Bipolar disorder abusive relationships
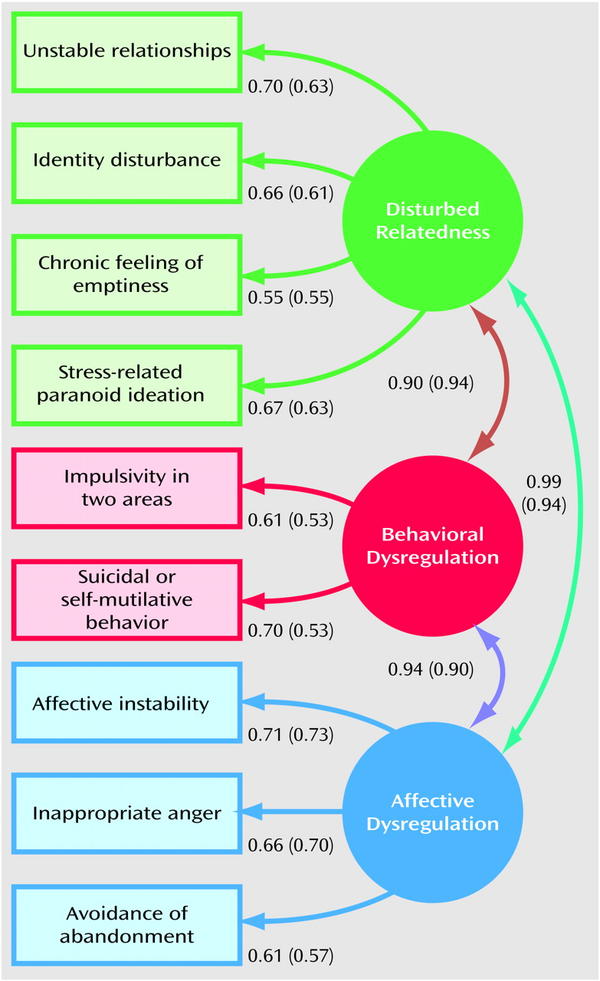
Abuse in Bipolar Relationships: Warning Signs
by John McManamy Patient Expert
Medical Reviewer
Jerry Kennard, Ph.D.
iStock
Medical Reviewer
Jerry Kennard, Ph.D.
iStock
The potential for abuse flows two ways in relationships involving one partner with bipolar and the other with “normal.” Typically, the abuser leverages the illness as a way of achieving dominance and control over his or her partner. In an abusive relationship, the behavior may start out innocently enough, but it never remains that way. Here are some of the warning signs.
Thinkstock
The “normal” partner: using the club
What may start out as an expression of interest and understanding in one’s illness may soon turn into a weapon of destruction. In no time, the “normal” partner refuses to recognize the other’s legitimate emotions and concerns and dismisses them as part of the illness.
Bottom line: You do not exist as a person.
iStock
The bipolar partner: using the excuse
What may begin with the bipolar partner being candid about his or her illness may soon turn into a justification for refusing to take personal responsibility. Often, the offending behavior has nothing to do with the illness or any other related condition.
Bottom line: No one likes to be exploited.
Thinkstock
The “normal” partner: being the sadist
Staying healthy involves taking sometimes elaborate precautions. This may involve getting to meetings well in advance or taking chill breaks or rigid sleep routines. The “normal” partner may work to defeat these efforts, typically through shame and ridicule, expressions of losing patience, and by not keeping to agreements.
Bottom line: Your distress has become your partner’s pleasure.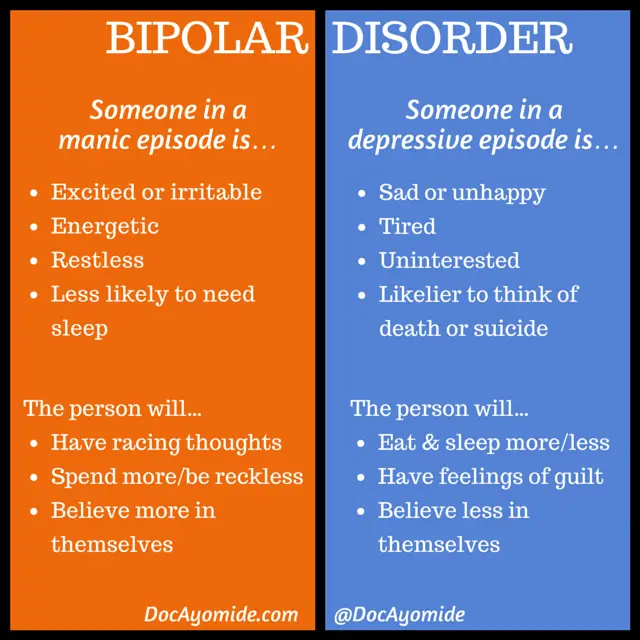
Thinkstock
The bipolar partner: being the prima donna
It is one thing for the “normal” partner to show consideration for the bipolar partner’s needs. It is another to put up with that individual’s selfish whims. From the setting of the thermostat to hogging the remote, the prima donna always has a bipolar justification.
Bottom line: You are the hired help in your own castle.
Thinkstock
The "normal" partner: playing superior
People with bipolar are constantly second-guessing themselves about how well (or not) they are fitting in. Over time, the “normal” one may assist by finding ways to undermine his or her partner’s confidence. Typically, the bipolar partner is reduced to being the “crazy” one, the deficient one, the social misfit. It’s a wonder the “normal” one even puts up with him or her.
Bottom line: It’s amazing how fast this can happen.
Thinkstock
The bipolar partner: playing superior
People with bipolar paint Sistine Chapels. “Normal” people work in offices. Everyone knows that, right? The bipolar partner may remind his or her “normal” partner of this at every available opportunity. In this context, the “normal” partner is reduced to being the stuck-in-the-mud, the deficient one, the social misfit. It’s a wonder the bipolar one even puts up with him or her.
“Normal” people work in offices. Everyone knows that, right? The bipolar partner may remind his or her “normal” partner of this at every available opportunity. In this context, the “normal” partner is reduced to being the stuck-in-the-mud, the deficient one, the social misfit. It’s a wonder the bipolar one even puts up with him or her.
Bottom line: Even “normal” people can be made to feel abnormal.
The Revealing Link Between Domestic Violence and Bipolar Disorder
How should you react to physical or verbal abuse from a bipolar spouse? Imagine you’re in a relationship with a person and you notice their behavior is changing gradually. They’re becoming more impatient — they may have a shorter temper. One day, you remind them of a project they said they’d do today and they react with anger and indignance, calling you names or even physically hurting you.
When a person with no history of this type of behavior suddenly becomes abusive, it can be unexpected and traumatic.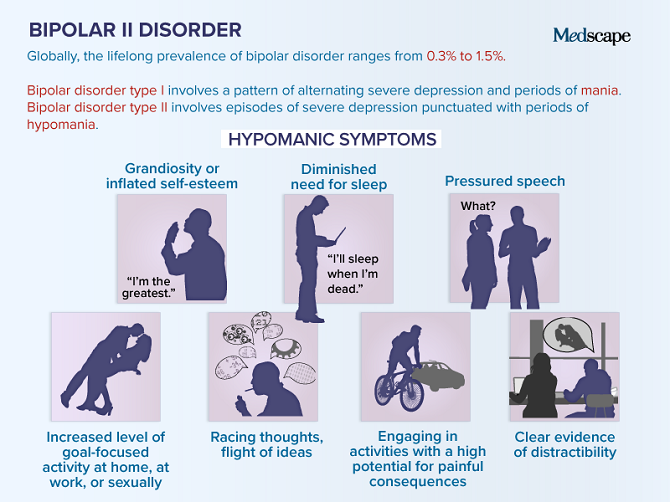 It can also be a sign of a serious mental health condition, such as bipolar disorder. Whether you knew about the condition previously or the changes are coming without warning, you may not know where to turn. At FHE Rehab, we’re here to tell you that you need to get help, no matter the circumstances.
It can also be a sign of a serious mental health condition, such as bipolar disorder. Whether you knew about the condition previously or the changes are coming without warning, you may not know where to turn. At FHE Rehab, we’re here to tell you that you need to get help, no matter the circumstances.
The issues discussed in this piece are sensitive. We’re not drawing conclusions about any single relationship where mental health and abuse are significant factors. We’re also not saying there’s any instance where a condition like bipolar disorder should be used as an excuse for domestic violence or that anyone should stay in an abusive relationship.
The Effects of Bipolar Disorder on Relationships
Bipolar disorder (BD) is a mood disorder that causes the person affected to fluctuate between manic periods of high energy and excitement and depressive periods of low energy, sadness and other symptoms commonly associated with depression. It’s a chronic brain disease that demands lifelong treatment, often involving medication to control changes in mood.
When your spouse or another close family member receives a bipolar diagnosis, it can be difficult to take. It may feel like the person you once knew isn’t there anymore, replaced by someone erratic and unpredictable. Living with someone who has bipolar disorder is difficult, but it’s important to remember: In many cases, with the proper treatment, they can live life in control and as the person, you know them to be.
The Prevalence of Physical or Verbal Abuse With a Bipolar Spouse
That being said, it’s impossible to ignore the statistics about domestic violence when one partner is suffering from bipolar disorder. One study performed in Sweden found that across the board, people suffering from mental and behavioral health conditions were more likely to perpetrate abuse against their partners. An article published in Psychiatric Times found specifically that people with BD are more likely to be violent toward other people in their lives.
But what does this link mean? A few explanations have to do with the behavioral changes that occur with BD.
As we’ve explored in the past, people with bipolar disorder are often in denial about changes in their behavior or personality. This may cause the person affected to see a partner’s attempts to be supportive of their condition as confrontational, causing them to lash out verbally or physically.
Uncontrollable Mood ChangesMost people who’ve been in a relationship understand how it feels when their own bad mood makes them easily annoyed by their partner. We might look back on arguments later and wonder what started them. For people with BD, this dynamic is taken to an extreme.
When a bipolar person is experiencing a manic episode, they may experience feelings of happiness and motivation, but this sudden burst of energy can also manifest itself in a negative way.
The same applies to behavior during a depressive episode. When a person is feeling low or depressed, they may experience apathy and stop caring about other people’s feelings temporarily, which may lead them to say something hurtful they wouldn’t otherwise say.
The delicate nature of a relationship is part of what makes it so amazing when people can share trust and love. However, when one partner is struggling to control their mood and behavior due to an untreated mental health condition, it can put the relationship’s stability on a knife’s edge.
Why Is It So Important?
If you’re in a relationship affected by a bipolar partner, your next steps should be made with your own best interests in mind. We would never recommend reconciliation in a case where one person is being physically or emotionally harmed by their partner.
With this in mind, it’s important that the abuser gets the help they need as well, especially if their behavior is unique to their bouts with severe BD. Here are a few of the main reasons why help is needed:
Avoid the Vicious Cycle of Mental Health and Abuse
There’s an explanatory link between relationship abuse and bipolar disorder. The Psychiatric Times article mentioned above cites that around 80% of people with bipolar disorder experienced one or more traumatic events earlier in their lives. This shows that abuse isn’t only the result of some cases of mental illness — it’s also the cause.
This shows that abuse isn’t only the result of some cases of mental illness — it’s also the cause.
Additionally, there’s a stigma that psychiatric patients are violent people, which harms the cause of raising awareness for these types of disorders. In most cases, patients not inherently violent or dangerous; they just need an increased degree of support.
Jails Can’t Support the Needs of People With Mental Health Conditions
Mental illness causes issues with impulse control and behavior. Physical and verbal abuse by a bipolar spouse often end up involving law enforcement, but the justice system doesn’t have the resources to support the needs of mentally ill people and get them the treatment they require.
As a result, mentally ill inmates tend to stay incarcerated longer. When they do get out, they find it more difficult to get a job or secure stable housing and as a result, often end up being rearrested.
Getting Treatment for Bipolar Disorder
When a bipolar spouse verbally abuses or hurts you, it’s a serious matter. If you don’t feel your issues are something counseling can fix without further harm to your physical or emotional well-being, you should leave. Additionally, your partner shouldn’t be able to use their condition as an excuse — domestic abuse is never okay and should always have consequences for the perpetrator.
If you don’t feel your issues are something counseling can fix without further harm to your physical or emotional well-being, you should leave. Additionally, your partner shouldn’t be able to use their condition as an excuse — domestic abuse is never okay and should always have consequences for the perpetrator.
But those consequences should look different based on the best interests of everyone involved. At FHE Health, our priority is making sure people struggling with the effects of bipolar disorder — either on themselves or the people around them — can access the support they need to live a healthy life.
How to support a loved one with BAD (bipolar affective disorder)?
People living with bipolar disorder need the support of family and friends. We will tell you how to help them and how not to harm them.
Anastasia Nikiforova
We have already talked about what Bipolar Affective Disorder (BAD) is and why it is so difficult to diagnose.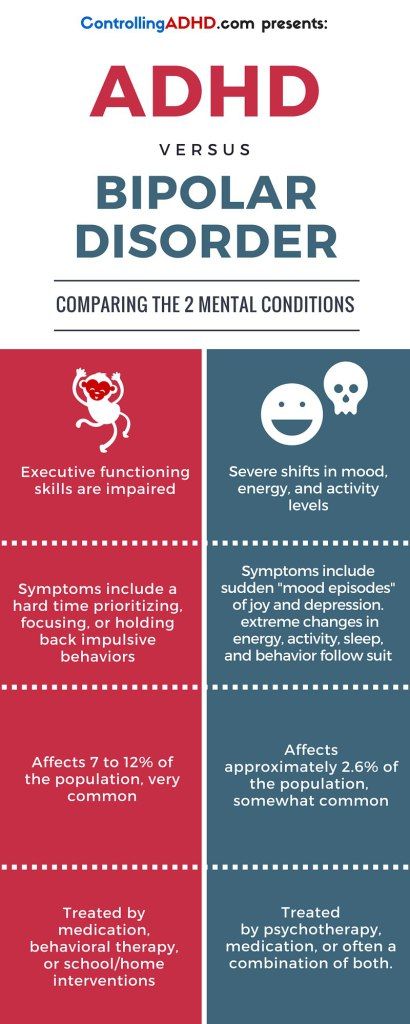 But what to do after the diagnosis is made? How to help your loved one? How to support and how not to harm?
But what to do after the diagnosis is made? How to help your loved one? How to support and how not to harm?
Do not self-medicate! In our articles, we collect the latest scientific data and the opinions of authoritative health experts. But remember: only a doctor can diagnose and prescribe treatment.
Bipolar disorder affects a person's mood, which means it will often fluctuate from extreme to extreme. Our loved ones will experience manias (periods of hyperactivity and increased energy), followed by periods of depression. Some people may experience hallucinations and delusions, up to psychosis.
It can be very difficult to support a person with bipolar disorder: contrary to our good intentions, a loved one may refuse help due to shame or unwillingness to accept their condition. There are ups and downs in any relationship, and the BAD of a loved one can complicate this process even more.
The editors of huffpost. com reached out to mental health experts and charities that help people fight mental illness. They got 9important tips on how to best support a loved one with bipolar disorder.
com reached out to mental health experts and charities that help people fight mental illness. They got 9important tips on how to best support a loved one with bipolar disorder.
1. Talk to a loved one about his or her experience
The stigmatization of mental illness and a distorted public perception of bipolar disorder may mean that people with this disorder are reluctant to seek help. If your loved one is sick, use a trusting relationship to help – discuss his or her experience with bipolar disorder. Feel your support and acceptance, ask questions about how you feel, be open to talking about your own mental health.
Create a "safe space" free of pressure or judgment.
The main thing is patience. Experiencing a manic or depressive episode can be frightening, especially if your loved one is "new" to their illness and has not yet sought help. You may not be fully aware of what your friend or relative is going through, but the very act of understanding is helpful.
2. Find out what bipolar disorder is
A good way to understand how your friend or family member might feel is to read about the experiences of people living with a bipolar diagnosis for a long time. For example, the UK bipolar community recommends The Restless Mind by Kay Redfield Jamison.
3. Remember your loved one's "warning signs"
It will be very helpful to learn and remember the "warning signs" of your loved one's transition from depressive to manic. Thus, if you notice individual "symptoms" in behavior, you can gently point out to your loved one that a manic episode is approaching.
General signs of mania can be as follows:
- increased energy;
- less sleep;
- more active spending of money.
But, of course, more individual signs are possible, for example, related to eating habits or social behavior.
The manic phase can be triggered by certain triggers. Here are the most frequent:
- somatic diseases;
- sleep disorders;
- serious problems in everyday life (with money, work or relationships) death of a loved one;
- break in relationship;
- physical, sexual or emotional abuse.
4. Be prepared for manic episodes
It is worth making a plan of action during manic episodes. When your loved one is feeling well, try talking to him or her about how support would be helpful.
You can discuss co-creation, art therapy or relaxation exercises, your help with stress reduction and cost control, support with daily routines, sleep and rest, regular meals.
5. Discuss behaviors that are challenging (but after the tide is out)
Don't be afraid to discuss behaviors that you find difficult to accept. Someone may become disinhibited during a manic episode, act rudely or act inappropriately, even offensively.
Someone may become disinhibited during a manic episode, act rudely or act inappropriately, even offensively.
It's good to talk about it - but choose the time of the conversation wisely. You shouldn't bring this topic up in the midst of mania. Calmly discuss your feelings when the "big water is gone" and your loved one will become more emotionally stable.
6. Find a balance between support and control
It is not uncommon for people with bipolar disorder to live under too much pressure from family and friends. It can be expressed in excessive control and criticality.
It is very important to support but not to control. Balance is not easy to find - we all want the best for our loved ones - but it is extremely important. Constant communication, respect and acceptance of each other's feelings helps to establish balance.
7. Stay calm and give comfort
When your loved one hears and sees something that you do not see, it can be a very scary and difficult experience for him. What should you do - support the delusion at the risk of deepening the state, or try to bring your loved one back to reality by upsetting him? Doctors recommend keeping calm and letting your loved one know that you realize that this is real for him.
What should you do - support the delusion at the risk of deepening the state, or try to bring your loved one back to reality by upsetting him? Doctors recommend keeping calm and letting your loved one know that you realize that this is real for him.
Provide support in feelings, without confirming or refuting the perception of reality by a loved one, because for him at these moments everything is very real.
Comfort and care can help your loved one feel seen, heard and appreciated. And disagreement or contestation, on the contrary, deepens alienation.
8. Seek professional help
If you are concerned about the behavior of a friend, relative or loved one, consider arranging a meeting with their doctor to discuss next steps. Your joint trip to the doctor will be a sign of support. You can make a list of specific behaviors that bother you ahead of time. This will help the doctor understand what's going on, especially if your loved one doesn't believe they have the disease.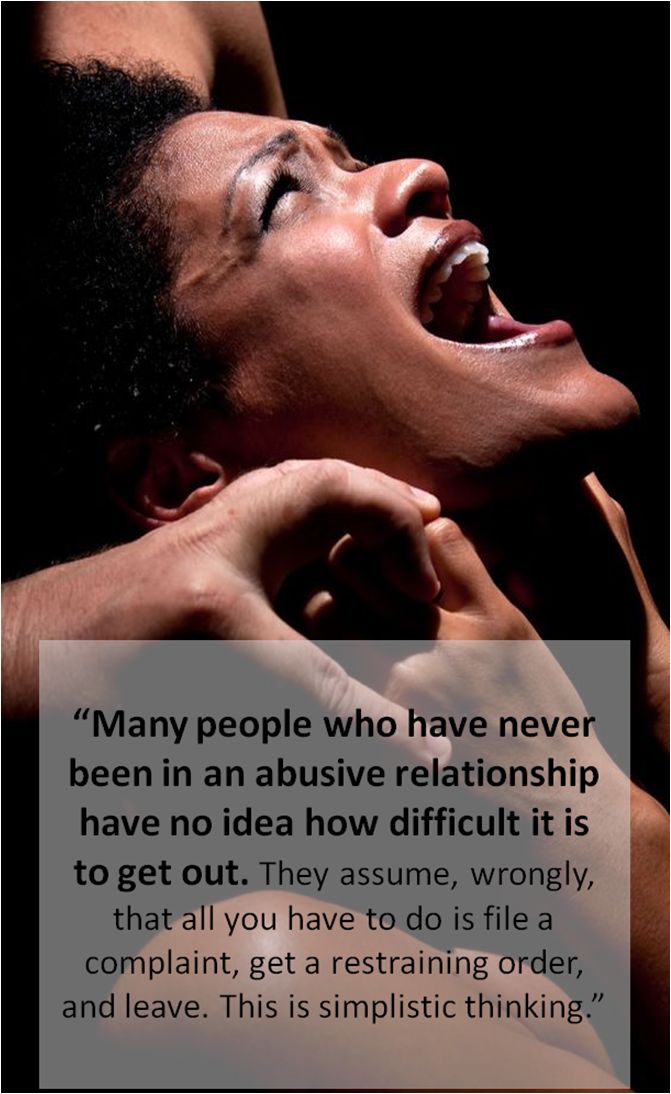
If the doctor has prepared a treatment plan and recommendations, it is worth making a copy of it so that you understand how you can help. In the treatment of bipolar affective disorder, early diagnosis and timely initiation of treatment are important. As a rule, it combines medication support, psychotherapy and self-management skills.
9. Take care of yourself
Worrying about someone close to you with a mental illness can cause you to put your own mental health on the back burner. All experts agree - you should remember to take care of yourself too. Emotionally burned out, you will not help anyone. Your strength can be devoured by guilt (for example, because you cannot help as effectively as you would like), rejection of important aspects of your own life, anger due to the illness of a loved one, loneliness.
If possible, contact a therapist or support group. Many people go through similar experiences, you don't have to "stew in your own juices". Communication and mutual support can give you new strength and reduce stress levels.
Communication and mutual support can give you new strength and reduce stress levels.
Have you experienced mental illness in loved ones?
How to survive in prison with bipolar disorder
Update
July 26, 2022
Follow us on Telegram
IN THE OPINION OF ROSCOMNADZOR, "UTOPIA" IS A PROJECT OF THE CENTER "NO TO VIOLENCE", WHICH, IN THE OPINION OF THE MINISTRY OF JUSTICE, FUNCTIONS OF FOREIGN AGENT
Why not?
Briefly
St. Petersburg artist Sasha Skochilenko was sent to a pre-trial detention center for an anti-war action - she pasted price tags on leaflets with agitation in the Perekrestok store. Now, while in prison, she has to prove not only her innocence of the crimes, but also her sanity, and at the same time the right to receive therapy - the girl has bipolar affective disorder. In the letter that Skochilenko handed over to Cherta, she talks in detail about the whole kitchen of forensic psychiatric examinations and prison psychological assistance - although the last word is hardly applicable here.
In the letter that Skochilenko handed over to Cherta, she talks in detail about the whole kitchen of forensic psychiatric examinations and prison psychological assistance - although the last word is hardly applicable here.
“I was handcuffed to the district PND”
There is serious discrimination against people with mental disorders in our penitentiary system. And in a sense, I'm glad that I had a chance to see what was happening with my own eyes - for a psycho-activist, this is a huge experience - and now I can tell you about it.
I have bipolar affective disorder, and due to severe depression that I experienced at 18, I almost accidentally got registered with the district PND (never tell government specialists that you have suicidal thoughts when you are depressed, if don't want that). Service at the PND never suited me, so for many years I was treated by private specialists, took medications as prescribed by doctors, and went to psychotherapy. And at some point she achieved a stable remission. I went to support groups, gave up bad habits, educated a lot in the field of mental health, participated in educational projects myself (for example, I illustrated the book by Masha Pushkina, which was published by the AST publishing house: “A Guide to Bipolar Disorder”, drew for the Partnership of Equals organization) . I even created colorful comics about my personal experience with the treatment of the disorder, which have attracted many psychiatrists and psychotherapists. In general, I was concerned with my own mental balance and well-being almost more than many of my compatriots.
I went to support groups, gave up bad habits, educated a lot in the field of mental health, participated in educational projects myself (for example, I illustrated the book by Masha Pushkina, which was published by the AST publishing house: “A Guide to Bipolar Disorder”, drew for the Partnership of Equals organization) . I even created colorful comics about my personal experience with the treatment of the disorder, which have attracted many psychiatrists and psychotherapists. In general, I was concerned with my own mental balance and well-being almost more than many of my compatriots.
Over time, I was deregistered in the district PND. To do this, you need to pass a bunch of tests and an interview with the chief medical officer, and then do the same again a year later, and if, as a result of these events, you are considered sane, your card will go to the archive. And then only in a few years, if you do not come into the view of the MHP again. My card went to the archive in the 17th year.
But after my arrest this April, she was taken out again. I was brought in handcuffs to the district PND, where I had a great conversation with the district psychiatrist - she poured me tea and yelled at my guard: “This is wrong! Where is our country headed? It's wrong to put a person in jail for this! What are you doing?!". She wished me luck, said that she would sign the petition for me, and solemnly established the fact of my sanity, which was not difficult.
Actually, it is a well-known fact, which Sherlock, who is investigating my case, is ignorantly ignorant of, that a person with bipolar disorder is absolutely sane, except when he is in the acute phase of psychosis (which is very difficult to achieve when you take care of your mental health about the same as me). People with bipolar disorder live the most ordinary human lives: they study, start families, work as doctors, teachers, civil servants, even psychiatrists. Until a certain point in life, a person may not know that he suffers from this disease.
However, my investigator, Mr. Proskuryakov, is clearly not very versed in the topic, and the fact that the PND established the fact of my sanity, as well as the fact that I had already passed the commission in the district PND, was not enough for him, so he insisted that I be sent for a forensic psychiatric examination.
But people under investigation are usually sent to the EIT when there are serious doubts about their adequacy, especially when it comes to a long-term inpatient examination. I know very few women from Arsenalka who were subjected to this event. So, one of the prisoners I know, who suffers from epilepsy and depression and was convicted under [Article] 228 of possession and distribution of drugs [of the Criminal Code], was assigned a three-hour outpatient examination. There is such an option, and it is often used, but the investigator immediately made it clear that this option was not for me. Perhaps this was done in order to humiliate me as much as possible, or in order to organize additional pressure on me - after all, the examination itself and the expectation of its results in total slowed down the paperwork for the whole two months of my further detention.
By the way, the fact of my sanity did not raise any questions from the staff psychologist of the pre-trial detention center, who gave me a general test for the detection of mental disorders. However, even this was not enough.
“It would be better if you stole something from the store”
And so, in June, I went to the City Psychiatric Hospital No. 6, where I lived under round-the-clock surveillance of cameras and endlessly passed tests and conversations with a psychologist and a psychiatrist. Most of the tests were already familiar to me, and it was also intuitively clear to me what specific “deviations” the questions of specialists probed. If life was preparing me for something, then it seems to be precisely for this.
For three weeks, I sorted pictures into categories, filled in empty bubbles in comics depicting people in conflict situations (from psychotherapy, I know that it is necessary to protect your personal boundaries, but express aggression in a targeted and correct way). I was asked to imagine what the hands in the pictures folded into certain gestures are doing, I explained the meaning of proverbs (people with schizophrenia, for example, often do not understand the figurative meaning), filled out a general test for the identification of mental disorders (again!) and interviewed a psychiatrist.
I was asked to imagine what the hands in the pictures folded into certain gestures are doing, I explained the meaning of proverbs (people with schizophrenia, for example, often do not understand the figurative meaning), filled out a general test for the identification of mental disorders (again!) and interviewed a psychiatrist.
In conversations with a specialist, in response to leading questions, I tried to emphasize that I experience a wealth of feelings and affects, and do not dwell on them, I do not have manic ideas of grandeur or paranoid thoughts. I have stable social connections, am capable of empathy, am in a long-term non-abusive relationship and stable remission. In the ward, she behaved calmly and friendly, socialized with other subjects...
The commission also faced questions regarding the motives of my "great crime", my ability to realize responsibility for it, as well as signs of remorse for what I had done. It seems to me that the standard templates of forensic psychology were applied to me, which I think apply to thieves, murderers, rapists and swindlers. This is how peacefulness and anti-war agitation are easily and naturally built into the list of criminal deviations from the conditional law-abiding norm, and the characteristics of people who commit such "crimes" will gradually be included in Russian textbooks on the psychology of crime, and hardly anyone will interfere with this.
This is how peacefulness and anti-war agitation are easily and naturally built into the list of criminal deviations from the conditional law-abiding norm, and the characteristics of people who commit such "crimes" will gradually be included in Russian textbooks on the psychology of crime, and hardly anyone will interfere with this.
But let's get back to the examination. As a result, I was interviewed by an impressive panel of five doctors and one "special consultant". I have not heard that this person was present at the commission of my other cellmates, and it seems that he came almost specifically on my case. He asked me questions for a long time, sneered at my deed (“It would be better if you stole something from this store ...”) and gave me a couple of compliments. The next day I went to the pre-trial detention center with a note on the card that I was sane and did not need medical treatment.
In the pre-trial detention center, everyone was persistently interested: is “everything is all right” with me? I think if the commission had not established the fact of my sanity, this would have been to the advantage of many, since all my complaints, statements and news in the media would have turned into a “pumpkin” overnight and I would have been easily written down as “untrustworthy sources” . Therefore, the next day after arriving at the SIZO, I had an interview with another psychiatrist, who - guess what? - again testified to the fact of my sanity.
Therefore, the next day after arriving at the SIZO, I had an interview with another psychiatrist, who - guess what? - again testified to the fact of my sanity.
To be honest, I have never in my life had to confirm the fact of my mental balance so often and so successfully as during these three months, and all because I once had a chance to tell a government doctor about my depression. As someone who has come such a long way in the struggle for their mental well-being, such an obsessive and obsessive interest in the issue of my mental health seems to me insulting and unnecessary. As a psychiatrist from the pre-trial detention center put it: “What do we have now, dissent is considered a mental illness?”
And this pitiful and small "stamp" about insanity has a very strong effect on a person's status in the penitentiary system. Based on the fact of insanity of the individual, established by the commission, the court may decide on compulsory treatment. But at the same time, the fact of the presence of a mental disorder cannot under any circumstances become the basis for changing the preventive measure. Although the inhumanly stressful conditions of detention may provoke the same psychosis or general deterioration in the individual suffering from the disorder. And people who find themselves in custody and investigation for months or even years will not receive any special help and care for their mental health.
Although the inhumanly stressful conditions of detention may provoke the same psychosis or general deterioration in the individual suffering from the disorder. And people who find themselves in custody and investigation for months or even years will not receive any special help and care for their mental health.
Helping the investigation, not the person
SIZO-5 has two full-time psychologists, very specific ones. One offered me a consultation, but could not arrange a comfortable and confidential environment for her, and instead suggested "whispering in the hallway." Then she admitted: “Our main task is to find out why you pasted the price tags.” That is, her task is not to provide psychological assistance to a person, but to help the investigation. How can you build trust in such a psychologist? For some reason, the second psychologist gave me a test on the knowledge of what criminal or administrative penalties an individual can face for crimes related to terrorism. Then, for some reason, the same psychologist insistently invited me to church.
The very attitude towards sub-experts in the FSIN system leaves much to be desired.
For example, upon my arrival at the examination at GPB No. 6, several employees in uniform spied on how I was changing. Subsequently, one of them, introducing himself as Petrov, tried to convince me that a) this did not happen, it just “felt” to me b) the FSIN officers “have no gender”, they are “like doctors”, therefore they can observe the subject at any time “by security considerations."
Drawing of Sasha made in prisonWhen we were taken to the doctors, the staff could eavesdrop on our conversations or intervene in them, give birth to self-ridicule jokes about our statements. One of the employees interfered in my conversations with the lawyer while he was watching our meeting.
There was a feeling that people in uniform perceived the subjects as their own entertainment and amusement. Some employees did not give their names, explaining this for reasons of "own security.