Zinc mental health
How it Helps Anxiety and Depression I Psych Central
Zinc is an essential nutrient that has many health benefits, including helping to reduce symptoms of anxiety and depression for some people.
Many factors can contribute to feelings of anxiety and depression. While stress, hormones, or genetics often play a role in these feelings, diet can also affect our mood.
Not getting enough specific minerals and nutrients can throw a wrench in how we feel. This includes getting enough zinc in our daily diet.
Zinc is essential for physical function, but it may also play a role in mental wellness. Maintaining adequate zinc levels can improve your overall well-being, helping you feel healthier and happier.
Zinc is crucial for brain growth and development and several other body functions, including:
- immune function
- protein synthesis
- DNA synthesis
- wound healing
- cellular health
- general growth and development
The body can’t produce or store zinc on its own, so it must come from your diet or supplements.
Zinc is generally obtained through a variety of plant and animal foods. Foods that don’t have zinc naturally, such as baking flour and snack bars, often contain synthetic forms of zinc.
You can also find supplements with zinc.
Because zinc plays a role in immune function, it can also be found in various cold medications, lozenges, and nasal sprays.
Zinc not only plays an essential role in the way our immune system functions, but it also affects our neural (aka brain) processes, according to a 2017 study. The study also links zinc and specific hormones or neurotransmitters — namely our “happiness” hormones, serotonin, and dopamine.
According to a 2021 study, zinc does this by helping elevate levels of brain-derived neurotrophic factor (BDNF) in the areas of our brain that control our emotions. When zinc is in low supply, BDNF levels drop, and so does our mood.
Other research supports this, finding ties between zinc and anxiety across different groups of people:
- A 2011 study suggests that low levels of zinc may lead to lower gamma-aminobutyric acid (GABA) levels in the brain — a neurotransmitter that blocks specific signals to reduce fear, worry, and stress.
 Zinc supplementation can help raise levels of GABA, thereby improving symptoms of anxiety.
Zinc supplementation can help raise levels of GABA, thereby improving symptoms of anxiety. - A 2019 study found that regular use of multivitamin mineral supplements may improve anxiety in young adults between ages 18 and 24.
- In a 2019 study of Japanese workers, mental health conditions and diet were linked, with researchers concluding that low levels of zinc, magnesium, and copper contributed to feelings of depression and anxiety for workers.
- A 2020 study suggests that zinc deficiency in older adults was tied to higher rates of depression and anxiety. A 2021 study of this age group showed that using zinc supplements significantly reduced signs and symptoms of anxiety and depression.
Studies have also linked low levels of zinc and depression.
A 2017 review reported that several studies found a link between lower levels of zinc and depression. It also found that adding zinc supplementation in combination with other treatments may help improve symptoms of depression.
According to a 2011 review, zinc may improve signs of depression or mood disorder because it helps reduce inflammation, inhibiting brain function and cognitive performance.
When our bodies get enough zinc, inflammation is reduced or eliminated, and our immune and brain systems can function at peak levels, which all contribute to a healthier body and mind.
Maintaining healthy zinc levels can have a positive impact on your overall physical and mental well-being.
According to the National Institutes of Health (NIH), besides reducing symptoms of anxiety, zinc may also help:
- support immune function
- promote wound healing
- treat or prevent chronic diseases such as diabetes, high blood pressure, and metabolic syndrome
- prevent age-related macular degeneration or vision loss
- promote sexual health
- treat diarrhea
- maintain healthy skin
- treat acne
- prevent osteoporosis
- reduce common cold symptoms
- treat neurological symptoms
- boost cognitive function
- reduce inflammation
- lower risk of infection
How much zinc do I need?
The appropriate amount of zinc you should be getting each day generally depends on your age and gender.
The recommended dietary amount (RDA) is as follows:
- Adult men: 11 mg
- Adult women: 8 mg
- Teen boys (ages 14 – 18): 11 mg
- Teen girls (ages 14 – 18): 9 mg
- Children (under age 13*): 2 mg – 8 mg
The RDA of zinc for women who are pregnant or nursing may be higher, so it’s important to talk with your doctor about how much you need.
*Babies and children need less zinc than teens and adults. Talk with your child’s pediatrician for more information and to make sure your child is getting the right amount for their age.
There are multiple ways to get your recommended daily amount of zinc. The easiest is through diet. Many foods contain enough zinc to meet your RDA, and they’re likely items you already eat regularly.
Zinc-rich foods include:
- red meat
- fish and seafood such as crabs and oysters
- poultry
- nuts and seeds
- beans, chickpeas, lentils, and other legumes
- certain vegetables such as mushrooms, asparagus, and kale
- eggs
- milk and other dairy products
- whole grains
- certain fortified foods such as breakfast cereals and snack bars
Supplements are another way to get your daily dose of zinc, particularly if your diet isn’t cutting it.
Zinc supplements can be especially helpful for those who have or are at chance of having zinc deficiency. According to NIH, this can include:
- people with gastrointestinal diseases such as Crohn’s disease
- women who are pregnant or nursing
- vegetarians or vegans
- people with sickle cell anemia
- older infants who are exclusively nursing
- people with chronic kidney disease
- those who misuse alcohol
There are several types of zinc supplements, and they can come in various formats, including capsules, tablets, liquids, and even topicals.
Dosage can depend on your current diet and zinc levels, so you may consider speaking with your doctor before adding a zinc supplement to your routine. They can recommend specific types and amounts tailored to your needs.
Getting too much or too little zinc can lead to some serious — and seriously unpleasant — side effects.
Nearly 1 billion people worldwide have some level of zinc deficiency due to not having enough zinc in their diet, according to a 2015 study. While more severe cases are rare, not getting enough zinc can still wreak havoc on your health.
While more severe cases are rare, not getting enough zinc can still wreak havoc on your health.
Zinc deficiency can cause:
- weakened immune system
- cold symptoms
- skin rash
- skin ulcers
- weight fluctuations
- diarrhea
- poor concentration
- hair loss
- vision problems
- breathing problems
A 2017 review also suggests that low zinc levels can increase your chance of contracting infections, including pneumonia, malaria, tuberculosis, and HIV.
Getting too much zinc can also create issues, including toxicity. Zinc toxicity can be serious and can cause various acute or chronic side effects, such as:
- cramps
- diarrhea
- changes in appetite
- changes in cholesterol levels
- weakened immune function
- nausea
- vomiting
- headaches
High levels of zinc are often caused by supplement use. Figuring out supplement dosage can be tricky because you also need to account for the zinc you’re getting through your diet. Taking too much zinc can increase your levels and lead to toxicity.
Taking too much zinc can increase your levels and lead to toxicity.
A 2015 study shows that too much zinc can also affect how your body absorbs copper and iron — two other essential minerals. Excessive amounts of zinc can even lead to a copper deficiency.
Zinc can also interfere with the effectiveness of some medications, including antibiotics and diuretics.
Zinc is an essential nutrient that supports many of our body’s functions, including immune function, cellular health, and certain brain functions.
It can also affect our mood, with zinc deficiencies often linked to anxiety and depression. By maintaining proper zinc levels, we can help improve our overall well-being.
Because our bodies don’t produce zinc, it must come through outside sources, such as diet or supplements.
It’s crucial to be cautious when using zinc supplements — it can be easy to overdo it. This can lead to zinc toxicity, which can cause immune issues, cramping, and changes in your cholesterol.
If you’re experiencing symptoms of anxiety or depression, consider speaking with a healthcare or mental health professional.
They can work with you to determine whether a zinc deficiency is behind how you feel or whether there’s another underlying cause. They can then help you develop a treatment plan tailored to your unique needs.
Effects of Zinc Supplementation in Patients with Major Depression: A Randomized Clinical Trial
Iran J Psychiatry. 2013 Jun; 8(2): 73–79.
, MS,1, PhD,2, MD, PhD,1, PhD,1, PhD,1, MD,3, MSc,4 and , MD4
Author information Copyright and License information Disclaimer
Objective
Major depression is a mood disorder that causes changes in physical activity, appetite, sleep and weight. Regarding the role of zinc in the pathology of depression, the present study was aimed to investigate the effects of zinc supplementation in the treatment of this disease.
Methods
This study was a double-blind randomized clinical trial. Forty four patients with major depression were randomly assigned to groups receiving zinc supplementation and placebo. Patients in Zinc group received daily supplementation with 25 mg zinc adjunct to antidepressant; Selective Serotonin Reuptake Inhibitors (SSRIs), while the patients in placebo group received placebo with antidepressants (SSRIs) for twelve weeks. Severity of depression was measured using the Beck Depression Inventory at baseline and was repeated at the sixth and twelfth weeks. ANOVA with repeated measure was used to compare and track the changes during the study.
Results
The mean score of Beck test decreased significantly in the zinc supplement group at the end of week 6 (P < 0.01) and 12 (P < 0.001) compared to the baseline. The mean score of Beck Depression Inventory reduced significantly compared to the placebo group at the end of 12th week (P < 0.05)
Conclusion
The results of the present study indicate that zinc supplementation together with SSRIs antidepressant drug improves major depressive disorders more effectively in patients with placebo plus antidepressants (SSRIs).
Keywords: Major depressive disorder, Zinc supplement, placebo and Selective Serotonin Reuptake Inhibitors (SSRIs)
According to the criteria of Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), major depressive disorder (MDD) is a psychiatric disorder with genetic, biological, and environmental risk factors. This disorder is one of the most common diseases in the world, with high levels of associated mortality. It affects people of every region in every ethnic group (1, 2) to the extent that one out of every 5 people referred to a physician is affected by depression (3).
About 19-34% of patients with depression do not respond to antidepressants, and 15-50% of them have a recurrence; therefore, other medications or supplementation with micronutrients are increasingly adjunct to antidepressant drugs to improve their therapeutic effects (4).
Zinc is one of the micronutrients involved in behavior, learning and mental functions. The first clinical studies in the field of serum zinc level in depressed patients have been published by Hansen and colleagues (5). The first report on the relationship between zinc status and brain function in humans has been published in 1998 by Sand stead and colleagues (6). Various studies have identified the effects of zinc in the pathophysiology of depression and antidepressant drugs mechanisms of action. Also, other clinical studies have shown low serum zinc concentrations in patients with depression (7).Furthermore, Long-term treatments with zinc in laboratory animals have had the same mechanisms and effects as the antidepressant drugs (8).
The first clinical studies in the field of serum zinc level in depressed patients have been published by Hansen and colleagues (5). The first report on the relationship between zinc status and brain function in humans has been published in 1998 by Sand stead and colleagues (6). Various studies have identified the effects of zinc in the pathophysiology of depression and antidepressant drugs mechanisms of action. Also, other clinical studies have shown low serum zinc concentrations in patients with depression (7).Furthermore, Long-term treatments with zinc in laboratory animals have had the same mechanisms and effects as the antidepressant drugs (8).
In previous studies, the dietary micronutrients as confounding factors have not been studied. However, the present study was designed to examine the effects of zinc supplementation in patients with major depression, while assessing and controlling dietary intake. The present study was the first randomized clinical trial in Iran designed to examine the effects of zinc supplementation in patients with major depression.
Participants and Procedure
This study was a double blind randomized clinical trial that was performed on 44 patients with major depression. Study population was among people with depression who were referred to the psychiatric clinic of Imam Hussein, Tehran. Sampling started after obtaining approval from the ethics committee of Nutrition Research Institute, Shahid Beheshti University of Medical Sciences (No. t/1/044).
The patients were aged 18-55 years. The inclusion criteria included diagnosis of major depressive disorder by a psychiatrist based on DSM-IV-TR, obtaining informed consent from the patients, no supplements usage at least four weeks before the study, not taking any medication except for those associated with depression status. The exclusion criteria included pregnancy or lactation, severe psychotic symptoms, changing drug class, symptoms requiring hospitalization including suicidal thoughts and actions.
Patients were randomly assigned in to two groups. One group received 25-mg zinc supplement daily with Selective Serotonin Reuptake Inhibitors (SSRIs) antidepressants (citalopram 20-60mg per day or fluoxetine 20-60mg per day), and the other group received placebo (containing Malto-dextrose) plus an antidepressant SSRI (citalopram 20-60mg per day or fluoxetine 20-60mg per day). The groups were blinded to the researchers and patients.
One group received 25-mg zinc supplement daily with Selective Serotonin Reuptake Inhibitors (SSRIs) antidepressants (citalopram 20-60mg per day or fluoxetine 20-60mg per day), and the other group received placebo (containing Malto-dextrose) plus an antidepressant SSRI (citalopram 20-60mg per day or fluoxetine 20-60mg per day). The groups were blinded to the researchers and patients.
Demographic data form was completed at the baseline. Inclusion and exclusion criteria and disease background were evaluated by research team. The Beck Depression Inventory (9), physical activity questionnaire, three-day dietary recall, and anthropometric indices were completed in the beginning, middle and end of the study. Nutritionist IV software was used to analyze a three-day dietary recall. Macro and micronutrients intake was derived from the three-day dietary recall and compared between the two groups.
Also, at the beginning and end of the study, a blood sample of 5 ml was taken after a 12-hour fasting state. Serums were separated and zinc concentrations were measured by flame atomic absorption spectrophotometry.
Serums were separated and zinc concentrations were measured by flame atomic absorption spectrophotometry.
Statistical Analysis
Sample size was determined so that 11 score difference in the mean of Beck score could be detectable, while comparing zinc and placebo groups with α = 0.05 and 1-β = 80%. In all, a sample size of 18 was detected to be sufficient. However, to cover at least 20% drop out which is common in clinical trials, a sample size of 22 subjects was determined for each group.
Data analysis was performed using SPSS version 16. The Kolmogorov - Smirnov and chi-square tests were used to determine the normal distribution of quantitative data and to compare qualitative variables between the two groups, respectively. In the case of quantitative variables with normal distribution for comparison between the beginning and end of the intervention within each group, paired t-test, and for comparison between the two groups at the beginning or end of the intervention, t-test were used.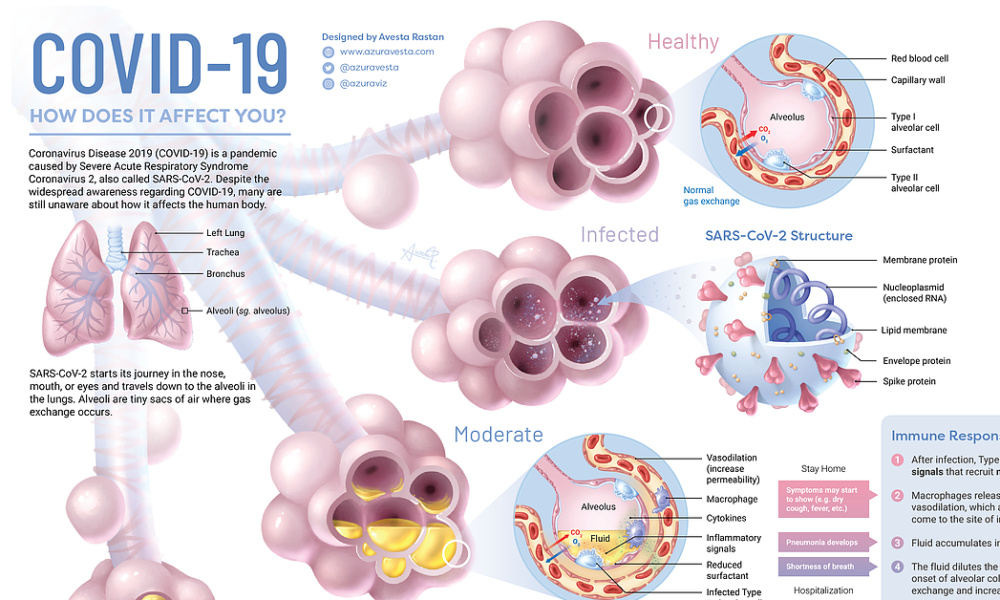 The Wilcoxon and Mann-Whitney tests were used in the case of quantitative variables with non-normal distribution. To compare and track the change of means of quantitative variables that were measured three times during the study period, analysis of variance (ANOVA) with repeated measure was done. Covariance analysis was performed to adjust for quantitative confounding factors.
The Wilcoxon and Mann-Whitney tests were used in the case of quantitative variables with non-normal distribution. To compare and track the change of means of quantitative variables that were measured three times during the study period, analysis of variance (ANOVA) with repeated measure was done. Covariance analysis was performed to adjust for quantitative confounding factors.
The IRCT number was 201110187836N1
In this study, 6 out of 44 patients were excluded voluntarily or due to lack of medication. Therefore, 21 patients in the group receiving zinc supplements and 17 in the placebo group remained in the study (). Furthermore, when serum zinc concentration was assessed, one subject was dropped out in zinc group due to loss of blood sample. The mean age in the zinc group was 37±9 and in the placebo group was 37.5±8 years, which was not significantly different.
Open in a separate window
Flow chart of the study
The two groups were alike with respect to gender, education level, income, smoking, and no significant difference was observed between them (). Both groups received the same SSRI antidepressants. Furthermore, the groups were statistically similar in terms of sleep duration, physical activity, weight, BMI, and serum zinc concentration during the study ().
Both groups received the same SSRI antidepressants. Furthermore, the groups were statistically similar in terms of sleep duration, physical activity, weight, BMI, and serum zinc concentration during the study ().
Table 1
General characteristics of Zinc and Placebo groups
| Variables | Zinc group (n = 21) n (%) | Placebo group (n = 17) n (%) | |
|---|---|---|---|
| Gender | Female | 20(95%) | 14(82%) |
| Male | 1(5%) | 3(18%) | |
| Education Level | Elementary school | 3(14%) | 5(29%) |
| Secondary school | 8(38%) | 2(12%) | |
| High school | 7(34%) | 5(29. 5%) 5%) | |
| Academic | 3(14%) | 5(29.5%) | |
| Smoking | No | 18(86%) | 15(88%) |
| Yes | 3(14%) | 2(12%) | |
| Marital Status | Single | 2(9.50%) | 2(12%) |
| Married | 19(90. 50%) 50%) | 15(88%) | |
| Income | Less than 200 thousand | 2(9%) | 1(6%) |
| 200 to 400 thousand | 6(29%) | 2(12%) | |
| 400 to 600 thousand | 7(33%) | 10(59%) | |
| More than 600 thousand | 6(29%) | 4(23%) |
Open in a separate window
Table 2
Mean and standard deviation of sleep duration, physical activity, anthropometric indices and serum zinc concentration in patients with depression receiving zinc supplementation or placebo
| Variables | Study groups | N | Study period | ||
|---|---|---|---|---|---|
| | |||||
| Baseline | Sixth Week | Twelfth week | |||
| Sleep duration (hours per day) | Zinc Placebo | 21 17 | 7±1 7±1 | 7±1 7±1 | 7±1 7±1 |
| Physical activity (d/MET/h) | Zinc Placebo | 21 17 | 16. 5±3 5±318±3 | 17±3 18±4 | 17±3 18±3 |
| Weight (kg) | Zinc Placebo | 21 17 | 71±17 68.5±10 | 72±17.5 69±10 | 71±18 70±10.5 |
| Height (cm) | Zinc Placebo | 21 17 | 161±6 162±9 | - - | - - |
| BMI (kg/m 2) | Zinc Placebo | 21 17 | 27±6 26±5 | 28±7 26±5 | 27. 5±6 5±627±5 |
| Serum zinc concentration (µg/dL) | Zinc Placebo | 20† 17 | 100±15 106±17 | - - | 107±11 106±14 |
Open in a separate window
†When serum zinc concentration was assessed, one subject was dropped out in zinc group due to loss of blood sample
No significant difference was observed between the two groups regarding dietary intake of energy, carbohydrate, protein, cholesterol, and fiber (). However, intake of total fat, saturated fatty acids and Monounsaturated Fatty Acids (MUFA) in the zinc group was significantly lower in the sixth week (p < 0.05) and twelfth week (P < 0.01) compared to the placebo group(). Also, intake of Polyunsaturated Fatty Acids (PUFA) was significantly lower in the zinc group compared to the placebo group in the twelfth week (p < 0.05) ().
Also, intake of Polyunsaturated Fatty Acids (PUFA) was significantly lower in the zinc group compared to the placebo group in the twelfth week (p < 0.05) ().
Table 3
Mean and standard deviation of energy intake, dietary macronutrients and fiber in patients with depression receiving zinc supplementation or placebo
| Variables (Energy and food components) | Study groups | N | Study period | ||
|---|---|---|---|---|---|
| | |||||
| Baseline | Sixth Week | Twelfth week | |||
| Total energy intake (Kcal/d) | Zinc Placebo | 21 17 | 1667±261 1787±259 | 1686±425 1819±239 | 1665±433 1851±289 |
| Total carbohydrate intake (g /d) | Zinc Placebo | 21 17 | 251±53 240±62 | 280±49 259±53 | 272±42 261±62 |
| Total protein intake (g / d) | Zinc Placebo | 21 17 | 57±19 66±23 | 58±17 63±23 | 60±11 67±27 |
| Total fat intake (g / d) | Zinc Placebo | 21 17 | 49±26 59±33 | 46±16a 65±34 | 46±15 b 65±21 |
| Saturated fatty acid intake (g / d) | Zinc Placebo | 21 17 | 17±8 21±7 | 18±6a 24±9 | 17±6 a 25±9 |
| MUFA fatty acids intake (g / d) | Zinc Placebo | 21 17 | 13±6 16±7 | 13±4a 18±8 | 13±4 b 19±5 |
| PUFA fatty acid intake (g / d) | Zinc Placebo | 21 17 | 9±14 18±24 | 9±8 17±25 | 8±7 a 17±17 |
| Cholesterol intake (g / d) | Zinc Placebo | 21 17 | 224±120 254±152 | 178±87 208±153 | 210±131 238±177 |
| Fiber intake (g / d) | Zinc Placebo | 21 17 | 13±5 14±4 | 16±4 14±4 | 14±3 13±4 |
Open in a separate window
For comparison in each group paired t-test and for comparison between two groups independent sample t-test was used. Statistically significant difference compared with Placebo
Statistically significant difference compared with Placebo
ap < 0.05
bp < 0.01
During the study, dietary intakes of micronutrients such as zinc, magnesium, iron, vitamins B1, B2, B3, B6, B12 and folic acid were not significantly different between the two groups (). Only dietary intake of magnesium in the group receiving zinc supplementation was significantly lower (p < 0.05) than the placebo group at the baseline ().
Table 4
Mean ± SD dietary micronutrient intake in patients with depression receiving zinc supplementation or placebo
| Variables (Energy and food components) | Study groups | N | Study period | ||
|---|---|---|---|---|---|
| | |||||
| Baseline | Sixth Week | Twelfth week | |||
| Zinc intake (mg/d) | Zinc Placebo | 21 17 | 6. 5±2.1 5±2.17.6±2.2 | 7.5±1.7 7.4±2.5 | 7.5±1.7 7.3±2.5 |
| Magnesium intake (mg/d) | Zinc Placebo | 21 17 | 193±55a 249±75 | 227±63 255±83 | 234±85 254±63 |
| Iron intake (mg / d) | Zinc Placebo | 21 17 | 11±4 13±4 | 12.5±5 13±4 | 12±4 13±4 |
Vit. B 1intake (mg / d) B 1intake (mg / d) | Zinc Placebo | 21 17 | 1.4±0.5 1.7±0.5 | 1.5±0.5 1.7±0.4 | 1.6±0.4 1.5±0.3 |
| Vit. B 2intake (mg / d) | Zinc Placebo | 21 17 | 1.2±0.4 1.5±0.5 | 1.5±0.6 1.5±0.7 | 1.5±0.5 1.4±0.4 |
| Vit. B 3intake (mg / d) | Zinc Placebo | 21 17 | 17±5 18±5 | 17±6 18±5 | 18±5 19±8 |
Vit. B 6intake (mg / d) B 6intake (mg / d) | Zinc Placebo | 21 17 | 1.5±0.8 1.5±0.4 | 1.5±0.6 1.5±0.3 | 1.5±0.6 1.6±0.4 |
| Folic acid intake (µg / d) | Zinc Placebo | 21 17 | 198±119 246±114 | 239±110 234±130 | 228±106 270±120 |
| Vit. B 12intake (µg / d) | Zinc Placebo | 21 17 | 2±1. 2 22±0.9 | 2.4±1.4 2.6±1.4 | 2.6±1.1 2.7±1.8 |
Open in a separate window
Statistically significant difference compared with Placebo
ap < 0.05
* Vit.= Vitamin
The Beck score decreased in the placebo group, but this reduction was not significant compared to the baseline. Depression scores decreased significantly in the zinc group in the sixth week (P < 0.01), and the twelfth week of the study (P < 0.001) compared to the baseline, but this difference was not statistically significant compared to the 6th and 12th week values.
At the end of the study, Beck scores was significantly lower (p < 0.05)in zinc group compared with the group receiving the placebo. Even after adjusting for the effect of dietary confounding factors, including intake of total fat, saturated fatty acids, MUFA and PUFA fatty acids and magnesium, this difference still remained significant ().
Open in a separate window
Changes in mean Beck depression scores in the groups receiving zinc compared with placebo using ANOVA with repeated measure. * Statistically significant difference compared with Placebo after 90 day: p < 0.05
Zinc is an essential micronutrient which is responsible for the different biological roles. Some of these functions are involvement in some enzymes activation, gene expression, synthesis and release of insulin, and cardiovascular homeostasis. The amount of zinc stored in the adults’ body is 2-3 grams; most of which, is in skeletal muscle and bone. Only 0.1% of the total zinc pool is present in plasma. The plasma levels of zinc are used to evaluate the nutritional status of zinc (10).
In the present study, mean serum zinc concentration in the group receiving zinc supplements increased by 6.5 µg/dL. However, this increment was not significant compared with placebo. Mean serum zinc concentrations at baseline were 100 ±15 and 106 ±17 µg/dl in the zinc and placebo groups, respectively. These amounts were similar to the mean serum zinc concentrations in healthy adults in Shiraz 104 ±18 µg/dL (11), and Ahvaz (7)111 ± 18 µg/dL, respectively. Some studies have shown the low serum zinc levels in depressed patients which are resistant to treatment (12, 13).Other studies have also shown that low serum zinc levels are normalized during treatment with antidepressants (14) which is consistent with our findings. In the present study, the mean dietary zinc intake in patients with major depression was about 6.5-7 mg per day. While in the study of Ghasemi and colleagues, the mean dietary zinc intake in men and women were 15.8 ± 11 and 14.7 ± 11 mg/day, respectively (15). The less zinc intake in these patients may be due to some antidepressants and lack of appetite as one of the symptoms of depression. Serum zinc level was normal in the current study. Therefore, despite the low intakes of zinc, we can infer that the increased serum zinc up to normal levels may be due to antidepressants.
These amounts were similar to the mean serum zinc concentrations in healthy adults in Shiraz 104 ±18 µg/dL (11), and Ahvaz (7)111 ± 18 µg/dL, respectively. Some studies have shown the low serum zinc levels in depressed patients which are resistant to treatment (12, 13).Other studies have also shown that low serum zinc levels are normalized during treatment with antidepressants (14) which is consistent with our findings. In the present study, the mean dietary zinc intake in patients with major depression was about 6.5-7 mg per day. While in the study of Ghasemi and colleagues, the mean dietary zinc intake in men and women were 15.8 ± 11 and 14.7 ± 11 mg/day, respectively (15). The less zinc intake in these patients may be due to some antidepressants and lack of appetite as one of the symptoms of depression. Serum zinc level was normal in the current study. Therefore, despite the low intakes of zinc, we can infer that the increased serum zinc up to normal levels may be due to antidepressants. The antidepressants may stimulate releasing zinc from the body's stores such as muscles and bones. Also, zinc supplementation on these patients has restored the zinc pools.
The antidepressants may stimulate releasing zinc from the body's stores such as muscles and bones. Also, zinc supplementation on these patients has restored the zinc pools.
Studies on dietary factors and their relation to depression have shown that consumption of meals containing high amounts of carbohydrates cause insulin release. Insulin causes glucose entrance into the cells, and on the other hand make more amino acids such as tryptophan to cross the blood - brain barrier. This may increase neurotransmitter levels, especially serotonin, in the brain which can lead to improved mood (16). Amino acid tryptophan can be converted to serotonin in the body and can cause sleep and mental calmness (17). Tyrosine amino acid can be synthesized from the amino acid phenylalanine and may enter into the biochemical pathways of dopamine and norepinephrine (18). Dietary omega-3 fatty acids are provided from some especial plant and animal sources (especially some marine animals). Omega-3 fatty acids are involved in regulating corticotropin factor, stimulating the serotonergic pathway, preventing neuronal apoptosis, improving blood flow to the brain and regulating gene expression (19). Folate and B12 deficiency are associated with depression. About 10 to 30% of depressed patients have low serum folate levels and their response to antidepressants is weak. Early vitamin B12 deficiency leads to depression. This is due to the reduced synthesis of S-Adenosyl Methionine (20). S-Adenosyl Methionine is associated with mood. The low concentrations in cerebrospinal fluid of depressed patients have been observed and it was found that increasing its plasma concentrations have improved the depressive symptoms (21). So far, clinical trials published in this field have not assessed the mentioned dietary confounding factors. However, the present study was the first experiment which evaluated the effects of dietary confounding factors in patients with depression. As shown in the results, the effects of dietary factors on depression during the study were similar between the two groups. In cases where there was statistical difference between the two groups, the confounding effects were adjusted using ANCOVA.
Folate and B12 deficiency are associated with depression. About 10 to 30% of depressed patients have low serum folate levels and their response to antidepressants is weak. Early vitamin B12 deficiency leads to depression. This is due to the reduced synthesis of S-Adenosyl Methionine (20). S-Adenosyl Methionine is associated with mood. The low concentrations in cerebrospinal fluid of depressed patients have been observed and it was found that increasing its plasma concentrations have improved the depressive symptoms (21). So far, clinical trials published in this field have not assessed the mentioned dietary confounding factors. However, the present study was the first experiment which evaluated the effects of dietary confounding factors in patients with depression. As shown in the results, the effects of dietary factors on depression during the study were similar between the two groups. In cases where there was statistical difference between the two groups, the confounding effects were adjusted using ANCOVA.
In the present study, zinc supplementation significantly decreased the Beck depression scores compared with the placebo. Findings of this research were similar to the study by Nowak and colleagues on 20 patients with major depression. Nowak supplemented the antidepressants with 25 milligrams of zinc in one group and the other group was given a placebo with antidepressants. Beck depression scale at baseline and the second, sixth and twelfth weeks were measured. Nowak showed that reduction in Beck scores at week 6 and 12 in the group receiving the supplement were significant compared with placebo (22).
In a study on patients with major depression, Siwek and colleagues gave imipramine combined with 25 mg zinc supplement to one group and placebo combined with imipramine to another group. Siwek findings revealed no significant change in depression scores of the two groups. However, zinc supplementation significantly reduced the rate of depression in patients resistant to medication and may facilitate treatment with antidepressants (12). One of the possible causes of the differences in the results of Siwek study with ours may be due to different type of antidepressant medication prescribed.
One of the possible causes of the differences in the results of Siwek study with ours may be due to different type of antidepressant medication prescribed.
Antidepressants may exert their effect through the zinc-containing neurons. Zinc is located in the presynaptic vesicles of neurons of the cortex, amygdala, hippocampus, and spinal cord. These neurons are mainly glutaminergic. The majority of zinc-containing neurons in the spinal cord is gamma-amino butyric acidergic or GAB Aergic and partly Glycinergic; perhaps zinc inhibits glutamate receptors such as N-Methyl-D-Aspartic (NMDA) (23, 24).
Another hypothesis in this field is the role of the protein Brain-Derived Neurotrophic Factor (BDNF). Some recent studies have shown that the BDNF may be involved in mechanism of zinc antidepressant effect. Chronic high doses of zinc increases BDNF gene expression in the cerebral cortex of rats, while a low dose of zinc may increase BDNF gene expression in hippocampus (25, 26).
The limited number of patients did not allow subgroups analysis based on type of SSRI drugs.
The results of this study reveal that zinc supplementation combined with antidepressant drugs can be effective in the treatment of patients with major depression.
We would like to thank the Center for Neuroscience Research for financial support, Imam Hussein Laboratory personnel, and Endocrine Research Center of Shahid Beheshti University of Medical Sciences.
We suggest evaluating the effects of different doses of zinc on depression in future studies.
Authors have nothing to declare.
1. Kleinman A. Culture and depression. N Engl J Med. 2004;351:951–3. [PubMed] [Google Scholar]
2. Dejman M, Ekblad S, Forouzan AS, Baradaran-Eftekhari M, Malekafzali H. Explanatory Model of Help-Seeking and Coping Mechanisms among Depressed Women in Three Ethnic Groups of Fars, Kurdish, and Turkish in Iran. Archives of Iranian medicine. 2008;11:397–406. [PubMed] [Google Scholar]
3. Kaplan H, Sadock B. Synopsis of psychiatry. 8th eds. Williams and Wilkins; 2003. [Google Scholar]
4. Fava M, Davidson KG. Definition and Epidemiology of Treatment-Resistant Depression. The Psychiatric clinics of North America. 1996;19:179–200. [PubMed] [Google Scholar]
Fava M, Davidson KG. Definition and Epidemiology of Treatment-Resistant Depression. The Psychiatric clinics of North America. 1996;19:179–200. [PubMed] [Google Scholar]
5. Hansen CR, Jr, Malecha M, Mackenzie TB, Kroll J. Copper and Zinc Deficiencies in Association with Depression and Neurological Findings. Biological psychiatry. 1983;18:395–401. [PubMed] [Google Scholar]
6. Sandstead HH, Penland JG, Alcock NW, Dayal HH, Chen XC, Li JS, et al. Effects of Repletion with Zinc and Other Micronutrients on Neuropsychologic Performance and Growth of Chinese Children. The American journal of clinical nutrition. 1998;68:470S–475S. [PubMed] [Google Scholar]
7. Amani R, Saeidi S, Nazari Z, Nematpour S. Correlation between Dietary Zinc Intakes and Its Serum Levels with Depression Scales in Young Female Students. Biological trace element research. 2010;137:150–158. [PubMed] [Google Scholar]
8. McLoughlin IJ, Hodge JS. Zinc in Depressive Disorder. Acta psychiatrica Scandinavica. 1990;82:451–453. [PubMed] [Google Scholar]
1990;82:451–453. [PubMed] [Google Scholar]
9. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An Inventory for Measuring Depression. Archives of general psychiatry. 1961;4:561–571. [PubMed] [Google Scholar]
10. Ghasemi A, Zahediasl S, Hosseini-Esfahani F, Azizi F. Reference Values for Serum Zinc Concentration and Prevalence of Zinc Deficiency in Adult Iranian Subjects. Biological trace element research. 2012;149:307–314. [PubMed] [Google Scholar]
11. Dabbaghmanesh MH, Taheri Boshrooyeh H, Kalantarhormozi MR, Ranjbar Omrani GH. Assessment of Zinc Concentration in Random Samples of the Adult Population in Shiraz, Iran. Iranian Red Crescent medical journal. 2011;13:249–255. [PMC free article] [PubMed] [Google Scholar]
12. Siwek M, Dudek D, Schlegel-Zawadzka M, Morawska A, Piekoszewski W, Opoka W, et al. Serum Zinc Level in Depressed Patients During Zinc Supplementation of Imipramine Treatment. Journal of affective disorders. 2010;126:447–452. [PubMed] [Google Scholar]
13. Schlegel_Zawadzka M, Zieba A, Dudek D. Effect of depression and of antidepressant therapy on serum zinc levels- a preliminary clinical study. New York: 2000. [Google Scholar]
Schlegel_Zawadzka M, Zieba A, Dudek D. Effect of depression and of antidepressant therapy on serum zinc levels- a preliminary clinical study. New York: 2000. [Google Scholar]
14. McLoughlin IJ, Hodge JS. Zinc in Depressive Disorder. Acta psychiatrica Scandinavica. 1990;82:451–453. [PubMed] [Google Scholar]
15. Ghasemi A, Zahediasl S, Hosseini-Esfahani F, Azizi F. Reference Values for Serum Zinc Concentration and Prevalence of Zinc Deficiency in Adult Iranian Subjects. Biological trace element research. 2012;149:307–314. [PubMed] [Google Scholar]
16. White JW, Wolraich M. Effect of Sugar on Behavior and Mental Performance. The American journal of clinical nutrition. 1995;62:242S–247S. discussion 247S-249S. [PubMed] [Google Scholar]
17. Buist R. The therapeutic predictability of tryptophan and tyrosine in the treatment of depression. Int J Clin Nutr Rev. 1983;3:1–3. [Google Scholar]
18. Kravitz HM, Sabelli HC, Fawcett J. Dietary Supplements of Phenylalanine and Other Amino Acid Precursors of Brain Neuroamines in the Treatment of Depressive Disorders. The Journal of the American Osteopathic Association. 1984;84:119–123. [PubMed] [Google Scholar]
The Journal of the American Osteopathic Association. 1984;84:119–123. [PubMed] [Google Scholar]
19. Freeman MP, Hibbeln JR, Wisner KL, Davis JM, Mischoulon D, Peet M, et al. Omega-3 Fatty Acids: Evidence Basis for Treatment and Future Research in Psychiatry. The Journal of clinical psychiatry. 2006;67:1954–1967. [PubMed] [Google Scholar]
20. Fava M, Borus JS, Alpert JE, Nierenberg AA, Rosenbaum JF, Bottiglieri T. Folate, Vitamin B12, and Homocysteine in Major Depressive Disorder. The American journal of psychiatry. 1997;154:426–428. [PubMed] [Google Scholar]
21. Bell KM, Potkin SG, Carreon D, Plon L. S-Adenosylmethionine Blood Levels in Major Depression: Changes with Drug Treatment. Acta neurologica Scandinavica. Supplementum. 1994;154:15–18. [PubMed] [Google Scholar]
22. Nowak G, Siwek M, Dudek D, Zieba A, Pilc A. Effect of Zinc Supplementation on Antidepressant Therapy in Unipolar Depression: A Preliminary Placebo-Controlled Study. Polish journal of pharmacology. 2003;55:1143–1147. [PubMed] [Google Scholar]
2003;55:1143–1147. [PubMed] [Google Scholar]
23. Poleszak E, Wlaz P, Wrobel A, Fidecka S, Nowak G. Nmda/Glutamate Mechanism of Magnesium-Induced Anxiolytic-Like Behavior in Mice. Pharmacological reports: PR. 2008;60:655–663. [PubMed] [Google Scholar]
24. Nowak G, Szewczyk B, Sadlik K, Piekoszewski W, Trela F, Florek E, et al. Reduced Potency of Zinc to Interact with Nmda Receptors in Hippocampal Tissue of Suicide Victims. Polish journal of pharmacology. 2003;55:455–459. [PubMed] [Google Scholar]
25. Franco JL, Posser T, Brocardo PS, Trevisan R, Uliano-Silva M, Gabilan NH, et al. Involvement of Glutathione, Erk1/2 Phosphorylation and Bdnf Expression in the Antidepressant-Like Effect of Zinc in Rats. Behavioural brain research. 2008;188:316–323. [PubMed] [Google Scholar]
26. Nowak G, Legutko B, Szewczyk B, Papp M, Sanak M, Pilc A. Zinc Treatment Induces Cortical Brain-Derived Neurotrophic Factor Gene Expression. European journal of pharmacology. 2004;492:57–59. [PubMed] [Google Scholar]
Zinc - ingredient description, instructions for use, indications and contraindications
16 April 2020
15 December 2022
3 minutes ProWellness
Table of Contents
- Zinc Description
- Biological Functions
- Intake Rates
- Zinc Deficiency
- Zinc Overabundance
- Food Sources
- Preventive and Curative Use
- 0029
Disclaimer
Please note that all information posted on the site Prowellness is provided for informational purposes only and is not a personal program, a direct recommendation for action, or medical advice.
 Do not use these materials for diagnosis, treatment, or any medical procedure. Consult your physician before using any technique or using any product. This site is not a specialized medical portal and does not replace the professional advice of a specialist. The Site Owner is not liable to any party who has suffered indirect or direct damage as a result of misuse of materials posted on this resource.
Do not use these materials for diagnosis, treatment, or any medical procedure. Consult your physician before using any technique or using any product. This site is not a specialized medical portal and does not replace the professional advice of a specialist. The Site Owner is not liable to any party who has suffered indirect or direct damage as a result of misuse of materials posted on this resource. Description of zinc
Zinc is a trace element present in the body as part of more than 300 hormones and enzymes and performs vital functions.
Zinc accumulates in cells, hair, muscles, skin, bones. The total mass of the element in the human body is small - from 1.5 to 3 g. However, its importance for humans can hardly be overestimated.
Biological functions
Zinc is found in every cell of the body. It is important for the synthesis of DNA, RNA, carbohydrates, fats, proteins.
 Influences the activity of more than 300 enzymes that are involved in metabolism, nervous function, digestion and many other processes.
Influences the activity of more than 300 enzymes that are involved in metabolism, nervous function, digestion and many other processes. Without this trace element, the full development of immune cells and cell division is impossible. With its deficiency, the skin, digestive, nervous, reproductive, hematopoietic, and immune systems suffer.
In addition to the listed functions, zinc:
- important for prostate health;
- stimulates tissue regeneration;
- is required for insulin production;
- improves the absorption of tocopherol;
- is responsible for dental health;
- eliminates inflammatory processes;
- ensures the correct structure of the ribosome;
- normalizes the functioning of the liver;
- improves the condition of the organs of vision.
Zinc reduces oxidative stress and lowers the risk of pneumonia, macular degeneration, infections. It is involved in collagen synthesis, immune and inflammatory response, so it is used in the treatment of ulcers and burns.
Attention! Zinc can be used to treat acne. They inhibit inflammatory responses, sebaceous gland activity, and the growth of propionibacterium acne. Numerous studies have shown that people with acne are often deficient in zinc.
Consumption rates
A new portion of zinc is needed by the body every day, since it does not have a depot for its storage. The daily intake of a trace element for infants is 0.8 mg, for children - 3-10 mg, for adults - 15 mg, for pregnant women - 25 mg.
Zinc deficiency
With a micronutrient deficiency, the following symptoms are observed:
- feeling nervous;
- sleep is disturbed;
- no appetite;
- reduced visual acuity;
- anemia develops;
- nail plates are affected;
- depression occurs;
- mental disorders are manifested;
- dandruff develops;
- hair falls out;
- testosterone level drops;
- potency worsens;
- skin diseases occur.
Zinc excess
An overdose of zinc is accompanied by nausea, anemia, intestinal colic, vomiting, bloody diarrhea, impaired kidney function, a metallic taste in the mouth, and jaundice.
Food sources
Leading foods for zinc are oysters, pumpkin and sesame seeds, beef, lentils, cereals, almonds, walnuts, peanuts, chicken, and pork. In addition, zinc ions are found in fish, vegetables, berries, dried fruits, fruits, and milk.
Prophylactic and curative use
Zinc preparations are available in the form of capsules, tablets, ointments, solutions, pops and chewable lozenges, drops for oral administration. The active substance is included in the form of oxide, sulfate, citrate or acexamate.
The optimal prophylactic zinc dosage is 8 mg for women and 11 mg for men. If the micronutrient is used to treat various conditions, the doses are increased.
 For example, with acne - 135 mg, with problems with conception - 50 mg, with a cold - 150 mg.
For example, with acne - 135 mg, with problems with conception - 50 mg, with a cold - 150 mg. Attention! Zinc is taken one hour before meals or 2 hours after meals. You can not combine it with antibiotics.
Disclaimer
Please note that all information posted on the site Prowellness is provided for informational purposes only and is not a personal program, a direct recommendation for action, or medical advice. Do not use these materials for diagnosis, treatment, or any medical procedure. Consult your physician before using any technique or using any product. This site is not a specialized medical portal and does not replace the professional advice of a specialist. The Site Owner is not liable to any party who has suffered indirect or direct damage as a result of misuse of materials posted on this resource.
Zinc is an indispensable trace element for the human body
Already in 1963, the importance of zinc for human health and life was not in doubt, although at that time only three intestinal enzymes were known to science, for which zinc acts as a cofactor.
 Today we know about more than 300 enzymes and more than 100 transcription factor variants in which zinc acts as a cofactor.
Today we know about more than 300 enzymes and more than 100 transcription factor variants in which zinc acts as a cofactor. Zinc can be deposited in the human body in limited quantities, and therefore, to maintain its vital level, it is necessary to systematically consume foods or biologically active food supplements containing zinc.
About 2 billion people suffer from chronic zinc deficiency. This is usually associated with an unbalanced diet and excessive consumption of cereals containing phytic acid salts. Zinc deficiency can be caused by the presence of malabsorption syndrome and sickle cell anemia, among other diseases, as well as chronic damage to the liver and kidneys. Other reasons include pregnancy, breastfeeding, veganism (complete refusal of food of animal origin) and alcohol dependence.
Chronic zinc deficiency leads to stunted growth in children, immunodeficiency and cognitive impairment. Reduced immunity is accompanied by frequent repeated infectious diseases, which significantly reduces a person's life expectancy.
 In addition, sensitivity to infectious agents increases, the incidence of dermatitis increases, and the rate of wound healing slows down. In particular, it is worth noting that in the elderly, a lack of zinc causes inhibition of protein biosynthesis, leading to a decrease in the amount of muscle and an increase in adipose tissue.
In addition, sensitivity to infectious agents increases, the incidence of dermatitis increases, and the rate of wound healing slows down. In particular, it is worth noting that in the elderly, a lack of zinc causes inhibition of protein biosynthesis, leading to a decrease in the amount of muscle and an increase in adipose tissue. Health benefits. Systemic effects
Zinc is an effective immunostimulant. It acts as a "second messenger" of immune cells and significantly reduces the duration of colds. In addition, a sufficient supply of zinc to the visual structures ensures the correct perception of light stimuli on the retina and reduces the risk of developing age-related macular degeneration.
The antioxidant effect of zinc plays a critical role in reducing oxidative stress, which can cause DNA damage, and thus, this microelement reduces the risk of cancer.
Chronic zinc deficiency leads to or exacerbation of neurological and psychiatric disorders such as depression and schizophrenia, as well as neurodegenerative diseases such as Alzheimer's disease, Parkinson's disease or amyotrophic lateral sclerosis.
The key role of zinc in the synthesis of testosterone and in spermatogenesis has long been known, from which we can conclude that this trace element is necessary for men during sexual activity.
Antibacterial effect
Zinc's anti-inflammatory, wound healing, antioxidant and antibacterial effects make it versatile as an additive in personal care, skin and oral care products.
For example, preparations containing zinc salts and, in particular, zinc oxide are used to treat various forms of acne. Note that the effectiveness directly depends on the size of the salt particles: the smaller it is, the more it inhibits the growth of bacteria.
Zinc-containing sunscreen products help to reduce the oxidative stress associated with intense sun exposure. At the same time, micronized zinc oxide effectively absorbs and reflects long-wave UVA radiation, additionally creating physical protection for the skin.
The addition of zinc salts to toothpaste or mouthwash provides protection of the chewing surface of the teeth up to 2-3 hours after application due to the binding of saliva elements and bacterial membranes to the mucous membranes.