Bipolar partner making me crazy
Bipolar Relationships: What to Expect
Reviewed By:
Ups and downs are natural in any romantic relationship, but when your partner has bipolar disorder it can feel like you’re on an emotional rollercoaster. Not knowing what to expect each day is stressful and tiring. Over time, it wears on the relationship.
Understanding why your partner acts out sometimes or becomes withdrawn is the first supportive step you can take in strengthening your relationship. Learn exactly what a bipolar diagnosis means, how it could affect your partner’s behavior and what you can do to foster a healthy, stable relationship.
What does it mean if your partner is bipolar?
Bipolar disorder is a mental health condition marked by intense mood changes. People with the illness switch back and forth from mania or hypomania (an emotional state of being energetic and gleeful or sometimes aggressive or delusional) to having episodes of depression.
The lifelong condition tends to run in families, although the cause of bipolar disease is unknown. However, it can often be successfully managed through treatment. There are two primary types of bipolar disorder:
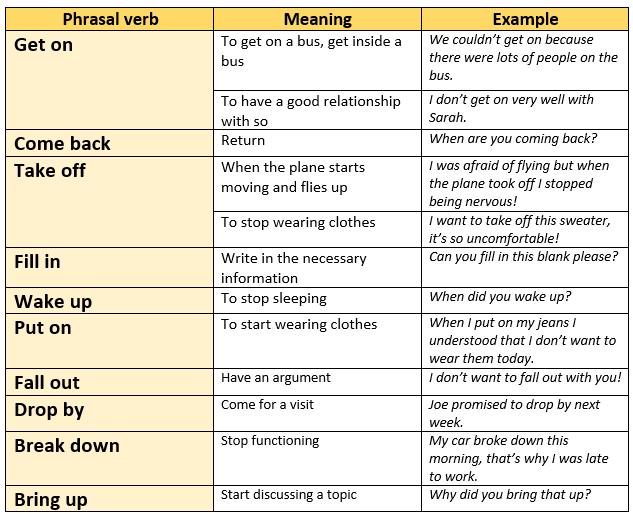
Bipolar 1
Bipolar 1 is a more severe form of the illness and is defined by manic episodes that have one of these characteristics:
- Hallucinations, delusions or paranoia
- Hospitalization required for safety
- Impulsive behavior with significant consequences
“When people are manic, they pursue pleasurable activities with great enthusiasm and with no regard for the consequences,” says Jennifer Payne, M.D., psychiatrist and director of the Women’s Mood Disorders Center at Johns Hopkins Medicine. “They may gamble, spend excessive amounts of money, use drugs or become promiscuous.”
Bipolar 2
People with bipolar 2 experience hypomanic episodes, which still include out-of-character behavior but aren’t as extreme as those with bipolar 1. Hypomanic episodes may include:
Hypomanic episodes may include:
- Increased energy and drive.
- Rapid speech.
- Decreased need for sleep.
“During hypomanic episodes, a partner with bipolar 2 may obsessively pursue sex with you or others,” says Payne. “They may stay up all night and have lots of wonderful ideas they want to tell you about at 3 a.m.”
Treatment Challenges
Bipolar disorder is usually treated with a combination of medications and therapy. However, successful treatment can be a challenge since many people miss the euphoria and energy of manic episodes.
Often people with bipolar disorder view these elevated mood states as their best selves — when they’re the most productive or creative — and will stop treatment in order to experience that again. Sometimes those with bipolar disorder will even intentionally trigger a manic episode.
“Lack of sleep is a trigger of manic episodes for a lot of people,” says Payne. “Sometimes patients with bipolar disorder will deliberately skip getting the sleep they need in order to initiate an elevated mood state. For example, a person might want the high energy that comes with a manic episode to get a project done.”
For example, a person might want the high energy that comes with a manic episode to get a project done.”
The key to your partner’s successful management of the illness is a commitment to continuing treatment and ongoing communication with their psychiatrist. This can take place at therapy sessions, during regular checkups or whenever necessary to discuss troubling symptoms.
Many people with bipolar 1 do well on lithium, a mood-stabilizing drug. Those with bipolar 2 may not fully respond to medications often used to treat bipolar disorder. If that’s the case for your partner, it’s important for them to continue to work with their psychiatrist to find an effective treatment.
Being in a Relationship with Someone Who Is Bipolar
There are certainly challenges in any romantic relationship, but bipolar disorder can make things especially difficult in various aspects of life:
Intimacy
It’s common for people with bipolar disorder to desire frequent sex during manic or hypomanic phases. Your partner may initiate intimacy much more than normal, or masturbate or use pornography more frequently than usual. Those with bipolar disorder may also engage in risky behaviors such as unprotected sex or extramarital affairs while manic.
Your partner may initiate intimacy much more than normal, or masturbate or use pornography more frequently than usual. Those with bipolar disorder may also engage in risky behaviors such as unprotected sex or extramarital affairs while manic.
During episodes of depression, your partner may avoid sexual contact altogether. This can be confusing or feel like rejection, especially if your partner recently desired lots of sexual activity during a manic or hypomanic period. Many medications for bipolar disorder can also lower sex drive.
Work
Your partner’s ability to perform well at work can be affected by bipolar disorder. Severe mood swings, along with manic symptoms such as poor judgement and impulsivity, or depressive symptoms such as low energy and disinterest make it tough to find and maintain a job. Stressors at work may also trigger or exacerbate your partner’s symptoms. If your partner can’t hold down a job, this could put more pressure on you to provide financial support until their illness is well-managed.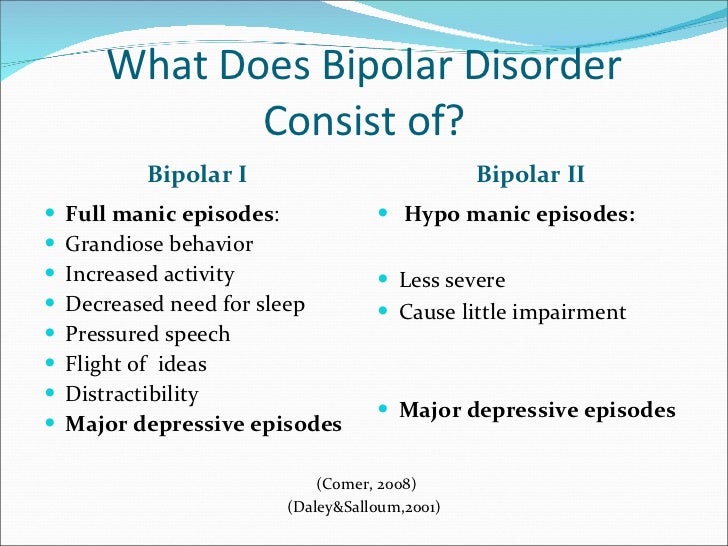
Parenting
Many people consider parenting the most stressful (albeit rewarding) job of their lives. But any kind of stressor — good or bad — has potential to trigger manic or depressive episodes for people with bipolar disorder.
In addition, the erratic behavior associated with bipolar disorder can be confusing and scary to children, who look to parents to provide stability. Helping your partner get and maintain treatment to control symptoms is crucial for providing a safe and secure home for children.
How to Make a Bipolar Relationship Work
It takes effort to keep any relationship strong, but it can be especially challenging when your partner has bipolar disorder. Payne offers these recommendations:
Go to Couples Counseling
Couples counseling is essential for working through upset over a bipolar partner’s actions. It’s common for someone with bipolar disorder to hurt and offend their partner. When someone is first diagnosed, there are often relationship issues that need to be addressed. Couples counseling can help you:
When someone is first diagnosed, there are often relationship issues that need to be addressed. Couples counseling can help you:
- Understand that there’s an illness involved in the hurtful behavior.
- Forgive the behavior that happened during an altered mood state.
- Set boundaries with a partner about maintaining treatment.
Get Involved with Treatment
Ask if you can be involved with your partner’s treatment, which may include occasionally going to the psychiatrist together. Being a part of your partner’s treatment has multiple benefits, including:
- Gaining a better understanding of the illness.
- Providing additional insight for the psychiatrist.
- Learning to spot signs of impending episodes.
- Alerting the psychiatrist about mood changes.
Even if your partner hasn’t signed off on you exchanging information with their psychiatrist, you can still report worrisome signs (the doctor just won’t be able to tell you anything).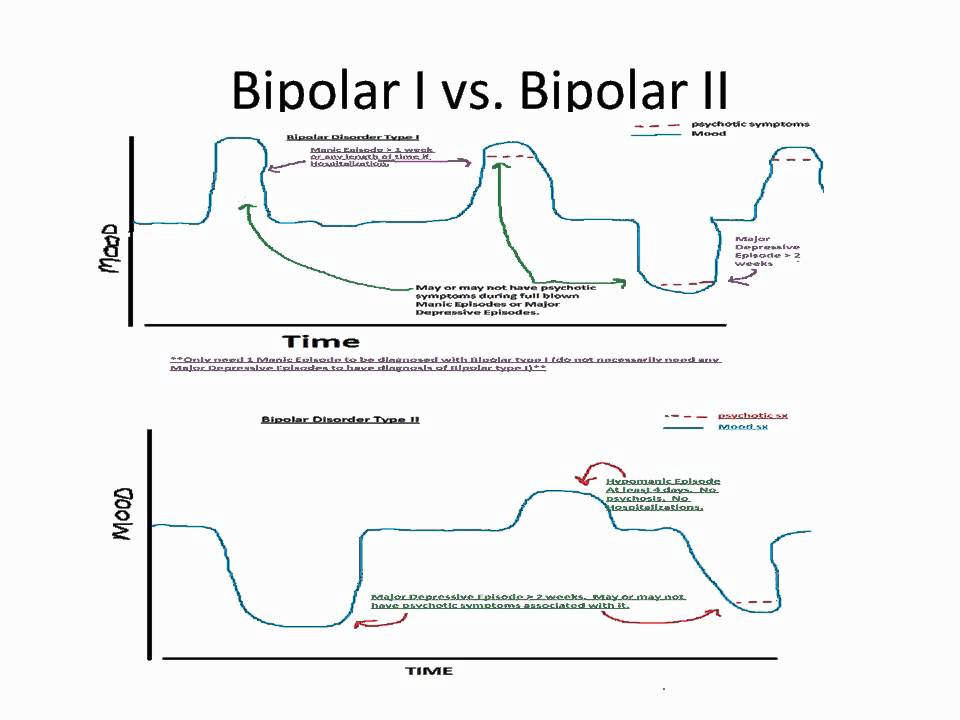 This gives the doctor a chance to make quick medication changes that may help your partner avoid being hospitalized.
This gives the doctor a chance to make quick medication changes that may help your partner avoid being hospitalized.
Practice Self-Care
Self-care gets a lot of buzz these days, but nowhere is it more important than when you’re caring for someone with a serious illness such as bipolar disorder. It’s essential to dedicate time to your own physical and mental health, whether that’s going to a support group, talking to a therapist or attending a yoga class.
Being in a healthy relationship with someone with bipolar disorder requires not only careful management of their illness, but also setting aside time to take good care of yourself.
Why Is My Loved One with Bipolar Suddenly Being Difficult and Unkind?
Post Views: 52,687
Views
Some mood episodes can cause behavior that is out of character and difficult to tolerate. We can help loved ones recognize and prevent these shifts before they damage our relationship.

Many people believe that bipolar disorder comes with only sad depression or euphoric mania. In reality, this is just 50% of bipolar disorder. The other side of bipolar includes symptoms of irritation, anger, restlessness, and a mean and nasty mood. This mood swing can be from either agitated depression, or an episode with mixed features, which I call dysphoric mania.
Typical Symptoms of “Mean and Nasty” Bipolar Episodes
- Physical restlessness.
- Anger at specific people whom you believe have done you wrong.
- Anger at businesses or governments who are not doing what you believe they should do.
- Physical anger—your arms and legs want to punch and kick whatever is around you.
- Talking more forcefully and sometimes more loudly than normal.
- A marked increase in cussing and language you would not normally use in a normal conversation.
- Blaming everyone, except yourself, for how you feel. (There’s a real lack of insight in this mood swing.
 )
) - Unable to see the positive; and when others point it out, these people seem stupid and unaware—and you let them know it!
- Extremely opinionated and aggressive with your opinions.
- Fully entrenched in confirmation bias. You will look for articles and information that match your unhappiness and prove your opinions.
Is It Agitated Depression or Dysphoric (“Mixed”) Mania?
Judging from my own experiences with these episodes, as well as with my clients, it’s not difficult to tell the difference between agitated depression and “mixed” episodes, which I call dysphoric mania.
Dysphoric mania comes with very obvious manic changes in energy: The person will sleep less and not be tired. You will see changes in spending, sexuality, volume and speed of talking; an inability to let others have opinions; aggression, and/or risk-taking behaviors.
If it’s agitated depression, the person will still sleep or will be very tired if sleep is disrupted. Agitated depression isn’t as physically energized as dysphoric mania. It doesn’t have an increase in spending or sexuality, and the person will not be as physically aggressive as a person who is in a mixed state.
Agitated depression isn’t as physically energized as dysphoric mania. It doesn’t have an increase in spending or sexuality, and the person will not be as physically aggressive as a person who is in a mixed state.
Another way to tell the difference is to look at the intensity of the symptoms. The symptoms themselves will be the same in each type of mood swing, but the intensity of the behavior will be much stronger in dysphoric mania than in agitated depression.
How to Help Yourself When You Have a “Mean and Nasty” Episode
Write down what you think, say, and do during one of these episodes (or have a close friend and/or family member help you, if you are dealing with lack of insight). Documenting what you think, say, and do can help you determine if it’s agitated depression or dysphoric mania. You can also use this list in the future to prevent the mood swing from going too far. I call this being a bipolar detective.
Here is an example of my think, says, does list from my last agitated depression:
What I said to others and wrote in my journal:
- The government where I live is so f—ing stupid.
 They are incompetent and I HATE them. They should all be fired! They lied to the press and caused enormous distress for all of us!
They are incompetent and I HATE them. They should all be fired! They lied to the press and caused enormous distress for all of us! - I can’t believe how dumb everyone is! People are sheep and they are stupid! They are blind and I can’t figure out how they can be so dumb!
- This life is too hard. It’s ridiculous that my life is so hard. I can’t find peace anywhere.
My behavior:
- I called friends and complained heavily about my life and the world.
- I couldn’t find a comfortable place to sit! Nothing felt right. Chairs were uncomfortable, and nothing was calming.
- Sleep was difficult. I wanted to sleep and I slept, but I woke up throughout the night and got up too early. I felt tired and stressed. (This is often called “wired and tired.”)
- I felt anger boiling in me, and I needed to release it somehow! I was mad at everyone!
- Sounds were too loud and people were really upsetting me with their loud talking and chewing and being stupid!
- I had trouble seeing the other side of a situation because I was right! People are blind and can’t see what I can see! They are making excusing for stupid people! I wanted to tell my friends they are just sheep and are being lied to!
I do NOT think like this at all when I’m stable. I’m not a mean or unkind person. This is a downswing. (My behaviors are exactly the same during dysphoric mania, but my energy levels are through the roof. I am much, much more aggressive during mania, including my driving behaviors.)
I’m not a mean or unkind person. This is a downswing. (My behaviors are exactly the same during dysphoric mania, but my energy levels are through the roof. I am much, much more aggressive during mania, including my driving behaviors.)
How I Ended the Agitated Depression
Writing my thoughts and behaviors down in my journal really helped me recognize that I was sick and I needed to help myself so that I wouldn’t ruin any relationships:
- I stopped talking about politics and world events.
- I tried to be nice to myself and remind myself that I have bipolar and this is simply a symptom. What matters is that I caught it—and that is a positive.
- I used the ideas in my books, Take Charge of Bipolar Disorder: A 4-Step Plan for You and Your Loved Ones to Manage the Illness and Create Lasting Stability, and Getting It Done When You’re Depressed: 50 Strategies for Keeping Your Life on Track.
- I apologized.
We Get “Mean and Nasty” Because It’s a Symptom!
When the world feels out of control, it’s natural that bipolar disorder would be affected. Sometimes this can lead to what we consider typical depression symptoms, such as sadness or lack of energy, but it can also lead to an irritated, nasty downswing called agitated depression, or a manic episode called “mixed” or dysphoric mania.
Sometimes this can lead to what we consider typical depression symptoms, such as sadness or lack of energy, but it can also lead to an irritated, nasty downswing called agitated depression, or a manic episode called “mixed” or dysphoric mania.
People with bipolar disorder get mean and nasty during agitated downswings or dysphoric manias because this is a symptom of bipolar disorder.
It’s not okay, and it doesn’t mean that we get to go around yelling and abusing people. But it’s important to know we’re not doing this on purpose.
I had this recent downswing because of having surgery. The stress and the anesthesia affected my mood. This is normal. I had a plan in place and caught the episode within 24 hours.
If you’re a loved one who wants help to communicate with someone in a “mean and nasty” mood swing, please read more about my Bipolar Conversation technique. It works!
We can teach ourselves to recognize, stop, and hopefully prevent “mean and nasty” mood swings!
Julie
Originally posted September 23, 2020
Read More:
20 Unexpected Signs of Bipolar Depression
aggression, agitated depression, mixed mania, mood management
About the author
Related
How love drives you crazy and what to do about it
Articles
Love - the same true love - should be dramatic, passionate and emotional. We do not notice the moment when passion turns into pathology. Sometimes love and unhealthy relationships can become a catalyst, the “last straw”, provoking manic, delusional, depressive and other conditions. ASI correspondent learned about the types of unhealthy relationships at a lecture by a psychiatrist, psychotherapist of the psychiatric hospital No. 1 named after N.A. Alekseev, candidate of medical sciences Elena Yurievna Onegina.
We do not notice the moment when passion turns into pathology. Sometimes love and unhealthy relationships can become a catalyst, the “last straw”, provoking manic, delusional, depressive and other conditions. ASI correspondent learned about the types of unhealthy relationships at a lecture by a psychiatrist, psychotherapist of the psychiatric hospital No. 1 named after N.A. Alekseev, candidate of medical sciences Elena Yurievna Onegina.
Health, Culture and education 05/22/2018
In classical literature, love is almost always described as a tragic feeling, lovers experience months and years full of dramatic events, and then either die or part, continuing to suffer all their lives.
To remember a novel or a poem about happy love that brings only joy and harmony, you will have to try hard.
From childhood, boys and girls absorb behavior patterns described in novels and drama series. Excessive jealousy, addiction, painful, codependent relationships, and more seem to be the norm until the situation gets completely out of hand. An expressive and passionate relationship on the part of one or both partners may not be a “crazy and beautiful love story”, but a pathology that a psychiatrist will have to deal with.
An expressive and passionate relationship on the part of one or both partners may not be a “crazy and beautiful love story”, but a pathology that a psychiatrist will have to deal with.
Obsessive Compulsive Love
This is the most common type of disorder. He is extremely masochistic and with him a person torments himself first of all, thinking about the object of love and suffering from uncertainty.
This is "thinking gum". If your close friend talks about how he is madly in love, how he thinks about the upcoming date day by day and tells you about this date when he endlessly imagines “how we will meet, how I will confess my love, and what will happen after that” . But in reality, absolutely nothing happens.
Psychotherapists say that there is nothing healthy and romantic about this rather common condition. This uncertainty can last for years.
Depressive love
A love drama typical of 19th century novels can be described as an example of depressive love.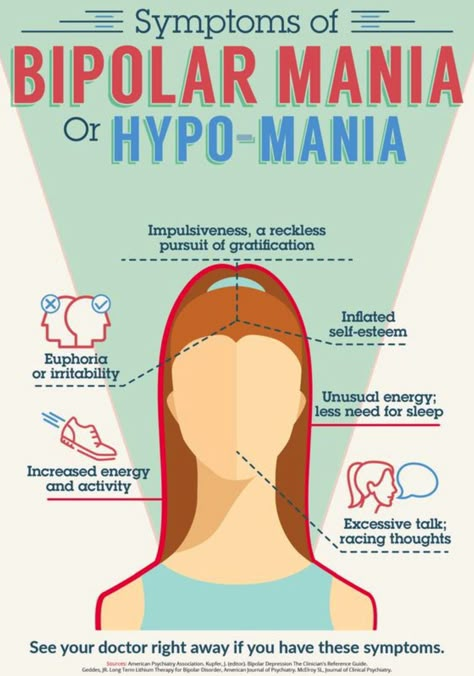 Almost all the heroines of Russian literature lost weight, turned pale, wringed their hands and suffered in every possible way. They stopped eating and fainted, instead of trying to communicate with the object of love, or at least try to live with it without harming themselves.
Almost all the heroines of Russian literature lost weight, turned pale, wringed their hands and suffered in every possible way. They stopped eating and fainted, instead of trying to communicate with the object of love, or at least try to live with it without harming themselves.
A happy story is boring, says the therapist. - If we take poetry, cinema, literature with you, then it will definitely be some kind of tragic plot with a bad ending, depressive love, which is so often sung in novels. And why talk about happiness, you can’t write poems and songs about it.
In case of depressive love, portrait descriptions of the hero of a love story can be written from a person. Psychosomatic symptoms make a person lose weight and turn pale, anxiety increases and there is a need for sedatives, there are disturbances in the functioning of other organ systems: the gastrointestinal tract, skin, and the cardiovascular system.
Manic love
Excessive euphoria, excitement, desperate dramatic acts for love, the need to share love with others and ignoring the feelings of the object of "blind love" are all signs of manic love.
The lover has a feeling that he is a godsend for his beloved, but at the same time he absolutely ignores his feelings and needs. Whom does a person love in these relationships: the object of love or himself - so wonderful and beautiful?
Bipolar relationships (codependency)
Bipolar relationships are absolute instability. What is called "I love it, I hate it." All this happens in accordance with the phases, which sometimes even depend on the change of seasons of the year, the psychiatrist claims.
“At one stage I accept my partner with all his strengths and weaknesses, at another he irritates me, I cannot forgive him for the slightest slight fault. Such love requires constant reinforcement and confirmation from the partner, constant words and actions expressing love, and this is impossible, ”says Elena Onegina.
Delusional love
Delusional love is the most difficult option. With her, a person in love loses touch with reality in the literal sense. He can talk about the fact that someone is in love with him, although in fact "love" exists only in his head. In this case, urgent psychiatric help is needed.
He can talk about the fact that someone is in love with him, although in fact "love" exists only in his head. In this case, urgent psychiatric help is needed.
There are many cases in which girls who are persecuted by men had to change their place of residence. This is already called stalking and it is very important to recognize it in the early stages.
Pathological jealousy
At a certain age it is very pleasant to be jealous. When they arrange scenes, when they ask: “Who is he, why is he calling you, and why is he writing to you, I don’t want him to call you, but I don’t allow ...”, quotes Onegin’s common phrases.
According to the psychiatrist, at some point ordinary jealousy turns into persecution. It becomes impossible to convey to a person that this is not the norm and one has to turn not only to a psychotherapist, but also to the police. In the classifier of diseases there is a special disease “alcoholic delirium of jealousy,” Onegin continues.
In contrast to ordinary jealousy, which can be removed by a heart-to-heart talk, persuasion and logical explanations do not work on a person suffering from a disease. Even if the girl says that the courier called her, the jealous person even then begins to see the catch and say that she specially persuaded someone and is deceiving again.
The most important thing is to recognize any of these pathologies or any other unhealthy moments in a relationship in time. And immediately go to a specialist who will help save the relationship and the health of both partners. In recent years, the situation has changed for the better even in budgetary neuropsychiatric dispensaries and there is an opportunity to undergo treatment while in a day hospital, without consequences in the further search for work and obtaining rights.
So if your partner, friend, or yourself is trapped in one of these pathologies or is experiencing other difficulties, advise him (or yourself) to see a therapist.
The lecture was held within the framework of the interactive psycho-educational project “I can't keep silent” in the space of the Blagosfera. The event was organized jointly with the Regional Public Organization "Psychiatrists Club" and Hospital No. 1 named after N.A. Alekseev.
how cognitive dissonance drives migrants crazy - Knife
Cheating on the homeland: how emigrants are driven crazy by cognitive dissonance - KnifeAs of 2017, Russia ranks third in the world in terms of the number of emigrants: there are 10.6 million of them. This is 7% of the country's population and 4% of the total number of those who, of their own free will or due to circumstances, left their native lands in search of a better life. Most of them are constantly in a state of cognitive dissonance. Many need psychological and psychiatric help.
ShareRepostTweet
From the Author:
“My family and I moved five years ago and within a year I was diagnosed with bipolar disorder. Trying to figure out the reasons, I read a lot of books and scientific studies and found a lot of evidence that immigrants do indeed face such difficulties more often. The theory was confirmed by practice: members of the Russian-speaking support group for people with mental disorders, which we organized, also called moving as the main reason for their illnesses.”
Trying to figure out the reasons, I read a lot of books and scientific studies and found a lot of evidence that immigrants do indeed face such difficulties more often. The theory was confirmed by practice: members of the Russian-speaking support group for people with mental disorders, which we organized, also called moving as the main reason for their illnesses.”
What are you complaining about?
Moving to a new country entails changes in all areas of life, so emigrants are more likely to have health problems, suffer from mental disorders, are anxious and pessimistic.
In 2002, Dr. Joseba Ahotegui of the University of Barcelona described the clinical condition of migrants with chronic or multiple stress as "Ulysses (Odyssey) Syndrome". Its manifestations include:
1) depression - sadness, tearfulness, guilt and thoughts about death;
2) anxiety - tension and nervousness, excessive anxiety, irritability and insomnia;
3) physical ailments - headache, fatigue, problems with the musculoskeletal system, discomfort in the chest and abdomen;
4) cognitive problems - memory and attention deficit, disorientation in time and space.
Research confirms that expats are exposed to numerous chronic stressors. Language and cultural changes, isolation, loneliness, a sense of "not belonging", a lowering of social status (lack of documents and job opportunities, poor living conditions), failures in a new country - all this depresses a person's adaptive abilities.
I emigrated several times: at 5, at 18, at 21 and at 26. My therapist and I believe that frequent moving at an early age is most likely the cause of my borderline personality disorder.
When my parents took me away from Russia, I found myself in complete isolation. I was a sociable child, and here for two or three years I talked only with mom and dad.
And then I went to school and found myself in an unfamiliar language environment and in a new cultural environment. I was in isolation for a long time and checked all my judgments with the point of view of my parents, because of which I became very dependent on their opinion.
I quickly began to adapt to those around me. For a long time, I actually didn’t have my own personality - there was only one that mirrored other people. This is how the survival mechanism worked.
If I had not adapted, I would have become an outcast, and I was very afraid of this. With each new move, my situation worsened. The last time I found myself in isolation again: I left all my friends in the UK and moved to Spain, where at that time I knew only my future husband and his colleagues. Because of this, I again fell into familiar patterns. I tried to contact at least someone - but did not get the closeness that I needed. My psyche became more and more shattered.
The matter is further complicated by the fact that, being isolated in an unfamiliar environment, I cannot find specialists who understand my problem. Very few psychotherapists have experience working with those who grew up in such a multicultural and multilingual environment.
Anna, chef, aged 35
The migration process requires constant adaptation to a new environment and is therefore considered one of the main chronic stressors.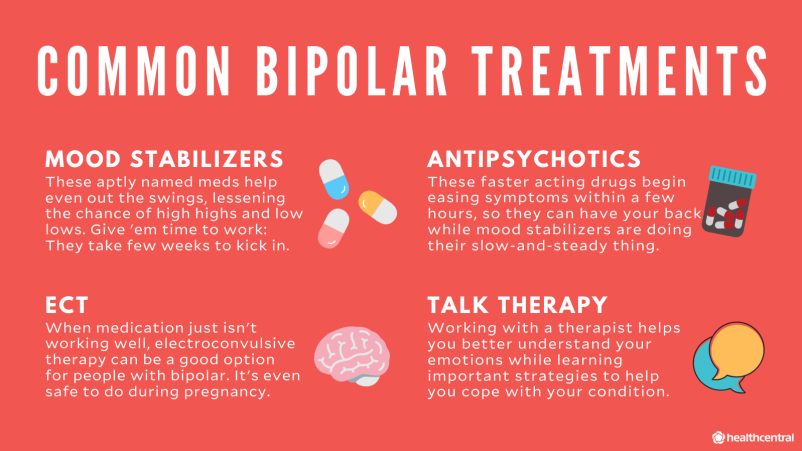 It can cause psychological or somatic problems and lead to the development of various pathologies, including post-traumatic stress disorder (PTSD), clinical depression, psychosis, and suicidal syndrome (including those with a tragic outcome).
It can cause psychological or somatic problems and lead to the development of various pathologies, including post-traumatic stress disorder (PTSD), clinical depression, psychosis, and suicidal syndrome (including those with a tragic outcome).
PTSD is diagnosed in 47% of emigrants. The risk group includes people who have traumatic experiences associated with moving to another country: racial discrimination, abuse by law enforcement officers, forced eviction, separation from family, detention, deportation. But often this disorder also occurs in those for whom the move went quite well.
Immigrants are at increased risk of developing schizophrenia and other non-affective psychotic disorders (NPD). Swedish researchers found that refugees are diagnosed with such diseases 66% more often than ordinary migrants from the same regions, and they are almost three times less common among representatives of the indigenous population of Sweden.
One of the main negative influences on mental health is the experience of discrimination.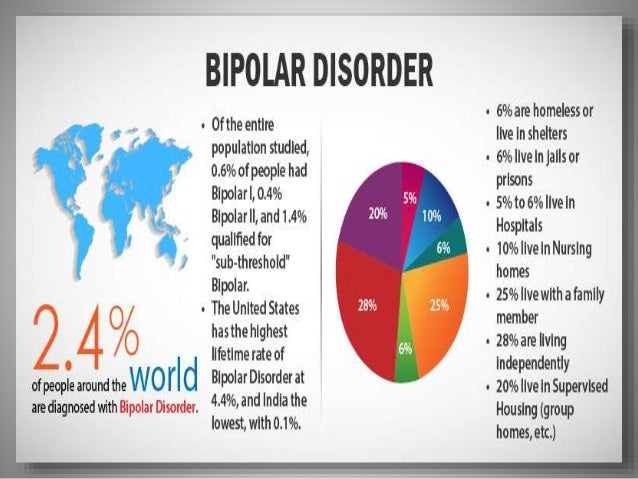 Migrants living in areas of low ethnic density are at increased risk of developing psychosis. Most often this happens in the least well-off and most discriminated groups.
Migrants living in areas of low ethnic density are at increased risk of developing psychosis. Most often this happens in the least well-off and most discriminated groups.
Moving to another country often provokes eating disorders. The tendency of migrants to lose weight may be due to the fact that they are in a state of stress, which has been found to arise from anxiety about their appearance. The level of adaptation in the host country is positively associated with eating disorders or the risk of other syndromes. That is, those emigrants (in particular, women) who are better at home are most susceptible to such diseases. And vice versa, migrants who do not strive for deep integration are less likely to be diagnosed with RPD.
Dr. Helen Fagan, who emigrated to England at age 12, suffers from post-traumatic stress disorder and depression. She believes that migrants and refugees are just as susceptible to PTSD as the military. And those who left their native country in adolescence live in a state of cognitive dissonance and experience problems with self-identification.
Case history
Leon Festinger, the author of the theory of cognitive dissonance, believed that this condition occurs in case of a conflict of established beliefs or values - for example, in logical contradictions, differences in cultures, when an individual opinion does not coincide with the general one or there is a discrepancy between the accumulated experience and the situation in which a person finds himself.
Dissonance, it seems to me, does not occur in everyone, but only in those who cannot live superficially. Outwardly, everything is just cool: a different country, new people, a lot of interesting things. This is enough for the first three to six months. Further, depth, understanding, development are needed - but there are none.
A lot of time and effort is spent on trivial things that you are not used to: how to get where, how to say it correctly, how to pay the bill, how to fill out a declaration, how to turn on the boiler, where to eat, where to go.
The head is constantly tense from a non-native language. You are in alert mode all the time.
There is no intimacy with people. Yes, you get to know each other, communicate, go out to hang out, you have many new friends - but there is no emotional return from communication. That's when, against the backdrop of already accumulated tension, dissonance occurs. Perhaps this is typical only for London, where it is considered bad manners to enter a person’s personal space, only ill-mannered people do this. But it was this "personal" thing that I missed the most.
Weeks passed when there were no emotional outbursts, either positive or negative. Everything is smooth. I even thought: it would be great if some cashier yelled at me. Maybe someone is looking for this “evenly”, but it drove me crazy.
There was a period when my hands dropped, there was no strength left. I sat at home, watched TV shows and ate ice cream. I went to work like hard labor, overcoming myself. In general, everything was given with difficulty.
Sitting at home without getting out, I ran away from reality, turned off. Then I realized that something was wrong.
I turned to a psychologist for help, rather out of curiosity, to check the British insurance system for lice. I insisted that I only wanted to work with a specialist who spoke my native language. As a result, I got a therapist of Russian origin, but my hopes for the notorious "understanding" did not come true. She diagnosed me with depression and was very surprised when I refused drug treatment.
Anna, Marketing Director, 34
An important condition for the emergence of cognitive dissonance is changes in lifestyle and status. They force people to correct (and sometimes reconstruct) the existing system of views and attitudes and internalize them.
Festinger believed that a person seeks to get rid of cognitive dissonance that causes him psychological discomfort, actively avoids situations and information that can aggravate his condition. Sometimes it becomes chronic and becomes a factor in irrational and maladaptive behavior.
Sometimes it becomes chronic and becomes a factor in irrational and maladaptive behavior.
Say A!
The problem is that I don't want to communicate with anyone. Instead, I chat on WhatsApp with my lover in Moscow and my girlfriends. Of course, you need to learn languages. It seems to me that when I comprehend them, I will become absolutely independent of everything: from love, from men, from fears. For now, I can't overcome the language barrier - I'm embarrassed to talk to other parents at school. And my child is afraid to communicate with children.
Masha, journalist, 38 years old
Cognitive dissonance may be due to different ideas about reality in certain languages and cultures, because one of the conditions for successful speech interaction is a similar background of the interlocutors.
Scientific research has shown that the better a person speaks the language of the host country, the higher the risk of PTSD. The effect of unfulfilled expectations is triggered: an emigrant is sure that in a new environment he will be able to cope with all the difficulties and adapt faster than someone who speaks a foreign language poorly or does not speak it at all. In the latter case, a person tries to neutralize the dissonance and achieve consonance - compliance. Through the study of the language, understanding of traditions, he finds the cause of his condition - and ways out of it.
The effect of unfulfilled expectations is triggered: an emigrant is sure that in a new environment he will be able to cope with all the difficulties and adapt faster than someone who speaks a foreign language poorly or does not speak it at all. In the latter case, a person tries to neutralize the dissonance and achieve consonance - compliance. Through the study of the language, understanding of traditions, he finds the cause of his condition - and ways out of it.
The most difficult thing was the forced silence. I am a sociable person, but here I could not talk to anyone - neither with the cashier, nor with the hairdresser. I was walking home from somewhere and did not understand how it was like that at all?
The absence of friends was the hardest thing to survive: there was no one to go to dinner with, play cards. Then we talked a lot with my husband's big family.
Food, or rather its quantity, caused complete dissonance. "Come in, we're drinking coffee - sorry, only two pieces of cake.
You won't have enough." Indeed, the amount of roast is calculated for the number of eaters. I continue from this ***** [fuck].
After the birth of my second child, I was overcome by panic attacks and an anxiety disorder. For more than three years I have been doing psychoanalysis with a specialist. We came to the conclusion that one of the main reasons for my condition is the experience due to the fact that, having overcome the numerous difficulties of emigration, I did not achieve anything and everything was in vain.
Julia, geologist, 41 years old
Causes of malaise
Adaptation is one of the stages of acculturation, which includes qualitative changes in various areas of migrants' lives. Language, culture, values, communication, gender roles, customs and social relations, art - on how great a person's desire to integrate into a new society, his psychological state will largely depend.
Professor John Berry believes that large differences between the original and new culture and the need for relearning can cause prolonged internal conflict and make adaptation difficult. He identifies several mechanisms of acculturation.
He identifies several mechanisms of acculturation.
1. Integration: people retain their culture and take on the features of a new one.
It is always easier to integrate into multicultural societies characterized by low levels of racism, ethnocentrism and discrimination. Although it has been proven that even those emigrants who have been in the country for a long time and have adapted to a new way of life continue to identify themselves with their native culture.
When I was 15, I went to study in Moscow, my parents sent me there. It was a different world to which I didn't fit at all. At the same time, my first symptoms appeared: tightness in the chest, lump in the throat, tinnitus, constant heartbeat. I went to the doctors, but no one diagnosed me.
Ten years later, when I changed my country, the symptoms reappeared, but with greater intensity, now accompanied by obsessions and hallucinations. Only here, in Europe, I was finally sent to the address - to a psychiatrist - and I began to be treated.
At first, I felt inferior, defective, subhuman. Everything was not as if a fish had been placed from fresh water into salt water: nothing seemed to have happened, the environment looked the same and even better - but she felt bad.
It was possible to overcome these barriers with great difficulty - from choosing yogurt in the store to maintaining a conversation when you cannot express your thoughts. I was angry with myself and tried to learn the language as soon as possible, make new acquaintances, explore the city so as not to get lost in it every time.
The difference of cultures, the feeling that you are a stranger, that you are not understood, permanent acclimatization (unaccustomed heat in summer and terrible cold in houses in winter), a strange taste of food, when you expect sweet, but get salty - all this led to the fact that I'm crazy. But now, five years later, I feel like a fish in water here, and it doesn't matter whether it is fresh or salty.
Sasha, journalist, 34 years old
2. Assimilation: an emigrant does not care about maintaining his own cultural identity and strives to fully acquire the features characteristic of the inhabitants of the new country.
Assimilation: an emigrant does not care about maintaining his own cultural identity and strives to fully acquire the features characteristic of the inhabitants of the new country.
It makes sense to choose such a strategy if a person does not plan to return to their homeland or, for example, is married to a representative of a different culture. Compared to other groups, those who have been able to assimilate are more likely to adapt to local etiquette, deal with setbacks more easily, and make friends with people of higher status.
I am a chameleon - I quickly adapt to the environment. I start dressing and acting like others, I meet new people with pleasure and interest, I study the customs and traditions of the country and try not to violate them.
I have close relatives in Israel, and they, of course, have friends who have become my friends. They also helped me with work - rather, to maintain my pants, but still.
However, my most important socialization happened in the gay community.
I met a guy on the Internet, and he said that there is a public organization Aguda that supports LGBT people in Israel, and there is a Russian-speaking group in it. I immediately got to their meeting - it was fantastic!
I didn't think that at 35 my circle of friends would expand. But that evening, eight or nine people came to the group, and I still keep in touch with five of them. My orientation helped me a lot to quickly integrate into a new society without the slightest problem. I'm sure if I were straight, the process would be longer and more difficult.
Max, businessman, 45
3. Separation: people remain faithful to their native traditions, refuse to integrate into a new culture and go into isolation.
According to the results of the study, 87% of the Turks living in the Netherlands choose this strategy, and they are more prone to clinical depression (20 participants versus 2 of those who preferred integration) and anxiety disorder.
I didn’t have bright illusions about emigration, because I knew exactly how hard and painful it is to settle down in a new place. The most difficult thing in adaptation is, firstly, the language barrier, and secondly, new spaces in which you have to get used to. I remember I went to the Gallery shopping center on Rustaveli - and I was seized by a panic: it is five times smaller than the Metropolis next to my house in Moscow.
I don't feel integrated because I didn't set myself such a task. I wanted to live, warm up and not get sick at least for a while due to a collapsed immunity against the backdrop of another stress. Few manage to integrate into the local society - this requires titanic efforts: to learn the language at the level of a native speaker, to know the culture and rules, to constantly communicate.
If a person is not ready to plow every day, he freezes at the time he emigrated and pupates in the Russian ghetto. There is even an Armenian proverb: “In what year he emigrated, in that year he remained.
” In love, I choose partners from my culture with a similar background. I would like to understand my own - where are the strangers.
Anush, writer, aged 27
4. Marginalization: a person does not want to follow the traditions of his culture and does not identify himself with the new one - he remains outside these paradigms. Such an acculturation mechanism is characterized by a high level of anxiety, a sense of alienation, and a loss of contact with both groups.
The more marginalized emigrants in the new society, the greater the risk to their psychological health. According to many researchers, such people constantly experience a sense of instability, are in a state of chronic nervous tension, they regularly experience mood swings. They doubt their place in the social structure, they are afraid of being rejected, they are tormented by dual experiences. The marginalized person feels unwanted, lonely, and detached.
I have been living in Amsterdam for nine years and I understand that it is not possible to fully integrate.
There is no feeling that you belong to any nation. I have not been Ukrainian for a long time and will never become Dutch. But millions of people are in this condition. This is becoming the norm.
Grisha, architect, 30 years old
In the case of cognitive dissonance, a person tends to actively avoid situations that may aggravate his condition. This property of the psyche makes many choose the path of separation or marginalization, including linguistic, cultural and even food. According to Berry, such a strategy only exacerbates the internal conflict.
Acculturation difficulties often force emigrants to resort to psychological or psychiatric treatment.
After moving to Barcelona, like many others, I had a conflict of two cultures - but not native and local, but Spanish and Catalan. I ended up not in Spain, as I planned, but in Catalonia. My brain completely refused to accept two new languages and two new cultures. I couldn't figure out what to spend time on.
Learn Catalan culture in Spanish? Or learn Catalan and forget about Spain? As a result, I gave up and resigned myself to the fact that I am an expat and will remain so.
It was necessary to earn a living, but there were difficulties with this: in the homeland there is a language, a crust about education, connections - after the move, all options were reset to zero.
Existence itself was burdensome, and the relatives and friends who remained in Russia did not understand what it meant to move to another country. It seemed to them that we had moved from rainy Moscow to a resort. This means that we should: a) have fun (and only fun!) talk about how we live here, b) welcome everyone and at the same time, because they probably miss them, c) walk with those who come from morning to evening (" The sea is right there, why are you sitting at home, what a job!”).
Instead of support, I often encountered people trying to take advantage of me. In most cases, they did not go to see me, but to Barcelona.
At some point, I locked myself in the room and stopped going out - everyone was so fed up. My husband brought me food to bed for several weeks.
We were looking for an apartment: our rental contract for the previous one ended, and the owners raised the price a lot. The search circle was also very narrowed by my requirements for housing. In addition, we were refused in many places because of documents: our student visas were being renewed.
For two months we wandered through the empty apartments of friends, constantly looking through ads in search of a suitable option. I began to panic: what if we have to move into a miserable kennel, or will we spend all the money, or will something else happen? It seemed to me that this would last forever. And when we nevertheless rented an apartment, I just finished. I was diagnosed with clinical depression.
Marina, director, 32 years old
Treatment abroad
Cognitive dissonance does not always act only as a barrier to socio-cultural integration - sometimes the search for the causes of disharmony, on the contrary, leads to understanding, rapprochement and empathy. In the process of building intercultural communication, as a rule, a person also comprehends cultural differences.
In the process of building intercultural communication, as a rule, a person also comprehends cultural differences.
The feeling of "wrongness" of what is happening accompanies anyone - it does not matter whether he is in his native country or in emigration. But in the latter case, due to the difference in cultures, such a feeling arises more often and manifests itself with greater force.
The adaptation was very difficult, if not brutal. The most difficult thing turned out to be learning the language, understanding the structure of the social system, coming to terms with the slow rhythm of life, with the fact that everything needs to be done in advance. Plus a complete vacuum, no friends, a minimum of connections, the child is with me from morning to evening. Emotionally it was very hard. After an active and eventful Moscow life, suddenly - absolute emptiness. Yes, now I am satisfied with the move, but before that I had to shed a lot of blood, sweat and tears.