you or your child experiences CVS attacks after eating certain foods, or during certain events, try to avoid these whenever practical. An elimination diet procedure could help determine a diet related trigger. Stress management techniques can prevent attacks from occurring during tense situations.
However, sometimes triggers are unavoidable, and there is still the chance of experiencing an episode without any warning. In these situations, it is important to have other treatments available. One medication, amitriptyline (Elavil®), is used to prevent migraines and might help prevent episodes of vomiting in CVS when taken daily. There is also some evidence that co-enzyme Q10, a widely available nutritional supplement, might work nearly as effectively as amitriptyline.5
There is also some evidence that co-enzyme Q10, a widely available nutritional supplement, might work nearly as effectively as amitriptyline.5
Treating Episodes
During an episode of vomiting, it is important to remain comfortable. Bed rest is ideal, and this should be in a quiet environment with minimal lighting, similar to how you would set the room for an individual with a severe migraine.
Prolonged vomiting can cause dehydration, so be sure to drink fluids whenever possible. Electrolyte preparations, such as Pedialyte® or Hydralyte™ might also be necessary. If someone with cyclic vomiting syndrome shows signs of severe dehydration, such as excessive thirst, urine that is dark or very infrequent urination, dry skin or sunken eyes, and faintness or lethargy, then go to the emergency room, where they can provide intravenous hydration and any other necessary treatments.
During the prodromal phase or the vomiting phase, some medications can help control symptoms, such as those that reduce nausea and vomiting. Over-the-counter pain relief medicines, such as acetaminophen (Tylenol®) or ibuprofen (Advil®) can help reduce abdominal pain. Medications that suppress acid secretion, including histamine-2 receptor antagonists (H2RAs) and proton pump inhibitors (PPIs), can be useful for those with CVS by making stomach contents less acidic, thereby decreasing acid damage to the esophagus and teeth.6 Make sure to check with your physician before taking over-the-counter medications to treat CVS episodes.
Over-the-counter pain relief medicines, such as acetaminophen (Tylenol®) or ibuprofen (Advil®) can help reduce abdominal pain. Medications that suppress acid secretion, including histamine-2 receptor antagonists (H2RAs) and proton pump inhibitors (PPIs), can be useful for those with CVS by making stomach contents less acidic, thereby decreasing acid damage to the esophagus and teeth.6 Make sure to check with your physician before taking over-the-counter medications to treat CVS episodes.
Outlook
While symptoms tend to be severe during attacks, most individuals with this condition live relatively normal lives in between episodes. In addition, many children outgrow cyclic vomiting syndrome over time, but they might develop migraines instead.
First published in the
Inside Tract® newsletter issue 205 – 2018Photo: © sumnersgraphicsinc | Bigstockphoto.com
1. Venkatesan T
et al. Quantitative pedigree analysis and mitochondrial DNA sequence variants in adults with cyclic vomiting syndrome. BMC Gastroenterology. 2014;14:181.
BMC Gastroenterology. 2014;14:181.2. Finsterer J et al. Cyclic vomiting syndrome in multisystem mitochondrial disorder. La Tunisie Medicale. 2015;93(7):424-6.
3. Abu-Arafeh I et al. Cyclical vomiting syndrome in children: a population-based study. Journal of Pediatric Gastroenterology and Nutrition. 1995;21(4):454-8.
4. Blumentrath CG et al. Cannabinoid hyperemesis and the cyclic vomiting syndrome in adults: recognition, diagnosis, acute and long-term treatment. German Medical Science. 2017;15:Doc06.
5. Boles RG et al. Treatment of cyclic vomiting syndrome with coenzyme Q10 and amitriptyline, a retrospective study. BMC Neurology. 2010, 10:10.
6. Yang HR. Recent Concepts on Cyclic Vomiting Syndrome in Children. Journal of Neurogastroenterology and Motility. 2010;16(2):139–147.
Email News Sign Up
Join the badgut.org email list and receive the latest news on digestive health, BadGut® Lectures, events, and more. Click here.
Click here.
Search
Search for:
Share This Page
Page load link Go to TopCyclic Vomiting Syndrome - Evidence Based Medicine for All
What is Cyclic Vomiting Syndrome
Cyclic Vomiting Syndrome is characterized by episodes of severe bouts of vomiting that have no apparent cause. These episodes can last for hours or even days, and are interspersed with relatively asymptomatic periods. Each episode is similar to the previous ones: it usually starts at the same time of day, lasts the same time, and is accompanied by the same symptoms and intensity level. nine0007
Until recently, doctors believed that cyclic vomiting syndrome (CRS) only affects children, but it has now been proven to occur in all age groups. Studies show that SCR occurs in almost 2% of school-age children, less often in adult patients, but this number is constantly growing.
Cyclic vomiting syndrome may be associated with migraine. His attacks can be quite severe and keep the patient out of bed for several days.
His attacks can be quite severe and keep the patient out of bed for several days.
Additional information:
- Infant colic equivalent to migraine
- Migraine. General information.
This syndrome is difficult to diagnose because vomiting is a symptom of many diseases. SCR is a diagnosis of exclusion, the clinician must be sure that there are no other causes of vomiting in this patient. Treatment for SCR usually includes symptomatic medication to ease the attacks and lifestyle changes to prevent recurrence. The most commonly used drugs are from the group of antiemetic and antimigraine drugs. nine0007
Symptoms
Symptoms of cyclic vomiting syndrome include:
- Bouts of severe vomiting: repeated vomiting several times an hour and lasting from several hours to 1 week
- Three or more such seizures occurring for no apparent reason in the past year
During an SCR attack, the patient may also experience:
- Abdominal pain
- Diarrhea nine0017 Fever
- Vertigo
- Photophobia
Additional information: Diarrhea in a child. Modern view of the problem.
Modern view of the problem.
In the interictal period, as a rule, patients do not have any symptoms of trouble. However, some patients experience mild to moderate nausea or pain in the extremities between episodes of SCR.
Repeated repeated vomiting can lead to severe dehydration, which can even threaten the patient's life. nine0007
Symptoms of dehydration include:
- Thirst
- Infrequent urination
- Paleness
- Severe weakness and weakness
- dryness of mucous membranes and skin
Causes
The causes of cyclic vomiting syndrome are unknown. In the studies, it was only possible to identify factors that can provoke a new exacerbation of the SCR. These include:
- Colds, allergies or sinus problems
- Emotional stress or great agitation (especially in children)
- Anxiety or panic attacks (especially in adults)
- Certain foodstuffs (most commonly chocolate and cheese)
- Eating too much or eating before bed
- Hot weather nine0017 Physical overwork
- Menstruation
- Motion sickness or motion sickness
Additional information:
- Hypothermia and colds (SARS).
 Is there a relationship
Is there a relationship - Colds (ARVI) in children. Symptoms, diagnosis, treatment.
Identification of the main triggers of SCR attacks in a particular patient is one of the main tasks of therapy, since reducing their exposure can dramatically reduce or even stop the recurrence of SCR. nine0007
Risk factors
The nature and extent of the association between migraine and cyclic vomiting syndrome is still unclear. However, many children with SCR have a family history of migraine or SCR. In many children with age, SCR attacks are replaced by migraine attacks. However, in adults, the relationship between cyclic vomiting syndrome and migraine is usually weak.
Chronic marijuana (cannabis) use is also an important factor in cyclic vomiting syndrome. nine0007
Complications
Cyclic vomiting syndrome can cause the following complications:
- Dehydration. Repeated vomiting leads to massive loss of water and salts from the body.
 In severe cases, dehydration may require hospitalization in an intensive care unit.
In severe cases, dehydration may require hospitalization in an intensive care unit. - Inflammation of the esophagus (esophagitis). Stomach acid found in vomit can damage the tube that connects the mouth and stomach (esophagus). Sometimes the damage to the esophagus is so severe that it begins to bleed. nine0018
- Caries. Acid in vomit can erode tooth enamel, leading to cavities and chronic halitosis.
How to prepare for a doctor's appointment?
Both an internist (pediatrician) and a gastroenterologist can treat this condition. If you or your child is currently having an SCR attack, it may require immediate hospitalization. In other cases, you will have time to prepare for a visit to the doctor in advance. nine0007
Here is some information to help you prepare for your appointment with your doctor and what to expect from him.
Things you can do to help your doctor:
- Write down your symptoms in a notepad, especially when and how often you vomit; typical causes of the onset of an attack of vomiting; frequency of vomiting and any signs that you consider characteristic of your illness.

- Record key medical information. Including those diagnoses that you were given earlier. nine0018
- Write down key personal information. Including, changing your dietary habits, dates of severe stress and unrest - both positive and negative (if we are talking about your child - his stress and unrest).
- Bring a complete list of all medications, vitamins, supplements, etc. that you or your child has taken in the past to the doctor.
- Write down in advance the questions you would like to ask your doctor. nine0018
Questions to ask your doctor
Here are some basic questions you might want to ask your doctor:
- What is the most likely cause of these symptoms?
- Are there any additional tests needed to rule out other causes of recurrent vomiting?
- Do you think this disease will soon pass, or will it bother me for a long time? nine0017 What treatments do you recommend?
- What drugs can help?
- What dietary restrictions and lifestyle changes might be helpful?
Feel free to ask your doctor questions.
What to expect from your doctor
Be prepared to answer your doctor's questions, for example:
- How long ago did you (your child) start having these symptoms? nine0018
- How often do episodes of severe vomiting occur, how many episodes of vomiting usually occur per attack?
- What was the duration of the last seizure?
- Do you (your child) experience abdominal pain during an attack?
- Are there any signs by which you can tell that a new attack will start very soon: loss of appetite, feeling unusually tired; Are there any triggers, such as strong emotions, other illnesses, or the onset of menstruation? nine0018
- Do you (your child) or in your family have a history of mental illness? Cases of severe somatic diseases?
- What treatments do you (or your child) take for other conditions, including over-the-counter drugs, dietary supplements, folk remedies, herbal medicine, and homeopathy?
- What remedies and methods do you usually use to relieve the symptoms of an SCR attack, and how effective are they? nine0018
- Did you or your child have episodes of severe headaches?
- Do you have a family history of SCR and/or migraine?
What you can do while waiting for the doctor
If you bring this problem to the doctor at the time of vomiting, the doctor will most likely make an appointment for you as soon as possible. If at the moment there is no exacerbation, then expectant tactics may be shown. nine0007
If at the moment there is no exacerbation, then expectant tactics may be shown. nine0007
During this time, you should get as much rest as possible, increase your fluid and high-calorie intake (after a multi-day episode of vomiting and lack of appetite), and avoid caffeinated drinks.
Additional examination methods
As mentioned above, MCR can be quite difficult to confirm. There are no reliable tests or diagnostic tests to confirm such a diagnosis, and the only way to verify SCR is to exclude all other causes of vomiting, and there are a lot of them. Accordingly, the amount of additional examination methods will depend very much on the characteristics of your symptoms and medical history. nine0007
The doctor will begin by asking detailed questions about your (or your child's) history, and conducting initial tests.
After that, based on the information received, the doctor can recommend:
Imaging examinations of the gastrointestinal tract: fibroendoscopy, computed tomography, magnetic resonance imaging, etc. With the help of these studies, the doctor will exclude the organic pathology of the digestive system and not only.
With the help of these studies, the doctor will exclude the organic pathology of the digestive system and not only.
Laboratory blood tests to check thyroid function and rule out other metabolic diseases
Additional information: Getting ready for laboratory tests or how to pass tests correctly.
MRI of the head to rule out a brain tumor and other disorders of the central nervous system
Other tests and tests - if there is a reasonable suspicion of a disease that may be causing your vomiting episodes.
Treatment of cyclic vomiting syndrome
There is no causal treatment for cyclic vomiting syndrome, so therapy focuses on suppressing the symptoms of exacerbations and preventing relapses. nine0007
Your doctor may prescribe you or your child:
- Antiemetics
- Sedatives
- Antacids
- Antidepressants and others
Sometimes a pronounced effect in an attack of SCR can be achieved by taking the same drugs that are commonly used to treat migraine.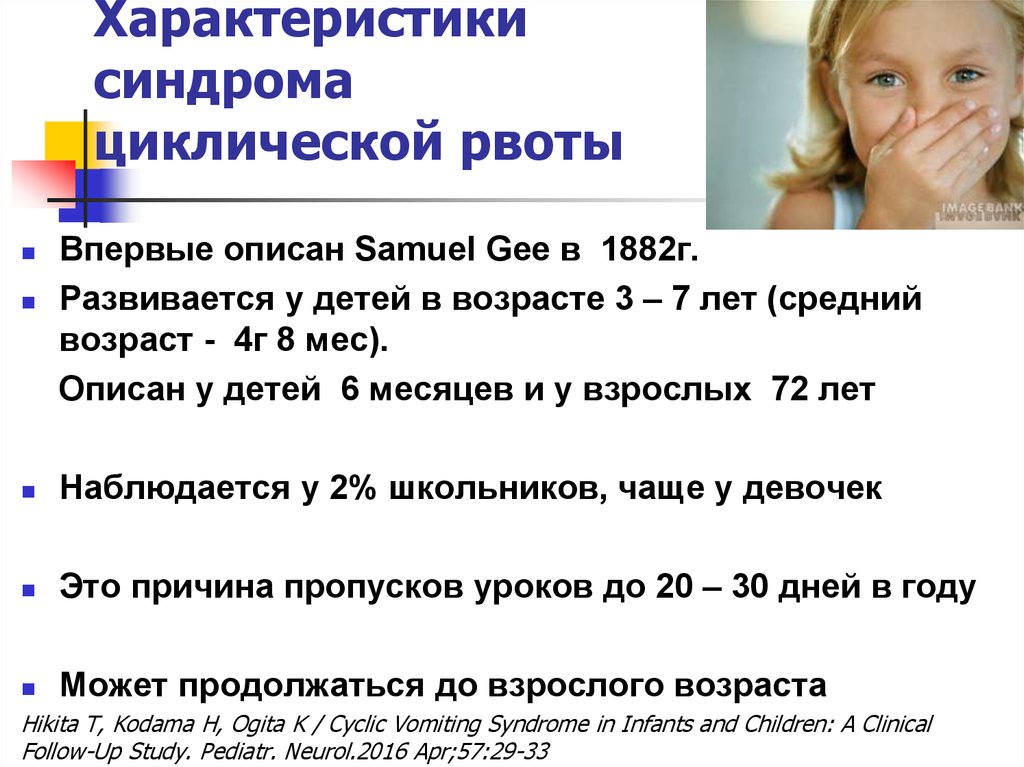 Anti-migraine drugs are especially indicated for people with frequent relapses of SCR.
Anti-migraine drugs are especially indicated for people with frequent relapses of SCR.
Behavior Therapy
Studies show that about half of people with CRS also have symptoms of depression or anxiety. However, the degree and nature of the relationship between SCR and depression remains unclear at the moment. Based on these symptoms, your doctor may prescribe behavioral therapy for you or your child.
Lifestyle changes and home remedies
A number of lifestyle changes can help relieve cyclic vomiting syndrome. First of all, people with SCR need to normalize sleep - it should be calm, comfortable and sufficient. This is useful not only as a preventive measure, but also during an attack that has begun - the patient should remain in a dark, quiet room and sleep as much as possible. nine0007
When the period of recurrent vomiting is over, it is very important to drink water and fluids that replace electrolytes (oral rehydration drugs). If the state of health is completely normal, and ordinary food does not cause nausea or vomiting, the diet is not required. Otherwise, you should follow a sparing diet in the early days, gradually and carefully expanding the diet.
Otherwise, you should follow a sparing diet in the early days, gradually and carefully expanding the diet.
If vomiting is triggered by stress or anxiety, try to avoid stress and remain calm during the asymptomatic interval. It can also be helpful to switch to six small meals a day instead of three large meals a day. nine0007
Alternative medicine
Alternative medicine and some paramedical techniques may be helpful in preventing vomiting, although none of these treatments have been studied in rigorous scientific studies. These methods include, for example:
Biofeedback training - this can help manage stress and, as a result, reduce the risk of an SCR attack.
- L-carnitine intake. nine0017 Taking Coenzyme Q10 (ubiquinone).
L-carnitine and coenzyme Q10 can help your body overcome difficulties in converting food into energy (mitochondrial dysfunction). Some researchers believe that mitochondrial dysfunction may be the main factor causing both cyclic vomiting syndrome and migraine.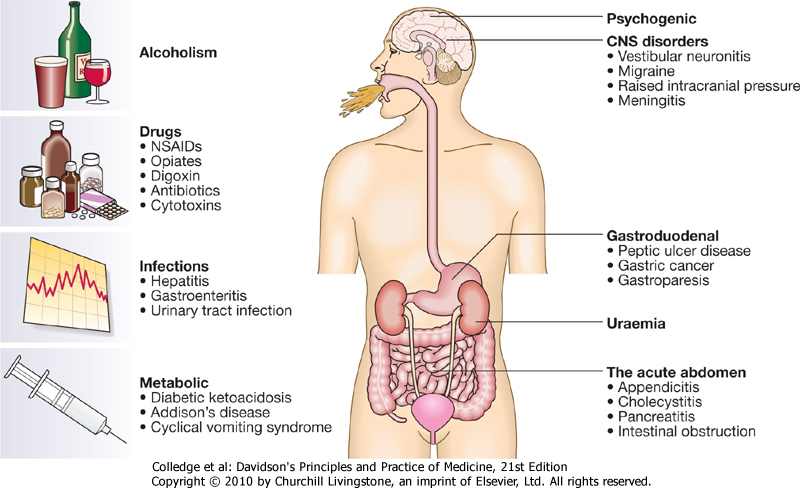
However, before taking any dietary supplements, you should make sure they are compatible with medications already prescribed by your doctor and, if possible, discuss with your doctor if they are appropriate and safe for you. You should also be aware that in some people, taking L-carnitine and Coenzyme Q10 can increase the severity of CCR. nine0007
General measures
Since CCR attacks happen suddenly, you can't know in advance when it will happen. This is especially worrisome for children, as having a seizure in front of other children can lead to stigmatization and ridicule.
Both the child and the adult can benefit from communicating with other patients with CRS, learn from their positive experiences and learn from their mistakes. Ask your doctor about the availability of psychological support groups for patients with CRS in your city. nine0007
Seizure Prevention
Many people with CRS know very well what triggers their seizures. Without any prompting from the doctor, they try to avoid these triggers.
Without any prompting from the doctor, they try to avoid these triggers.
If episodes occur more than once a month or require regular hospitalization, your doctor may recommend preventive medication. Lifestyle changes can also help you, in particular:
- Enough sleep nine0017 Avoidance of exciting and stressful events
- Avoidance of certain foods (e.g. cheese and chocolate)
- Reducing the amount of food at one meal by increasing the frequency of meals
Author: Sergey Aleksandrovich Butriy
COMPLEX DIAGNOSTICS OF REPEATED VOMITING
Research article
Karchin O.V.
Kokueva O.V.
Herts V.R. nine0007
DOI:
https://doi.org/10.23670/IRJ.2019.90.12.044
Issue: No. 12 (90), 2019
Published:
2019/12/18 9000 9000 Complex diagnosis
Scientific article
Novoselya N.V. 1, *, Kokueva O. V. 2 , Hertz W.R. 3 , Karchin O.V. 4
V. 2 , Hertz W.R. 3 , Karchin O.V. 4
1 ORCID: 0000-0003-1774-9125;
1, 2, 3, 4 Night of the Kuban Medical Institute, Krasnodar, Russia
* Corresponding author (ankvin[at]yandex.ru)
Annotation
Cyclic vomiting syndrome is a pathological condition in which the patient has experienced at least three separate episodes of vomiting, each of which was accompanied by more than four episodes of vomiting at the height of the disease . In typical cases, there are no more than two episodes per week. The average duration of an attack is 24-48 hours (minimum 2 hours), but can last for 10 days or more. The duration of the intervals when the patient is free from vomiting and practically healthy is different. Isovaleric acidemia has similar symptoms. nine0007
Key words: Cyclic vomiting syndrome, isovaleric acidemia, diet.
COMPLEX DIAGNOSTICS OF REPEATED VOMITING
Research article
1, *, Kokueva O.V. 2 Herts V.R. 3 Karchin O.V. 4
1 ORCID: 0000-0003-1774-9125;
1, 2, 3, 4 NSEPI of HE, Kuban Medical Institute, Krasnodar, Russian Federation
* Corresponding author (ankvin[at]yandex.ru)
Abstract
Cyclic vomiting syndrome is a pathological state in which a patient experiences at least three separate attacks of vomiting, each of which is accompanied by more than four vomiting episodes at the height of the disease. In typical cases, no more than two episodes per week are observed. The average duration of an attack is 24-48 hours (minimally 2 hours), but it can last for 10 days or more. The duration of the intervals when a patient is free from vomiting and is practically healthy is different. Isovaleric acidemia has similar symptoms. nine0007
Isovaleric acidemia has similar symptoms. nine0007
Keywords: Cyclic vomiting syndrome, isovaleric acidemia, diet.
Syndrome of cyclic vomiting (in the English literature Cyclic Vomiting Syndrome - CVS) is a disease predominantly of childhood, manifested by stereotypical repeated episodes of vomiting, with periods of complete well-being. This disease affects 2.3% of Australians and 1.9% of Scottish residents. CVS is responsible for 0.51% of all hospitalizations in pediatric wards in India. A prospective study showed that the prevalence of the disease is 3: 100,000. The syndrome most often develops in childhood, usually between the ages of 3 and 7 years (according to statistics, 2% of school-age children suffer from CVS), sometimes in adolescence, rarely in adults. nine0007
It is known that this syndrome occurs more often in girls (60:40), the onset is mainly at an early age. Sometimes this condition can stop or weaken after 12 years, or migraine or abdominal migraine develops later. The syndrome may be accompanied by the appearance of acetone in the urine during an episode of vomiting. Such periodic vomiting with acetonemia was first described in 1901 by Marfan. The critical age of its manifestation is 2–10 years, usually it disappears by the puberty period (Kvashnina L.V., 2016). Until now, the pathogenesis of these attacks has not been deciphered, there are several theories. It is believed that there is a genetic predisposition, predominantly maternal, it is believed that certain mutations in mitochondrial DNA may be a risk factor for the development of cyclic vomiting. An analysis of the pedigrees of children with cyclic vomiting showed a statistically significant prevalence in maternal relatives of such diseases as migraine, myopathies, convulsions and autonomic dysfunction. The pedigree for these diseases was burdened in 75% of mothers and only in 11% of fathers. nine0007
The syndrome may be accompanied by the appearance of acetone in the urine during an episode of vomiting. Such periodic vomiting with acetonemia was first described in 1901 by Marfan. The critical age of its manifestation is 2–10 years, usually it disappears by the puberty period (Kvashnina L.V., 2016). Until now, the pathogenesis of these attacks has not been deciphered, there are several theories. It is believed that there is a genetic predisposition, predominantly maternal, it is believed that certain mutations in mitochondrial DNA may be a risk factor for the development of cyclic vomiting. An analysis of the pedigrees of children with cyclic vomiting showed a statistically significant prevalence in maternal relatives of such diseases as migraine, myopathies, convulsions and autonomic dysfunction. The pedigree for these diseases was burdened in 75% of mothers and only in 11% of fathers. nine0007
Isovaleric acidemia (aciduria), a hereditary disease from the group of organic acidemias, caused by a deficiency of isovaleryl-CoA dehydrogenase, which is involved in the metabolism of leucine, has similar symptoms. Deficiency of this enzyme results in isovaleric acidosis, also sometimes referred to as "sweaty feet syndrome" because isovaleric acid smells similar to sweat. Manifested by vomiting, lethargy, hypotension, refusal to eat. Protein load, stress can provoke an attack. The highest content of leucine was noted in cheese - 3450 mg, egg powder - 3770 mg per 100 g of product, soy (tofu), chickpeas, lentils are also rich in this amino acid (https://veganworld.ru/health/amino_table/). These products should be reduced in the diet of patients. nine0007
Deficiency of this enzyme results in isovaleric acidosis, also sometimes referred to as "sweaty feet syndrome" because isovaleric acid smells similar to sweat. Manifested by vomiting, lethargy, hypotension, refusal to eat. Protein load, stress can provoke an attack. The highest content of leucine was noted in cheese - 3450 mg, egg powder - 3770 mg per 100 g of product, soy (tofu), chickpeas, lentils are also rich in this amino acid (https://veganworld.ru/health/amino_table/). These products should be reduced in the diet of patients. nine0007
For the diagnosis of isovaleric acidemia, the 2016 Federal Clinical Guidelines require the quantitative determination of isovaleric, 3-hydroxyisovaleric acids and isovalerylglycine in urine by tandem mass spectrometry or gas chromatography methods, determination of isovaleryl-CoA dehydrogenase enzyme activity in cultured fibroblasts, molecular (DNA) diagnostics to detect mutations in the IVD gene. Treatment of such children includes protein restriction, carnitine at a daily dose of up to 200 mg / kg / day, glycine. During the recovery period from the metabolic crisis, maltodextrin can be used to maintain the energy value of nutrition, as well as low-protein starch-based mixtures. nine0007
During the recovery period from the metabolic crisis, maltodextrin can be used to maintain the energy value of nutrition, as well as low-protein starch-based mixtures. nine0007
The aim of the work was to demonstrate a clinical case of cyclic vomiting syndrome.
Description of a clinical case. The parents of an 8-year-old girl came to the reception with complaints about the selective diet of the child, consisting almost exclusively of vegetable products, from animal food, she consumes only milk and eggs as part of various dishes. The child chose such a diet on his own, when trying to introduce meat dishes, attacks of vomiting and nausea intensify, the girl refuses to eat. The child's parents eat a normal diet. Also, the child is disturbed by episodes of headache and bouts of vomiting, which occur about 2 times a month. Vomiting may continue for 3 to 9 daysonce a day without bile and blood, during vomiting with the help of test strips, acetone is detected in the urine. Bouts of vomiting disturb from 3 years.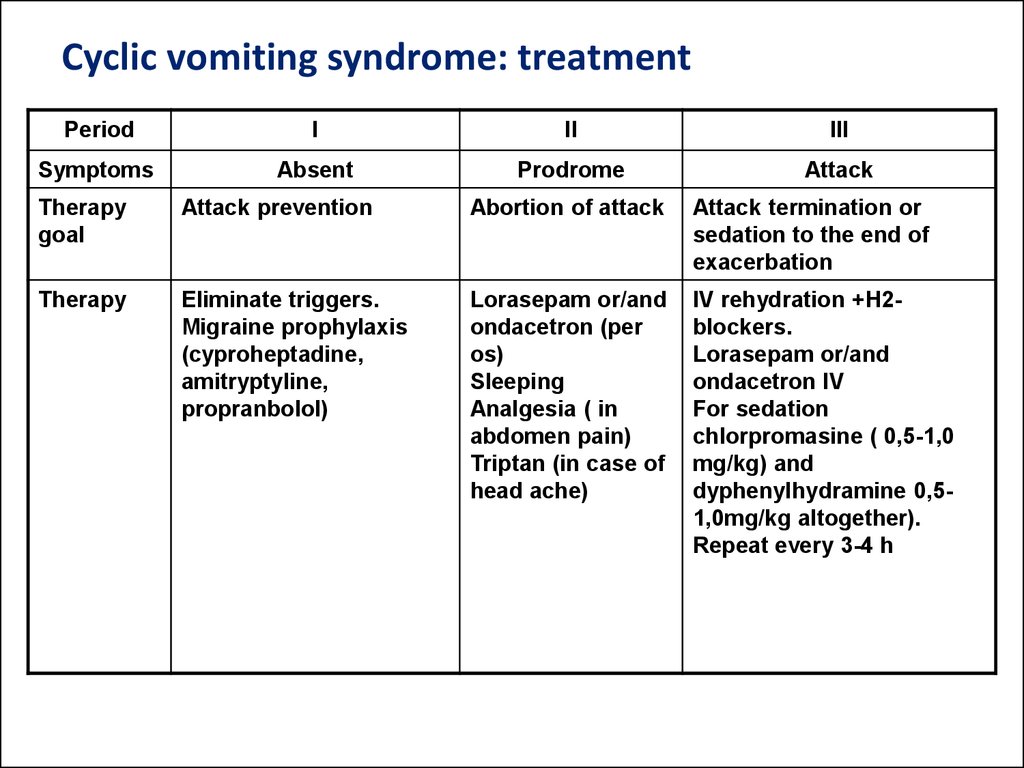
From the anamnesis revealed that at the age of 4 years with these complaints was examined in the gastroenterology department of the Children's Regional Clinical Hospital, diagnosed with Functional dyspepsia. Nervous-arthritic diathesis. Syndrome of cyclic vomiting. As a result of the ultrasound examination, echographic signs of a delimited cystic formation of a giant size of the left kidney without perifocal tissue changes were revealed, which can now be regarded as a fragment of a single-chamber solitary cyst of the kidney parenchyma. Computed tomography with contrast was recommended, consultation with a urologist. She was consulted by a gastroenterologist, with a diagnosis of functional dyspepsia, she received omeprazole, phosphalugel, domperidone, trimedat in courses without effect. Outside the attack, a general urinalysis without pathology. Examined by a neurologist, there is no lag in psychomotor development. Liver enzymes AST, ALT, total bilirubin, blood amylase, total protein within normal limits, alkaline phosphatase 83. 0 U/l, ferritin 120.8 ng/ml. Currently, he receives vitamin D3, omega 3, periodically takes citramon for headaches. On palpation of the abdomen, there is moderate pain in the epigastrium, also under the xiphoid process. nine0007
0 U/l, ferritin 120.8 ng/ml. Currently, he receives vitamin D3, omega 3, periodically takes citramon for headaches. On palpation of the abdomen, there is moderate pain in the epigastrium, also under the xiphoid process. nine0007
Taking into account the poor tolerance of protein foods, as well as the fact that the child independently adheres to a vegetarian diet, to clarify the diagnosis, it is recommended to quantify isovaleric, 3-hydroxyisovaleric acids and isovalerylglycine in the urine using tandem mass spectrometry or gas chromatography methods. Carry out molecular (DNA) diagnostics to identify mutations in the IVD gene. Conducted studies will help clarify the diagnosis.
The main task of diagnosing cyclic vomiting syndrome is to conduct a differential search with the exclusion of all possible diseases accompanied by vomiting. This syndrome should be differentiated from idiopathic occipital epilepsy with an early onset, Panagiotopoulos syndrome, as well as migraine and various gastrointestinal pathologies. As a result of the analysis of the literature on this topic and the clinical case, it can be concluded that doctors are not sufficiently aware of this pathology. nine0007
As a result of the analysis of the literature on this topic and the clinical case, it can be concluded that doctors are not sufficiently aware of this pathology. nine0007
| Conflict of interest Not specified. | Conflict of Interest None declared. |
References
- Belousova E.D. Cyclic vomiting / Belousova E.D. // Russian Bulletin of Perinatology and Pediatrics. - 2011. - No. 6. - P. 63-65.
- Davenport C. Cyclic vomiting / Davenport C., Zrull J., Kuhn C. et al // J. Amer. AcadChild. nineteen72.-N11.-P. 66-87.
- Kvashnina L.V. Acetonemic syndrome and neuroarthritic anomaly of the constitution in children: modern methods of correction / Kvashnina L.V. //Modern Pediatrics.- - No. 8 (80). - S. 49-54.
- Rashed H. Cyclic vomiting syndrome is associated with a distinct adrenergic abnormality/ Rashed H., Abell T.L., Cardoso S.
 // Gastroenterology. - 1997. - P. A910.
// Gastroenterology. - 1997. - P. A910. - Sapa Y.S. Syndrome of cyclic acetonemic vomiting [Electronic resource] / Sapa Yu.S. // Health of Ukraine. - 2001. - No. 5. – URL: http://www.health-ua.com/2001/07/ vomit.php (date of access: 10.2019).
- Shapovalova M.M. Pathophysiology of cyclic vomiting syndrome (literature review) / Shapovalova M.M., Drobysheva E.S., Ovsyannikov E.S. // Young scientist. - 2015. - No. 14. — S. 112-115.
References in English
- Belousova E.D. Tsiklicheskaya rvota // Rossiyskiy vestnik perinatologii i pediatrii [Cyclical vomiting] / Belousova E.D. // Russian Bulletin of Perinatology and Pediatrics, 2011.- N 6.- P. 63-65. [in English]
- Davenport C. Cyclic vomiting / Davenport C., Zrull J., Kuhn C. et al // J. Amer. AcadChild. Psychiatry. 1972. -N11.-P. 66-87.
- Kvashnina L.V. Atsetonemicheskiy sindrom i neyro-artriticheskaya anomaliya konstitutsii u detey: sovremennyye metody korrektsii [Acetonemic syndrome and neuro-arthritic anomaly of the constitution in children: modern methods of correction] //Sovremennaya pediatriya [Modern Pediatrics].